Article Text

Statistics from Altmetric.com
Dual-track assessment directs research ethics committees (RECs) to assess the risks of research interventions based on the unclear distinction between therapeutic and non-therapeutic interventions. The net risks test, in contrast, relies on the clinically familiar method of assessing the risks and benefits of interventions in comparison to the available alternatives and also focuses attention of the RECs on the central challenge of protecting research participants.
Research guidelines around the world recognise that clinical research is ethical only when the risks to participants are reasonable.1 Appropriate implementation of this requirement is vital to protecting research participants and allowing research to proceed when it poses acceptable risks. Unfortunately, as the US National Bioethics Advisory Commission (NBAC) notes: “current regulations do not further elaborate how risks and potential benefits are to be assessed, and little additional guidance is available to IRBs.”1
The NBAC, as well as numerous commentators, recommend that research ethics committees (RECs), ethics review committees and institutional review boards (IRBs) should adopt what may be called dual-track risk assessment.2–5 Yet, dual-track assessment unnecessarily divides research interventions into two different categories before assessing their risks and relies on the unclear distinction between therapeutic and non-therapeutic interventions. As a result, dual-track assessment provides RECs with confusing guidance and has the potential to block valuable research that poses acceptable risks. This paper describes one alternative, the net risks test, and argues that this approach offers a better method for assessing research risks, one that puts RECs in a position to protect participants without blocking appropriate research studies.
BACKGROUND
Clinical research exposes participants to interventions and procedures to gather systematic data that may be used to improve overall health and well-being. To ensure that research is ethical, RECs must ensure that the risks and burdens to participants are not excessive and that they are justified by the potential clinical benefits to participants, if any, and the social value of the knowledge to be gained from the research. To make this determination, it is widely agreed that RECs should assess the risks of the individual research interventions and procedures that make up a given study. This process of assessing individual interventions and procedures is sometimes called “component analysis”.
Importantly, not all research risks are ethically worrisome. Even serious risks may ethically be acceptable when the evidence suggests that the intervention in question—for example, an experimental treatment—offers participants a compensating potential for clinical benefit. The risks of undergoing a biopsy purely for research purposes, in contrast, are worrisome because participants are not offered a compensating potential for clinical benefit. This difference suggests that to protect research participants, RECs should assess whether the risks of a given research intervention exceed its potential for clinical benefit. For simplicity, we will refer to the risks of undergoing an intervention that exceed its potential for clinical benefit as the net risks of that intervention.
No regulatory consensus exists on the upper limit on the net research risks to which competent adults may be exposed. The US federal regulations do not mandate any limit on the net research risks to which competent adults may be exposed. Hence, in principle at least, these regulations allow competent adults to be exposed to serious net research risks as long as the risks are justified by the societal value of the research. The most prominent exception to this general rule is the Nuremberg Code, which prohibits research when there is “a prior reason to believe that death or disabling injury will occur”.6
In contrast with the lack of consensus on whether there should be an a priori limit on the net risks to which competent adults may be exposed, research regulations around the world agree that people who are unable to provide their own informed consent should be enrolled in research only when the net risks are minimal or, at most, a minor increase over minimal. Here again, the Nuremberg Code offers a noteworthy exception stating that informed consent of research participants is essential to ethical research, implying that research with people who cannot consent is unethical.
Most regulations define minimal risks on the basis of the risks of daily life. On this standard, an intervention qualifies as minimal risk when its risks are no greater than those risks that people face in daily life. To implement this standard, RECs need a way to assess the risks of research interventions and procedures.
DUAL-TRACK ASSESSMENT
Some commentators and guidelines direct RECs to assess research risks by first categorising the interventions included in a given study into two different categories, typically labelled therapeutic and non-therapeutic interventions (fig 1). Although this approach is sometimes labelled component analysis, it offers a substantive addition to components analysis understood as the requirement that RECs assess the risks of individual research interventions and procedures. Specifically, the present approach specifies one way in which RECs may assess these research interventions. To avoid confusing the process of assessing individual interventions with distinct recommendations for how RECs should assess them, we will refer to the approach under consideration here as dual-track assessment.
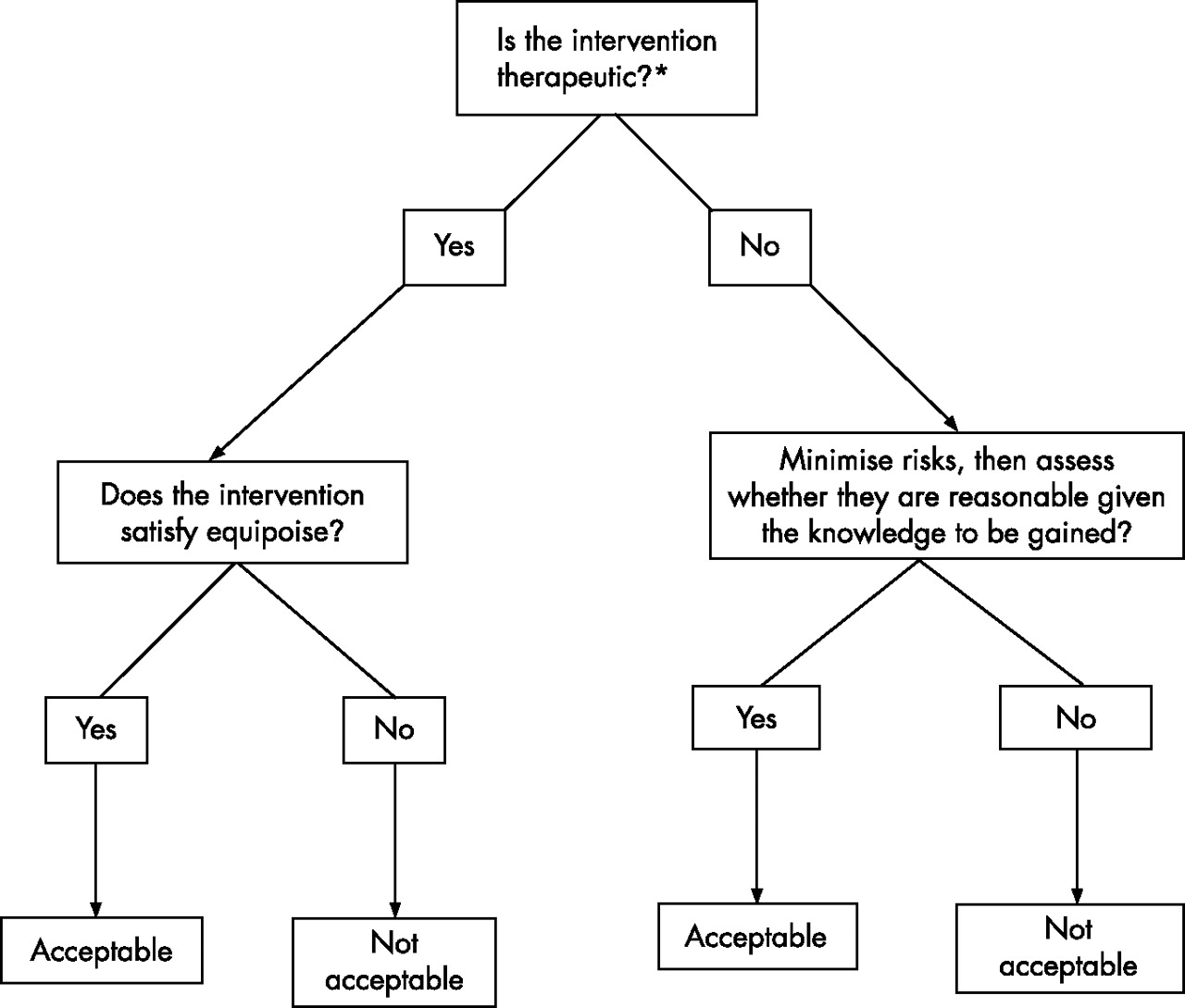
Dual-track assessment of individual interventions. *Therapeutic interventions are defined variously as ones designed to benefit participants, ones intended to benefit participants or ones given with therapeutic warrant.
According to dual-track assessment, RECs may approve therapeutic interventions only when they satisfy clinical equipoise—that is, only when there is “disagreement in the community of expert practitioners”5 about whether the intervention is in the medical interests of participants, in the sense that its risk–benefit profile is at least as promising for participants as the established standard of care. Dual-track assessment prohibits RECs from approving interventions that are categorised as therapeutic when they are not in the medical interests of participants, even when the social value to be gained from the procedures is important and the risks to participants are very low.
In contrast, dual-track assessment allows RECs to approve interventions such as blood draws to measure study outcomes, which are categorised as non-therapeutic even when they are not in the medical interests of participants. Unlike therapeutic interventions, dual-track assessment allows the risks of non-therapeutic interventions to be justified by the social value to be gained by including them in the study. One way to evaluate dual-track assessment, then, is to ask whether this difference in the assessment of the risks of therapeutic and non-therapeutic interventions is clear and justified.
CONCERNS ABOUT DUAL-TRACK ASSESSMENT
Unnecessary use of two ethical standards
The central goal of assessing the risks of research interventions is to ensure that they do not expose participants to excessive risks. To make this determination, dual-track assessment directs RECs to first divide the interventions under review into two different categories. Although this process adds complexity to risk assessments by RECs, proponents of dual-track assessment fail to explain why the use of two different categories is necessary to protect research participants.
One may assume that this distinction is needed to protect research participants from excessive risks. We have, however, found no reason to think that it is always ethically unacceptable for so-called therapeutic interventions to pose net risks to research participants, whereas non-therapeutic interventions that pose net risks can be ethically justified. Without an explanation for why the net risks of these two types of interventions have different ethical status, the dual-track approach seems to add complexity without increasing protection for research participants.
Proponents may reason that patients typically undergo therapeutic interventions, whereas non-therapeutic interventions are used typically in research with healthy volunteers. One may assume patients deserve greater protection, either because they are more vulnerable or because they are more likely to suffer from the so-called therapeutic misconception, failing to distinguish between research and clinical care. The principal problem with this defence is that many research studies include both therapeutic and non-therapeutic procedures. In particular, most treatment trials include interventions, such as blood draws, that are included purely for scientific reasons, suggesting that patients who participate in clinical research typically undergo both types of interventions.
Lack of a clear definition
Some commentators define non-therapeutic interventions as those designed to “achieve beneficial results for the public”.7 As all research is designed to benefit the public, this definition has the potential to categorise all research interventions as non-therapeutic. Hence, the risks of all interventions may have to be justified by their social value alone. By this definition, then, dual-track assessment would have the potential to inadvertently prohibit research interventions, the risks of which are justified by their potential benefits to participants.
Others distinguish between therapeutic and non-therapeutic interventions on the basis of the intentions of the investigators.2 The US NBAC2 states that research interventions qualify as non-therapeutic when “their sole intent is to answer the research question(s)”. Similarly, Weijer8 states that “Therapeutic and non-therapeutic procedures are, by definition, administered with differing intent. This difference is morally relevant.” Unfortunately, investigators often have mixed intentions, aiming at benefiting both participants and society. Even in research with healthy volunteers, researchers often attempt to benefit participants, for example, by informing them of any research findings that may be of clinical significance. Hence, this definition fails to provide RECs with a clear method distinguishing between therapeutic and non-therapeutic interventions.
Finally, some proponents of the dual-track approach appeal to the concept of therapeutic warrant, defining interventions as therapeutic when they are “administered with evidence sufficient to justify the belief that they may benefit research subjects”. The therapeutic warrant approach then defines interventions as non-therapeutic provided they are “administered solely for the purpose of answering the scientific question”.5
By defining non-therapeutic interventions on the basis of the “purpose” of administering them, this definition seems to appeal either to research design or to investigator intention. As a result, this definition fails to avoid the problems mentioned earlier: all research interventions are designed to answer scientific questions, and investigators typically have multiple intentions when administering research interventions.
Secondly, defining therapeutic interventions as those that may benefit participants has the potential to create further confusion. Many research interventions offer a very low chance of benefit to participants. Radiological scans conducted in healthy volunteers for research purposes seem to offer a paradigm example of a non-therapeutic intervention. Yet, data provide compelling evidence that research scans conducted in healthy volunteers offer a small chance of identifying an undiagnosed and treatable brain tumour,9 showing that this definition may lead RECs to categorise all research interventions as therapeutic.
Thirdly, the two clauses that make up the therapeutic warrant definition are not mutually exclusive. Interventions may be administered for scientific purposes, even when there is evidence that they have the potential to benefit participants, implying that most interventions would qualify as both therapeutic and non-therapeutic. This result is problematic, given that the dual-track approach applies conflicting requirements to therapeutic and non-therapeutic interventions: therapeutic interventions must satisfy the requirement of clinical equipoise, whereas non-therapeutic interventions do not have to satisfy this requirement. It is unclear how RECs are supposed to assess those research interventions, possibly the majority of research interventions, which qualify as therapeutic and non-therapeutic.
The consequences of this problematic result are exemplified by the NBAC’s use of the dual-track approach. The NBAC states that RECs should categorise individual research interventions into those “designed solely to answer the research question(s)” and those that “offer the prospect of direct benefit to participants”. The NBAC then reasons that RECs should use different standards to assess these interventions. Interventions designed solely to answer the research question are to be assessed on the basis of whether the risks “are reasonable in relation to potential benefits of knowledge”. Interventions offering direct benefit to participants are to be judged on the basis of whether “the risks are reasonable in relation to potential benefits to participants”.
This approach suffers from the concerns stated earlier. It relies on the unclear distinction between therapeutic and non-therapeutic interventions and unnecessarily advocates different ethical standards for the risks posed by the two different types of interventions. The two categories included in the NBAC approach are also not mutually exclusive—a serious concern for RECs, given that the standards endorsed for the two categories are mutually exclusive.
As the previous example of research scans shows, many research interventions are designed solely to answer the scientific question and also offer some prospect of clinical benefit to participants. This is also true of many, perhaps most, screening tests used in clinical research. These tests are included in research studies solely for scientific reasons, to determine whether prospective participants qualify for research enrolment. Yet, these tests often offer some potential for clinical benefit. Routine screening can reveal undiagnosed conditions, such as cardiac arrhythmias, low blood sugar and high blood pressure. These examples show that whether interventions offer the potential for clinical benefit depends on the possible consequences of undergoing the interventions, not on investigators’ intentions in administering them.
The practical difficulties posed by the lack of a clear definition of therapeutic and non-therapeutic interventions are exemplified by assessment of the risks of placebo controls. In most research trials, placebo controls are used strictly for scientific purposes, as a way to control for improvements that are not due to the intervention being tested. This suggests that placebo controls qualify as non-therapeutic interventions. Yet, one of the leading proponents of dual-track assessment seems to disagree: “A placebo control is at least a no-treatment control. A no-treatment control is the null case for therapeutic procedures and it, along with therapeutic procedures in the experimental arm, must pass the test of clinical equipoise.” The introduction here of the concept of the null case for therapeutic procedures, which would seem to imply that such procedures are not therapeutic, highlights the confusion that arises when we attempt to apply dual-track assessment to actual cases.
Lack of familiarity
Many research regulations make no mention of the therapeutic or non-therapeutic distinction, relying instead on distinctions such as whether the interventions offer participants a “prospect of direct benefit”. To implement the dual-track approach, RECs would have to reconcile a method that relies on the distinction between therapeutic and non-therapeutic interventions, with regulations that do not include this distinction. In particular, RECs would have to synthesise the concept of prospect of direct benefit, which focuses on the effect of research on participants with the therapeutic or non-therapeutic distinction, which, depending on the preferred definition, focuses on investigators’ intentions or the design of individual interventions.
Arbitrary judgements
Dual-track assessment allows RECs to approve non-therapeutic interventions that are not in the medical interests of the participants, provided the risks are sufficiently low and the knowledge to be gained justifies the risks. In contrast, dual-track assessment prohibits RECs from approving therapeutic interventions that are not in the medical interests of the participants, even when the risks are just as low or even lower, and the knowledge to be gained justifies the risks. A leading advocate of dual-track assessment writes:
Therapeutic procedures are those study interventions administered with therapeutic intent. The Institutional Review Board (IRB) must ensure that such procedures fulfill the requirements of clinical equipoise…Nontherapeutic procedures are not administered with therapeutic warrant…the IRB must ensure that the risks associated with such procedures are 1) minimized and 2) reasonable in relation to the knowledge to be gained.10
To assess the pathophysiology of depression, investigators sometimes need to carry out brain scans and other non-invasive procedures on people who are diagnosed with depression and are not taking drugs. These scans are designed purely for scientific purposes and are not intended to treat the depression in patients. In addition, the low chance of clinical benefit from these scans typically does not justify the risks and burdens of undergoing them, implying that these interventions qualify as non-therapeutic, whether we endorse the design, intent or therapeutic warrant definition. It follows on the dual-track approach that these procedures do not have to satisfy clinical equipoise. Whether they are acceptable depends on whether they pose excessive risks to participants, and in particular on whether the delay in receiving standard medically indicated treatment while people are on the study entails excessive risk.
In contrast, dual-track assessment would not allow the same people to enrol in a clinical trial evaluating an experimental treatment for depression that included a non-treatment arm, even when the length of time off treatment, the risks and the social value of the study are exactly the same as in the non-therapeutic, pathophysiology study. This study qualifies as therapeutic and hence would have to satisfy the requirement of clinical equipoise.
This difference in judgement seems ethically arbitrary. It is not justified by the primary goal of risk assessment—namely, protecting participants from excessive risks. If it is acceptable to expose competent adults to these risks, then both studies seem acceptable. Conversely, if we think that it is ethically unacceptable to expose people to these risks for the benefit of society, both studies would be unacceptable. Claiming that RECs should be allowed to approve the one type of study, but not the other, on the basis of the (unclear) distinction between therapeutic and non-therapeutic interventions is not justified.
Furthermore, as the above quote makes clear, dual-track assessment mandates that investigators and RECs should minimise the risks of non-therapeutic interventions, but does not make the same requirement for therapeutic interventions. This seems an important mistake that is perhaps encouraged by categorising some research procedures as therapeutic. For example, a randomised treatment trial may compare a new treatment to the standard of care. Dual-track assessment would allow this study to be approved, provided there is clinical equipoise between the two arms of the trial. Dual-track assessment would not require that the risks of the experimental treatment be minimised, provided it satisfies equipoise—an omission that may unnecessarily increase the risks to research participants.
THE NET RISKS TEST
To ensure that research participants are not exposed to excessive risks, RECs should minimise the risks of all interventions included in the study under review, consistent with sound scientific design. RECs then need a method that allows them to assess the ethical acceptability of the remaining risks to participants. In particular, RECs need a method to ensure that research interventions do not pose excessive net risks.
At least two scenarios exist in which research interventions pose net risks to participants. Most obviously, this happens when the risks of the interventions exceed their potential clinical benefits. A research blood draw that offers participants no potential for benefit poses net research risks, represented by all the risks that participants face from the blood draw. In addition, research interventions that have a favourable profile of risks to potential clinical benefits nonetheless pose net research risks when their risk–benefit profile is less favourable to participants than one or more of the available alternatives.
Investigators sometimes use older-generation drugs that have different mechanisms of action than current treatments to better understand the aetiology of certain diseases. Typically, the potential clinical benefits of older drugs exceed their risks. Administration of the older treatment poses net research risks if participants are precluded from receiving the newer treatment that offers a more favourable risk–benefit profile than the intervention with older-generation drugs. The older and current treatments may offer similar potential benefits, but the current treatment may have a slightly lower incidence of one side effect such as nausea. In this case, participation in the research study would pose net risks to participants represented by the increased incidence of nausea with the older drug as compared with the current treatment.
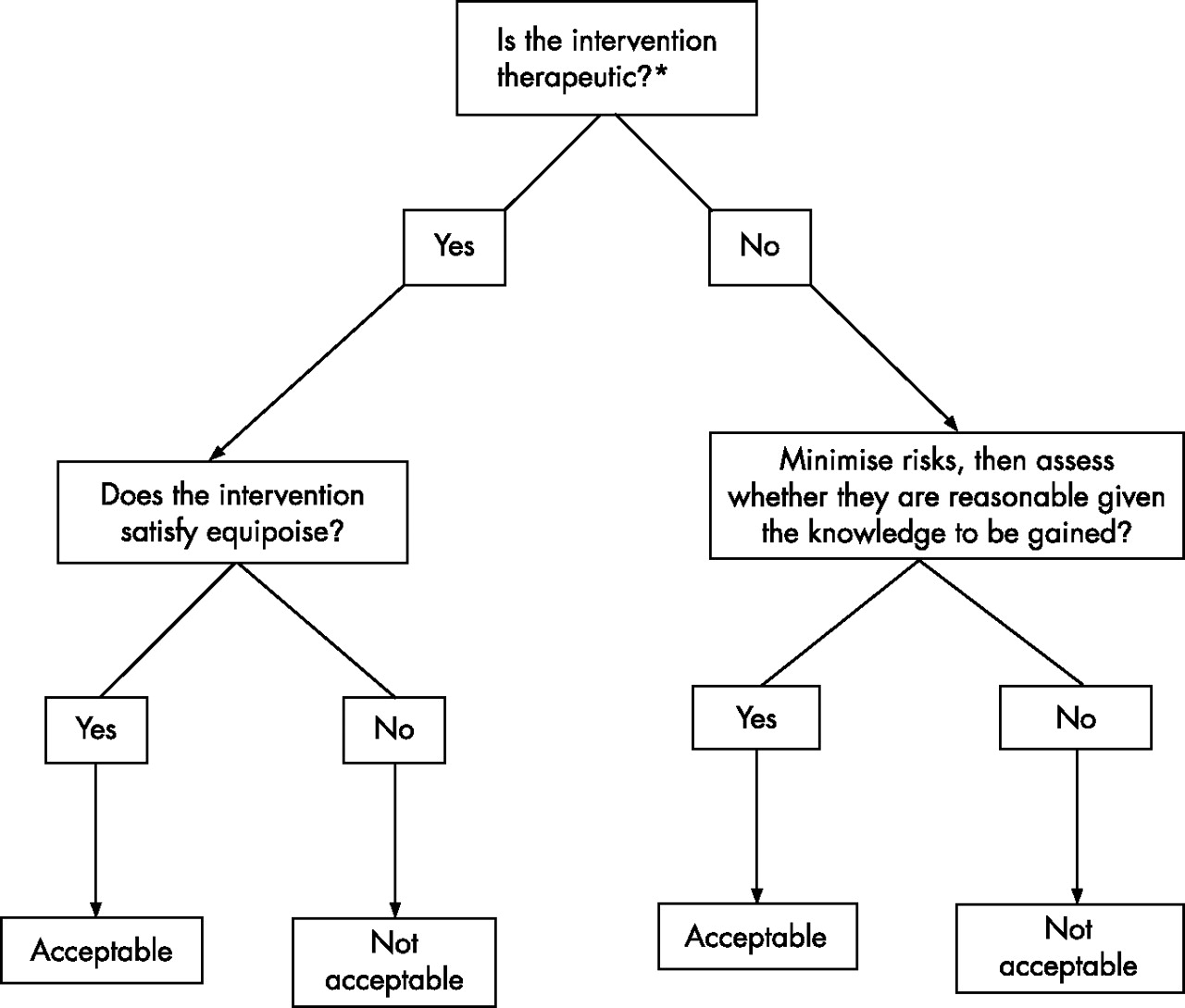
Whether the risks of studies that use administration of older-generation treatments are acceptable depends on whether the risks are minimised, benefits enhanced, the net risks to participants are sufficiently low and the value of the research justifies the net risks. To make this determination, RECs need a method that focuses on the risks that participants face and ensures that RECs assess the two potential sources of net research risks. The net risks test, divided into the following three steps, provides such a method (fig 2).

{kind=link}
{kind=link}
Net risks test for individual interventions. *Net risks refer to the extent that the risks and burdens of the intervention exceed its potential for clinical benefit. **For individuals who cannot consent, it is widely agreed that net risks should be minimal or at most a minor increase over minimal. For competent adults, there is no consensus on whether there should be a risk limit and if so how it should be defined.
Identify the net-risk interventions
The REC should identify the individual interventions included in the study under review. The REC should assess the risk–benefit profile of each intervention by comparing its risks with the potential clinical benefits for participants. The REC should then assess the risk–benefit profile of the available alternatives to each intervention, which, in some cases, may be no intervention at all, and then compare the risk–benefit profile for participants of each research intervention with that of the available alternatives.
When the risk–benefit profile of the research intervention for participants is at least as favourable as that of the available alternatives, including not undergoing the intervention at all, it poses no net risks. Conversely, research interventions that offer participants a less favourable risk–benefit ratio than one or more of the available alternatives, including not undergoing the intervention at all, pose net risks. The magnitude of the net risks is a function of the extent to which the intervention presents increased risks or decreased potential benefits compared with the available alternatives.
A study may provide an experimental treatment that is believed to have a risk–benefit profile equivalent to that of the standard of care, followed by a positron emission tomography scan for research purposes. The treatment poses no net risks because its risk–benefit profile is considered to be as favourable for participants as the available alternative of standard of care. The positron emission tomography scan, in contrast, poses net research risks from the use of low-dose radiation, because it offers a negative risk–benefit profile to participants, compared with the alternative of not undergoing the intervention at all.
Assess the net risk interventions
The REC should next ensure that the risks of each intervention that poses net risks are not excessive and are justified by the social value of the knowledge to be gained by its use in the study. For example, the REC should determine that the risks posed by the positron emission tomography scan conducted for research are not excessive, and that these risks are justified by the information to be obtained by having participants undergo the positron emission tomography scan.
Assess the net cumulative risks
Finally, by assessing the risks of individual interventions, the net risks test allows RECs to avoid the so-called “package deal”, which justifies the risks of some interventions by the potential benefits offered by other interventions in the same study.10 Assessment of individual interventions precludes investigators from justifying the risks of a biopsy for research on the grounds that the drug under study provides important medical benefit to participants. By limiting assessment of the REC to the risk–benefit profile of individual interventions, however, we ignore the possibility that “research may involve several different procedures that may involve minimal risk or burden individually, but that may present more than minimal risk when considered collectively”.11 The finding that a single magnetic resonance imaging and a single blood draw each pose minor risks fails to assess whether inclusion of a series of these procedures in a single study poses excessive risks. To assess this concern, RECs should calculate the cumulative net risks of all the interventions in the study under review and ensure that, taken together, the cumulative net risks are not excessive.
How should RECs determine whether the net risks of individual interventions and the net cumulative risks of research studies are excessive? It is widely agreed that vulnerable research participants, such as children and adults, who are unable to consent should not be exposed to net risks that exceed a minor increase over minimal. In contrast, there is a lack of consensus over whether there should be a priori limits on the risks to which adults who are capacitated may be exposed for the benefit of society. Can adults who are capacitated be able to consent to enrol in a study that poses serious net risks to them but offers the potential for profound social benefit, such as finding a cure for malaria? Permitting such research would raise the potential for serious abuses. Yet precluding such research in all cases seems inconsistent with other contexts where we sometimes allow adults who are capacitated to face serious risks for the benefit of society, such as firefighting and military service. Future research should assess whether there is a need for a limit on the net risks to which adults who are capacitated may be exposed and, if so, how this limit should be defined.
THE NET RISKS TEST AND PHASE I STUDIES
To clarify the net risks test, consider the assessment of phase I studies—a controversial research design. RECs reviewing phase I studies should enhance the benefits and minimise the risks by eliminating duplicative procedures and assessing whether the same information may be gained by using less risky procedures. The RECs then should identify the interventions that pose net risks, and compare their risk–benefit profile with that of the available alternatives, including not undergoing the intervention.
This assessment is similar to that used by many research regulations. When reviewing paediatric research, the US federal regulations require IRBs to assess whether individual research interventions offer a prospect of direct benefit. To assess individual interventions that offer children a prospect of direct benefit, the federal regulations instruct RECs to assess whether: (a) the risk is justified by the expected benefit to the children; and (b) the relationship between the expected benefit and risk is at least as favourable to the children as that with available alternative approaches. This assessment is essentially identical to the first two steps in the net risks test: identify the risk–benefit profile of individual interventions and then compare them with that of the available alternatives. Notice that both approaches require RECs to directly assess the risk–benefit profile of research interventions rather than first dividing all interventions into two different categories as recommended by the dual-track assessment. The similarity between the net risks test and the guidance offered by research regulations suggests that the net risks test, unlike the dual-track assessment, should be relatively familiar to most RECs.
For phase I studies in healthy volunteers, the preferred alternative would be not enroling in the research at all. Hence, the net risks of the experimental agent and the net risks of the other included interventions, such as blood draws, would be all the risks that these interventions pose to healthy volunteers. In this case, the REC should approve each intervention only when the risks to participants of each intervention are justified by the social value to be gained by the inclusion of that intervention in the study.
For phase I agents tested in patients, the REC should determine the risk–benefit profile of all the interventions for participants, including administration of the tested agent, and then compare the risk–benefit profile of each intervention to the available alternatives. When other treatments are available, the phase 1 agent should be compared with them. In the absence of treatment alternatives, this assessment should compare the risk–benefit profile of the phase I agent to receiving palliative care or no treatment at all.
The REC should approve each intervention only when the net risks it poses to participants, if any, are not excessive. Finally, the REC should assess the net cumulative risks of the study, ensuring that they are not excessive and are justified by the social value of the study. Research participants unable to provide informed consent should not be exposed to net risks that exceed a minor increase over minimal. Future research will be needed to determine whether the same limit should apply to research with adults who are capacitated.
CONCLUSION
Dual-track assessment, endorsed by the US NBAC and other commentators and groups, directs RECs to assess the risks of research interventions by first dividing them into two categories defined as therapeutic and non-therapeutic. This approach complicates the process of risk assessment without increasing the protection to research participants. In addition, confusion over which interventions are therapeutic and which are non-therapeutic suggests that the dual-track method will be difficult to implement.
The net risks test, in contrast, relies on the clinically familiar method of assessing the risks and benefits of interventions in comparison to the available alternatives. The net risks test, unlike dual-track assessment, also focuses attention of the RECs on the central challenge of protecting research participants—namely, whether they face excessive risks—thereby providing clearer guidance to RECs and more appropriate protection for research participants.
Acknowledgments
We thank Paul Litton, Donald Rosenstein and Christine Grady for their helpful comments on previous drafts of the manuscript. This work was completed as part of the authors’ official duties as employees of the US NIH.
Dual-track assessment directs research ethics committees (RECs) to assess the risks of research interventions based on the unclear distinction between therapeutic and non-therapeutic interventions. The net risks test, in contrast, relies on the clinically familiar method of assessing the risks and benefits of interventions in comparison to the available alternatives and also focuses attention of the RECs on the central challenge of protecting research participants.
Footnotes
-
Competing interests: None.
Linked Articles
Other content recommended for you
- Refuting the net risks test: a response to Wendler and Miller’s “Assessing research risks systematically”
- Individual risk and community benefit in international research
- Limits to research risks
- Can informed consent to research be adapted to risk?
- Risk, double effect and the social benefit requirement
- Meeting the goal of concurrent adolescent and adult licensure of HIV prevention and treatment strategies
- The potential benefit of the placebo effect in sham-controlled trials: implications for risk-benefit assessments and informed consent
- Assent in paediatric research: theoretical and practical considerations
- Process of risk assessment by research ethics committees: foundations, shortcomings and open questions
- When to start paediatric testing of the adult HIV cure research agenda?