Article Text

Statistics from Altmetric.com
Results of the Paralympic Injury and Illness Surveillance Study noted an unusually high injury incidence rate (IR) in the sport of Para alpine skiing at the 2014 Sochi Paralympic Games (IR 48.3, a sixfold increase in acute injuries in comparison to the Vancouver 2010 Paralympic Games).1–3 There were likely several associated factors. Some were clearly modifiable such as the course design, number of training runs permitted on the course and the command and control structure between the technical and medical staff. Additionally, Paralympic officials recognised that careful monitoring of weather data and timely management of snow production, taking advantage of modern technology, had the potential to reduce injury risk. Thus, for the 2018 PyeongChang Paralympic Winter Games (the Games), the International Paralympic Committee (IPC) Medical Committee, in collaboration with the World Para Alpine Skiing (WPAS) sport technical staff, implemented a series of changes following Professor Willem van Mechelen’s ‘Sequence of (Injury) Prevention’ model4:
Step 1: Establishing the extent of injury
The Paralympic Injury and Illness Surveillance Study carried out at the Sochi 2014 Paralympic Games demonstrated a dramatic increase in injuries in Para alpine skiing.1 2
Step 2: Establishing the aetiology and mechanisms of injury
The IPC Medical Committee hypothesised that this increase was likely most attributable to poor snow conditions and an overly aggressive course setting in Sochi.
Step 3: Introducing preventative measures
In response, the IPC Medical Committee collaborated closely with WPAS technical staff to implement the following measures.
The course setting during the test event in March 2017 included less aggressive lines and ‘waves’ instead of jumps. This course setting was then replicated at the Games with use of GPS technology.
The WPAS Management Team worked closely with the PyeongChang Organising Committee and experts from the Federation Internationale de Ski (FIS) in the snow preparation phase, including: (1) the development of a snow contingency plan, (2) continuous grooming of the course and (3) implementing new methods of snow preparation to ensure excellent race conditions throughout each day of competition.
Immediately after the Olympic Games, WPAS officials carried out proactive site inspections in conjunction with FIS, enabling a translation of ‘lessons learnt’ from the Olympic Winter Games to the Paralympic Winter Games.
The precompetition schedules were carefully crafted allowing for more days to schedule official downhill trainings prior to the start of competition.
Official pre-Games technical and medical briefings included an education programme for team medical and coaching staff.
Earlier start times were employed to take advantage of excellent snow conditions.
Step 4: Assessing the effectiveness
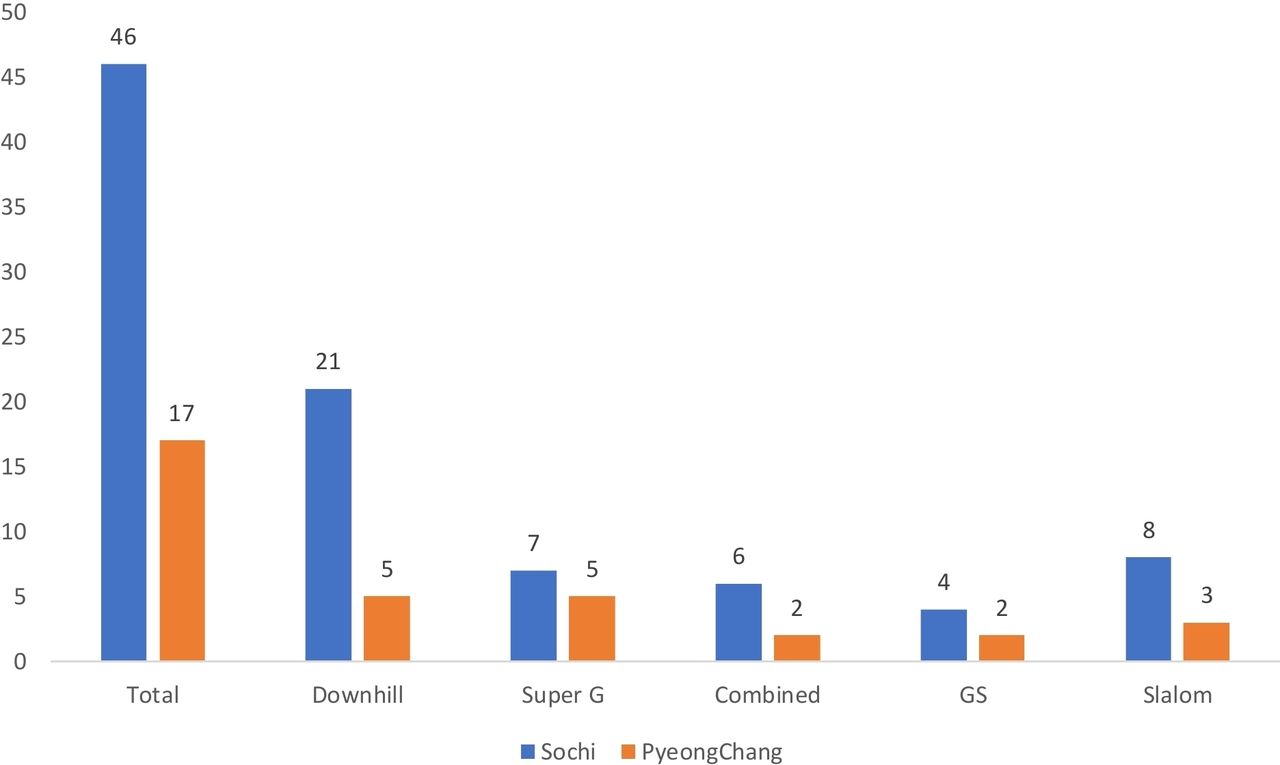
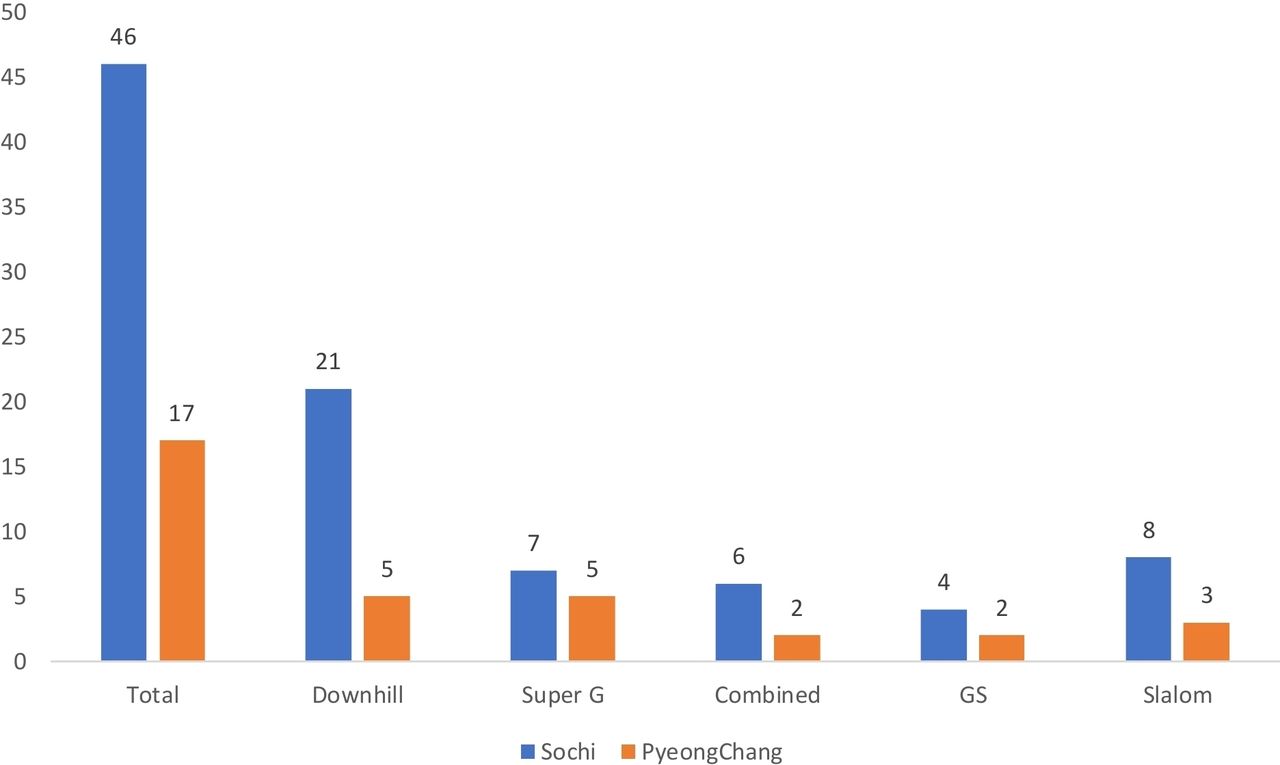
Let’s compare the number of injuries in the two Paralympic Games. A total of 98 injuries were reported in Sochi, while there were only 39 in PyeongChang. There were 17 acute injuries in competition in PyeongChang (down from 46 in Sochi); these injuries included five in downhill racing (down from 21 in Sochi) (figure 1). In PyeongChang, 11 athletes failed to finish (‘did not finish’); that category included 24 athletes in Sochi.
{kind=link}
Total acute injuries by Para alpine ski event at the Sochi 2014 Paralympic Winter Games versus the PyeongChang 2018 Paralympic Winter Games.
In addition to measures taken above, ‘mother nature’ likely played a role in mitigating injury. The weather was cold during speed events in PyeongChang, whereas it had been warm in Sochi (eg, average temperature was −2°C in PyeongChang vs 9°C in Sochi during the downhill, respectively).
Our experience suggests there is value in expediting the ‘Sequence of (Injury) Prevention’ model4 and imparts several important lessons.
In cases where there is the potential for athletes to suffer immediate harm (ie, traumatic injury), clinicians would be irresponsible if they stood by—doing nothing—while waiting for high quality scientific studies. At those times, it is ethical and wise to take rapid action to mitigate the risk.
Forming a healthy and productive collaboration between sports medicine and sport management is essential—sports medicine should be at the table to inform sport technical policy. We clinicians cannot work in a silo and expect to prevent injuries. Rather, contextual and socioecological factors must be considered to develop effective strategies.5
It is not acceptable to simply class a sport as ‘dangerous’ and accept high injury IRs as part of the sport culture. Rather, when high injury IRs are noted, one must look carefully at what immediate changes can be made to mitigate injury and ensure that athletes are not facing undue risk of harm.
This describes a concrete example of injury surveillance that identified sports in need of urgent attention. We then took considered, appropriate and rapid action. We measured and shared the outcomes.
Footnotes
Correction notice This article has been corrected since it published Online First. The title has been corrected.
Contributors The corresponding author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive license (or non-exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd and its licensees to permit this article (if accepted) to be published in Journal (British Journal of Sports Medicine) editions and any other BMJPGL products to exploit all subsidiary rights, as set out in our license.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.