Meta consent: a flexible and autonomous way of obtaining informed consent for secondary research
BMJ 2015; 350 doi: https://doi.org/10.1136/bmj.h2146 (Published 07 May 2015) Cite this as: BMJ 2015;350:h2146
- 1Centre for Applied Ethics and Philosophy of Science, Aalborg University Copenhagen, Department of Communication, AC Meyers Vænge 15, København SV 2450, Denmark
- 2University of Manchester, School of Law, Oxford Road, Manchester M13 9PL, UK
- Correspondence to: T Ploug ploug{at}hum.aau.dk
- Accepted 25 March 2015
A rapidly increasing capability for storing, linking, and analysing health data has led to new opportunities for research. However, it also raises new ethical and regulatory concerns. Central among these is the question of the conditions under which secondary research can use data that were collected as part of routine healthcare practice or for a specific research project. Does secondary use require renewed informed consent from the original participants?
New developments in data handling and analysis throw up new problems, such as whether it is possible to make patient data unidentifiable, and to what degree.1 2 If the use of identifiable data requires informed consent, we must carefully reconsider whether informed consent is robust enough to withstand the more complex ethical challenges that technology brings with it; for example, in relation to the level of privacy protection that can be offered now and in the future.3 In this paper we propose a model for resolving these tensions—“meta consent.”
Informed consent
Historically, informed consent in clinical healthcare gave doctors permission to perform acts that would otherwise have been classed as physical assaults. Later, the requirements were extended to protect the individual against risk of harm, to protect personal autonomy (defined as the right to form and pursue one’s own goals and values), and to protect the individual’s privacy and right to control personal information.
At least two factors have the potential to override the requirement for informed consent. Firstly, society may have an interest in gaining access to personal health data to, for example, make research possible. Secondly, it may be impossible to obtain consent. The current focus on “big data” sets these two factors in sharp relief. On the one hand, building and linking vast databases of individual health data has considerable potential for promoting health and benefiting society, as has been recognised in a number of official reports under the big data banner in the United Kingdom and the “learning healthcare system” in the United States.4 5 On the other hand, the practicalities of getting full informed consent for every secondary use of data will hinder research. Any requirement for informed consent must balance these factors, and two recent models (“broad consent” and “dynamic consent”) attempt to do so in different ways.
Broad consent
Broad consent means that the individual is given the option of consenting to future research of a particular type (in terms of both content and context) rather than to only a specific research project. It has attracted attention for its use by biobanks.6 7 8 The broad consent model protects society’s interest in research, as a practicable way of implementing consent for open ended projects. Opponents argue that broad consent is not necessarily informed consent because informed consent requires specific information about the research for which the data or tissue may be used.9 10 11 12
It is also questionable whether a patient who has given broad consent for secondary research in a clinical encounter can be said to have given valid consent, because the attention of both the patient and the healthcare professional is likely to be firmly fixed on the clinical problem rather than the research.
Dynamic consent
An alternative, participant centred, model has been suggested, in which the information about specific secondary use of health data or tissue and a request for consent is put to the individual through a web based platform.13 14 15 16 This dynamic consent model protects the autonomy of the participant by providing information about each new data application and by making the provision or withholding of consent easy and flexible. The high penetration of internet access makes the model feasible, at least in the Western world.
It could be argued, however, that dynamic consent based entirely on opting in does not sufficiently protect society’s interest in research. Only between 50% and 90% of participants consent to secondary use of tissue and between 40% and 90% to secondary use of health data.6 17 The model might work for specific research projects or biobanks, but it is difficult to see how it might function in isolation for research using routine clinical data. Every request for dynamic consent would have to be accompanied by a description of the entire project. It is also likely that participants would receive a high volume of consent requests and that repeated requests would lead to the routinisation of consent or to “consent fatigue.”18 19 20 21 In other words, giving or withholding consent may become an unreflective, habitual act based on little or no knowledge of the potential use of data or tissue.
Meta consent
We propose a new model of consent—meta consent—that combines the broad and dynamic models, with additional options for blanket consent and blanket refusal. The idea is simply to let individuals choose how they wish to provide consent for future secondary research of data collected in the past or of data that will be stored in the future. This means that meta consent is both retrospective and prospective.
Individuals would be informed about the types of research (box) for which their consent could be requested in the future, and on this basis they can decide their preferred method of requesting consent for each. In essence, future consent requests can be generated and communicated by means of information and communication technology, based on the individual’s choices.
Variables related to informed consent
Types of consent
Dynamic consent
Broad consent
Blanket consent
Blanket refusal
Types of research
Content
Electronic patient records
Tissue or genomic data
Health data
Non-health data
Context
Private or public
Commercial or non-commercial
National or international
The first decision to be made by the health authorities that would design the meta consent system is whether there are any types of research for which consent should not be sought, reflecting the interests that potentially override those of protecting the individual. Some might argue that no consent should be needed for any research that requires considerable effort to identify an individual or if data use is monitored by national data authorities or research ethics committees, such as research using limited sets of anonymised data. However, it has become much easier to identify, track, and contact individuals from their data.
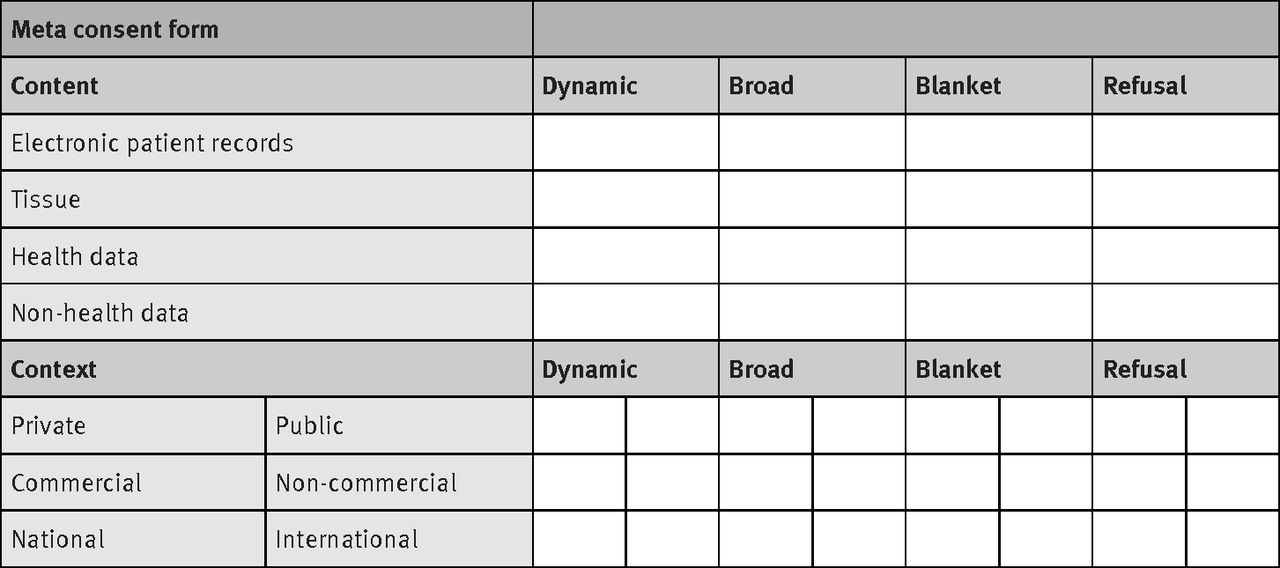
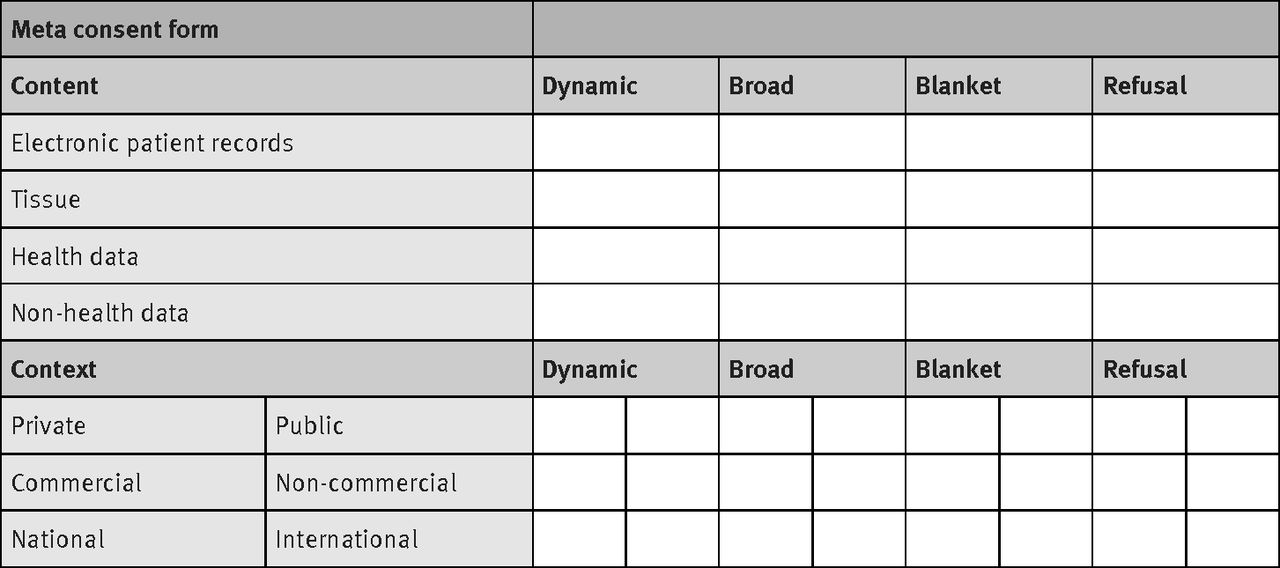
The second step in the implementation of meta consent is for individuals to choose the type of consent—dynamic consent, broad consent, blanket consent, or blanket refusal—that they wish to give for different types of research. Individuals could be asked to fill in a simple “tick box” table online (fig 1⇓).
{kind=link}
Choosing dynamic consent means that they would be asked for specific consent for every new research project in that category that used their data. Broad consent means that they would only be asked if a new project was outside the scope of their broad consent. Blanket consent means that their data would be used without further consent. If a future research project fell under more than one category, the most restrictive consent choice would apply.
Meta consent is a truly individual consent procedure that takes into account the differences in personal interests and levels of trust in researchers among the population. The risk of routinisation is reduced because individuals can limit the requests they receive to only those categories of research that really matter to them. Its implementation online makes meta consent easy to revoke or change.
Implementation
Meta consent should be arranged early in life, which could be achieved by making it mandatory as an individual comes of age. It might be set alongside the acquisition of other democratic rights as a way of marking the transition into adulthood. Parents could provide meta consent for children below the age of majority. Failure to provide meta consent could be handled in several ways—the individual could receive reminders from healthcare professionals when seeking treatment, reminders could be linked to the use of various official web services, or a default position of broad consent could be applied.
Implementation of meta consent requires a technological infrastructure at the societal level that enables the collection of meta consent, the generation of specific consent requests depending on the meta choices, and the two way communication between individuals and researchers of specific consent requests and decisions. This could be implemented relatively easily in countries where individuals are identifiable through a unique personal identification code, and where citizens are already required to have a publicly authorised electronic mailbox (in Denmark and Norway, for example). In these countries, the code is used to link data for epidemiological research and to direct mail to the mailbox. Implementing a further link to a consent request generator would be straightforward. However, until the internet is universally accessible there will be a segment of society that the system cannot serve. Although this group is likely to diminish over time, it is worth considering whether a default option might be helpful.
With the increasing use of technology in the interaction between citizens and the state, protection of citizens’ autonomy and privacy will become more important—and more difficult. Meta consent could enable the secondary use of data while providing flexible and workable protection to the individual.
Key messages
Traditional informed consent does not work well in the context of using health data in secondary research
Suggested alternatives, broad consent and dynamic consent, raise ethical and practical concerns
Individuals differ widely in their views on secondary use of their health data
We propose a practically implementable model of meta consent that allows research to go ahead while protecting the legitimate interests of individuals
Notes
Cite this as: BMJ 2015;350:h2146
Footnotes
Contributors and sources: TP had the initial idea, which was refined in discussion with SH. TP wrote the first draft, which was revised by SH. Both authors worked on subsequent revisions of the manuscript. The authors cover slightly different areas of expertise within the field of medical ethics. TP is the guarantor.
Competing interests: We have read and understood BMJ policy on declaration of interests and have no relevant interests to declare.
Provenance and peer review: Not commissioned; externally peer reviewed.