Article Text

Abstract
Clinical ethics support (CES) services are experiencing a phase of flourishing and of growing recognition. At the same time, however, the expectations regarding the acceptance and the integration of traditional CES services into clinical processes are not met. Ethics rounds as an additional instrument or as an alternative to traditional clinical ethics support strategies might have the potential to address both deficits. By implementing ethics rounds, we were able to better address the needs of the clinical sections and to develop a more comprehensive account of ethics quality in our hospital, which covers the level of decisions and actions, and also the level of systems and processes and aspects of ethical leadership.
- clinical ethics
- ethics committees/consultation
Statistics from Altmetric.com
Introduction
Clinical ethics support (CES) services are experiencing a phase of flourishing and of growing recognition. After the first steps in this movement were taken four decades ago in the USA, and about 20 years later also in Europe, clinical ethics consultation services and clinical ethics committees started to appear in more and more hospitals and institutions. At the same time, however, the expectations regarding the acceptance and the integration of traditional CES services into clinical processes are not met. In this paper, we will describe the implementation of ethics rounds as an additional instrument or as an alternative to traditional clinical ethics support strategies that might have the potential to address both deficits.
Background
Clinical acceptance
There are not much data available, but previously published studies revealed that although ethical uncertainties are frequently reported by healthcare professionals,1 the workload of many traditional CES services (consultation following requests) remains remarkably low.2 In 2006, 90% of the responding CES services in a US survey performed fewer than 25 ethics consultations per year; 20% had no consultations throughout the year. The median number of consultations was three.3 In the UK, a survey in 2010 showed that over half of the responding CES services received 1–5 requests for consultations in the previous 12 months; an additional 31% received 6–10 requests in that period.4 In Germany, only 18% of the responding CES services reported to have had more than 25 consultations between 2007 and 2012 (which roughly means four consultations per year).5
Little is also known about how clinicians perceive CES services.6 7 Few openly critical comments exist where clinicians, for example, were reported to feel scrutinised by CES services, bothered by ‘instant opinions’ on any ethically relevant clinical decision they make.8 In a national telephone survey among more than 300 US internists published in 2004, a majority of clinicians (as has been shown before9) reported positive experiences with CES services. However, more than 40% of the participants expressed reservations about CES in general or the quality of the service in their institution.10 Another study among the residents of a large academic teaching hospital revealed that 30% of the responding residents either were not aware of the CES services in their institution or had negative perceptions of ethics consultations.11 In this study, 89% of respondents never requested an ethics consultation.
Against this background, it might not come as a surprise that the expansion of CES services in healthcare organisations in the US and Europe is increasingly accompanied by critical voices from various sides. Here, fundamental questions are at stake, like the ends of clinical ethics consultation12 and the expertise of clinical ethics consultants.13 Evidence7 14 and professional standards are forcefully called for.15 Some authors have identified one major shortcoming of traditional approaches to clinical ethics support: They are criticising that most CES services are not well integrated with other parts of the respective organisation16–18 and are, thus, partly unaware of the needs of modern healthcare organisations.16 While focusing on only one level of ethics quality in healthcare (on the level of (a) decisions and actions), traditional CES services are said to be neglecting other important aspects on the levels of (b) systems and processes and (c) environment and culture.16 However, the proposed alternatives like ‘Preventive Ethics Teams’19 or ‘Liaison’ programs17 require major efforts and human resources as well as financial resources. It still seems to be the case that most CES services are solely operating with the traditional consultation model.
Top-down or bottom-up
Another line of critique addresses the principal approach of many CES services. The consultation model is usually implemented as a stand-alone clinical ethics consultation (offered by one or more consultants), or as one of several services of a clinical ethics committee.3 4 20 21 Both traditional approaches are providing consultation on request with the aim of resolving ‘uncertainty or conflict regarding value-laden concerns that emerge in healthcare’.22 ‘Ethics facilitation’ has repeatedly been outlined as the recommended approach to ethics consultation with the consultant facilitating the ‘building of a principled ethical resolution’.22 The consultants should not act as moral authorities, but have the necessary expertise and skills in order to support this process. Nevertheless, arriving at a recommendation or an action plan still seems to be the favoured goal for many consultants.3 The ways through which the recommendation or action plan are achieved vary substantially and—as far as we know—often, but not always do involve one-on-one or group meetings with the relevant stakeholders (team, patients, relatives).12 These approaches are sometimes characterised as having a top-downi perspective20 23 with the risk of consultants acting as moral ‘experts’ and the risk of authoritarian misuse.
The traditional approaches are contrasted with newer CES services with a bottom-up perspective like ethics rounds or moral case deliberation, where healthcare professionals themselves are pursuing the resolution of ethical conflicts. Although moral case deliberation is similarly concerned with conflicts in patient cases like the traditional approaches of CES, it is not focused on giving recommendations, but instead described as a facilitated reflection process that aims to raise awareness for ethical issues among healthcare professionals and to support them in making independent decisions.24 Ethics rounds have been implemented to provide a continuous structure where healthcare professionals from different disciplines can reflect on ethically difficult aspects of patient’s cases.25 The primary goal of ethics rounds is to develop relevant competencies in healthcare professionals in order to identify, prevent and solve ethical conflicts. Usually, a facilitator or clinical ethicist accompanies these rounds, supports with ethical (or legal) expertise, if needed, and ensures that the reflection process follows given rules.
In our institution, variants of both approaches—the traditional consultation service as well as ethics rounds—have been implemented consecutively and we will shortly describe the implementation process in the following paragraph.
From ethics consultation to ethics rounds: implementation process and framework conditions
The Uniklinik RWTH Aachen is a large maximum-care university hospital in western Germany with 1400 beds and nearly 50 000 inpatients annually. Intensive care units comprise interdisciplinary intensive care units (ICUs) (103 beds), medical ICUs (36+14 beds) and a neurological ICU for adults, as well as a neonatal/paediatric ICU.
In 2008, the clinical ethics committee was founded by resolution of the management board of the hospital, which thereby answered to a joint initiative of the Department of Medical History, Theory and Ethics and the Department of Palliative Medicine.
It has 18–20 members, is multidisciplinary and traditionally defined consultation, education and policy work (all on request) as its main tasks. Most of the requests for consultation are addressing ethical conflicts at the end of life. Before the implementation of the ethics rounds, the number of requests was similarly low like in many other CES services in Germany and internationally with two to six requests annually.
In 2010/2011, the idea grew to install ethics rounds as a structure for continuous discussion of ethical aspects in patient-centred rounds in ICUs. The initiative was prompted by the ICU teams. They are experiencing the ICU as a workplace full of potential conflicts, most commonly between the intensive care team and patients (respectively the relatives), but also within the team, which could benefit from a continuous exchange on ethical aspects of their work.
We started at a medical ICU (MICU) with cardiological and pneumological focus in May 2011. Ethics rounds were implemented as an extension to the normal grand rounds, took place once a week and were accompanied and facilitated by a clinical ethicist. These ethics rounds are structured similar to the normal grand rounds and are composed of the attending intensivist with cardiological background, a pneumologist, the head nurse of the ICU, the nurse treating the patient at the time of rounds and the ethicist. Rounds are opened by the intensivist with description of the medical history and overall critical care condition mentioning acute problems. Usually then, the nurse treating the patient describes his/her impressions of the patient and further critical care problems that might not have been mentioned before. Besides the usual daily treatment plan resulting from the interdisciplinary communication, the whole team explicitly reflects on ethical aspects in their discussion of each patient, including patient wishes, end-of-life aspects, issues of patient autonomy, surrogate decision-making and differing perspectives among the staff where appropriate. Reflections were aimed to be rational, free of hierarchy and pressure and including as many relevant perspectives as possible. There were no predefined rules for this part of round discussions. The aim was to achieve a consented decision by the whole ICU team regarding further treatment, treatment goals, possible end-of-life issues and a plan to resolve possible conflicts within the team or between the ICU team and patient surrogates. The ethicist has a threefold function in this aspect of rounds: moderator of the ethics part of the discussion, adviser on ethical issues and legal aspects of treatment or treatment decisions, and mediator in regards to possible conflicts. The results of these ethics rounds are documented in the PDMS patient file. The implementation process was prepared by questionnaire surveys among the staff, which highlighted areas for development in rounding and daily clinical work from an ethical perspective. In addition, the ethics rounds were evaluated on an annual and later on a 2-yearly basis by questionnaire surveys or team meetings.
In 2014, an interdisciplinary ICU team (iICU, Anaesthesiology and Neurosurgery) decided also to implement ethics rounds. The implementation process followed the MICU example. In both ICUs, a majority of the staff voted for continuation of the ethics rounds in every evaluation.
Ethics rounds: effects
As prominently outlined by Fox and colleagues16 in their Integrated Ethics model, the ethics quality of a healthcare institution is displayed not only and not even primarily on the level of (a) decisions and actions in relation to individual patients but also on the level of (b) organisational systems and processes, and on the level of (c) the organisation’s ethical environment and culture. If clinical ethics support services are aiming at improving the ethics quality (as one aspect of the overall quality) of a healthcare institution, they have to address all levels in order to bring about change. Even though not intended primarily, we made the experience that the implementation of ethics rounds had effects on all three levels of ethics quality in our institution.
Decisions and actions
The level of decisions and actions in relation to individual patients is the customary target level for traditional CES services like clinical ethics consultation. In addition to our traditional consultation service, we implemented ethics rounds with the main intention of proactively addressing and preventing possible uncertainties and conflicts in end-of-life-related decision-making. We intended to approach these problems at ethics rounds by early identification of possible sources of ethical conflict for each patient and by continuous education on ethical and legal aspects of end-of-life care.
Effects on this level could be measured in various ways, for example, as satisfaction of staff, or patients/relatives with decisional processes at the end of life, or as the percei ved need for clinical ethics consultation (indicating the number of conflicts that arise). For our purpose here, the latter is especially interesting because of the two differing categories of CES services (top-down and bottom-up), to which traditional clinical ethics consultation and ethics rounds belong. To our knowledge, there are no data available so far on how these two different types of CES are interacting with each other if implemented in the same institution.
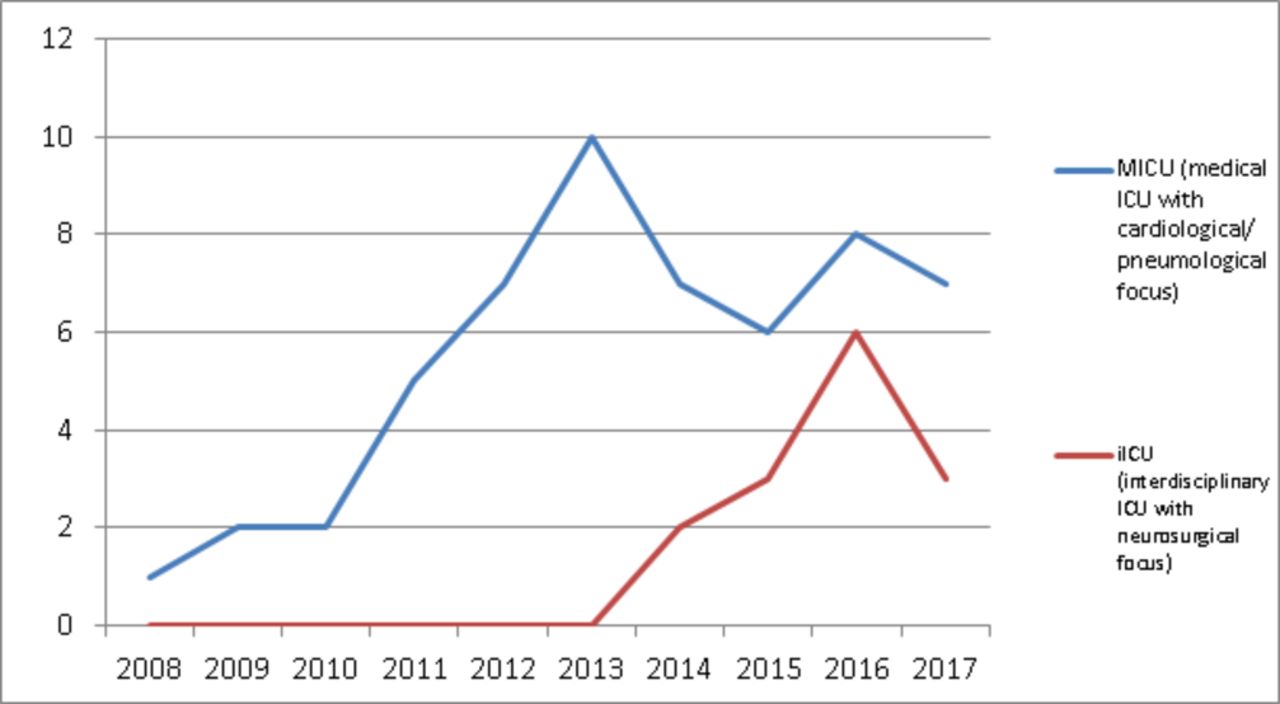
What we experienced in both sections was a quick and sustained increase in requests for clinical ethics consultation in the years after the implementation of ethics rounds.
The subjects of the requests did not change compared with prior the implementation.
Systems and processes
Ethical questions on the level of organisational systems and processes are not the typical area of responsibility for clinical ethics support services, but often they can be identified below the surface of case consultations. Many cases are exhibiting similar patterns of how the conflicts developed and grew, which sometimes are pointing to a problem on a deeper, structural or systematic level. Recurring conflicts related to complications after certain surgical procedures for example could indicate deficits in preoperative informed consent procedures. To identify and address these kinds of ‘ethics issues’19 on an organisational level has been termed to be one of the major challenges for clinical ethics.26 It is certainly a first step towards integrating CES services into the quality improvement efforts of healthcare organisations.
Implementing ethics rounds is in itself an action on the level of systems and processes which, in our organisation, was primarily done in order to respond to a felt need for earlier intervention in ethically complex patient cases. Therefore, we expected to mainly see its effects on the level of decisions and actions in relation to individual patients—as described above. Although there have been effects on this level (more requests), the major impact could be observed on the level of systems and processes.
First, a different type of clinical ethics counselling service was requested by the ethics rounds teams for ethically complex cases, where ethics rounds could not fix all problems, and was established as the main service from then on. Instead of asking for a traditional clinical ethics consultation, they frequently wished for support by a clinical ethicist in meetings with relatives or in team meetings in order to only have her moderating the discussion. These moderated meetings are not resulting in a recommendation but aim at encouraging communication and discourse. It is only the agents themselves who are discussing and trying to develop a solution for a complex situation or a conflict in a moderated process of discussion.
In these moderated meetings, the clinical ethicist first and foremost is in need of communication skills in order to support the agents in identifying and overcoming potential obstacles to sound ethical reasoning. They are having more aspects in common with reflective bottom-up approaches of ethical reasoning than with the traditional top-down consultation model resulting in ethical decisions.27
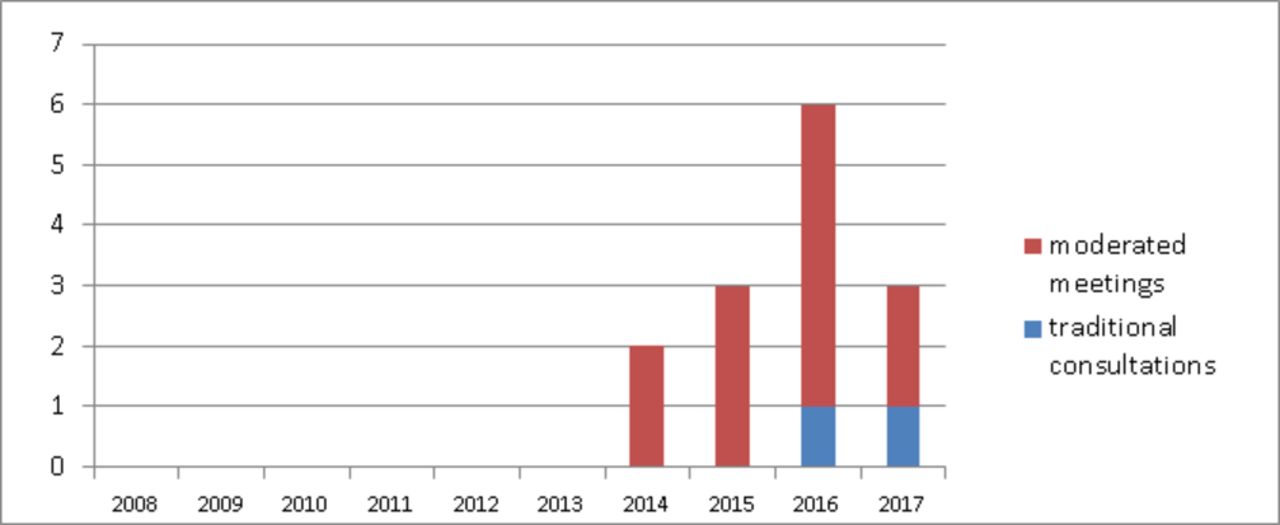
Looking at the requests for clinical ethics consultation after the implementation of ethics rounds in more detail, we saw in both sections that the described remarkable increase in numbers has largely been due to the requests for moderated meetings with teams and relatives.
As a second major effect, both ICUs described significant changes in everyday rounding structures as a consequence of doing ethics rounds once a week. Main characteristics of ethics rounds have been transferred into daily routine and are now pursued independently of clinical ethics support. The iICU team managed to newly install the report of the nurse, who is responsible for the particular patient, as an obligatory part of bedside rounding. This shift from physician-centred bedside rounding to interprofessional rounding structures, which is mandatory for our model of ethics rounds, has been found to be supporting also for everyday patient-related interprofessional communication.
The MICU team, which already had an interprofessional rounding structure for physicians and nurses prior to the implementation of ethics rounds, reports more content-related changes insofar as they started to routinely include ethically complex aspects in their everyday rounding reports. As a follow-up or preparation for weekly ethics rounds, they shortly discuss ethical aspects where appropriate in daily grand rounds. Interprofessional reflections on ethical conflicts or uncertainties, thus, have evolved to be a natural part of clinical routine, of providing good clinical care. In addition, the team has expanded the interprofessionality of ethics rounds and now also includes physiotherapists in this setting.
Environment and culture
The third level of ethics quality in a healthcare organisation is also termed as ethical leadership, and in the already cited Integrated Ethics model defined as ‘activities on the part of leaders to foster an ethical environment and culture’. For traditional CES services like clinical ethics case consultation, which are naturally targeting mainly decisions and actions in relation to individual patients, this level is even harder to address because an ethical leadership is a necessary precondition and not a working area for these services. If ethics quality a priori is not understood and appreciated as part of the overall quality of an organisation by its leaders, then the staff will not feel encouraged or authorised to seek for clinical ethics consultation. And due to the top-down approach, traditional CES services can do very little to enable the staff to initiate changes—even more so if consultations are not requested at all.
In our institution, where ethics quality already had a high priority for the leadership of both ICUs, the effects of the implementation of ethics rounds were mainly described as an improved exchange between the leaders and the staff on the institutional ideal of ethics quality and culture, and on the necessary steps to realise this ideal. Whereas, for example, initially the staff of the MICU voted for anonymous evaluation of daily rounding and ethics rounds by questionnaire survey, they in the following years wanted to discuss ethically relevant aspects of the structures and procedures of their unit directly in a team meeting with the head of the clinic and the rounding ethicist. This improved exchange in turn made the realisation of necessary next steps easier.
Discussion: the clinician’s perspective
Several observational studies in ICUs have verified that the ICU is a place where conflicts continue to occur. They arise commonly between the intensive care team and patients’ relatives (up to 85% of observed conflicts). Up to 45% of conflicts are within the team itself and only around 15% of observed conflicts are between the intensive care team and the patient himself.28–30 As Azoulay and colleagues showed in their study, many of the conflict scenarios appear especially due to inter-team miscommunication, misunderstandings or mistrust.28 In the same way, conflicts with the patients’ relatives often arise out of misunderstandings between staff and families.
The ICU teams described the effect of ethics rounds as beneficial in preventing and resolving conflicts in these both entities. Ethics rounds improved team communication merely by the presence of an impartial person as member of the rounding team and enabled a more open, more focused and much clearer discussion within the team, removing perceived barriers of communication due to hierarchical structures of ICU rounds and providing a better forum for discussion of perceived clinical or ethical critical care problems that otherwise might have gone unnoticed. Ethics rounds enabled the team to engage more thoroughly in the discussion on patients’ advance directives and their applicability for the given clinical situation.
Studdert et al showed in an observational trial in 2009 that conflicts between the critical care team and patients’ families arise more frequently in patients with prolonged intensive care treatment. Most of these conflicts deal with wishes for more aggressive or less aggressive treatment, that is, differences in perceived patient wishes and medically indicated treatment options, misunderstandings, especially about poor prognosis, and problems in identifying the patient’s main surrogate decision maker.31 The ICU teams experienced ethics rounds and family conferences moderated by the rounding ethicist as a valuable tool in ameliorating these potential sources for conflict. The ethicist in this scenario was already familiar with the patient’s current and previous medical history and had a clear understanding of the clinical scenario, problems and potential conflicts. By primarily using moderated family conferences in addition to ethics rounds, there was hardly any more need for consultations by the ethics committee to resolve inner-team or team-family discrepancies. Families involved in these moderated conferences gave very positive feedback on this way of cooperation and problem solving and showed high satisfaction with the decisions reached by these means. In summary, ethics rounds on the ICU have been shown to be a valuable addition and an improvement of care within the interdisciplinary team that is necessary to provide critical care on its highest level in this tertiary treatment centre.
Conclusion
We made the experience that by implementing ethics rounds in close cooperation with the respective clinical sections, we together were able to develop a more comprehensive account of ethics quality in our hospital and to better address the needs of the clinical sections. We saw effects on all three levels of ethics quality, whereas beforehand only very limited activities in individual patient-related cases have been possible. At the same time, the acceptance of other CES services seemed to benefit from this newly implemented structure insofar as we experienced a significant increase in requests for consultation. Only if CES services are successful in creating or improving a moral space within hospitals, in which clinicians ‘could more directly process their moral experience while still having to function in the complex, bureaucratic world that is our hospital’,32 33 will they be able to prove that there are reasons for their existence. Bottom-up approaches that address all levels of ethics quality in a hospital or an institution seem to be especially suited for this endeavour. However, research efforts are needed to verify our single-centre findings in this regard and to analyse its consequences on the practical, as well as on the theoretical level.

Number of requests for clinical ethics support per year stratified by the accompanied types of intensive care unit (ICU).

Stratification of requested clinical ethics support in the medical intensive care unit per year by modus of moderated meetings versus traditional clinical ethics consultation.

{kind=link}
{kind=link}
{kind=link}
Stratification of requested clinical ethics support in the interdisciplinary intensive care unit per year by modus of moderated meetings versus traditional clinical ethics consultation.
References
Footnotes
↵i Here, ‘top down’ explicitly refers to the design of CES discussions and the fundamental goal of decision-making, not to the way in which it is implemented (which can, of course, be either top-down or bottom-up).
Contributors All authors included on the paper fulfil the criteria for authorship (in accordance with the ICMJE recommendations).
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Other content recommended for you
- Interprofessional ethics rounds concerning dialysis patients: staff’s ethical reflections before and after rounds
- A report on small team clinical ethics consultation programmes in Japan
- Important outcomes of moral case deliberation: a Euro-MCD field survey of healthcare professionals’ priorities
- Objectives and outcomes of clinical ethics services: a Delphi study
- Morisprudence: a theoretical framework for studying the relationship linking moral case deliberation, organisational learning and quality improvement
- Ethics support in institutional elderly care: a review of the literature
- The Ethics Liaison Program: building a moral community
- Call to action: empowering patients and families to initiate clinical ethics consultations
- Taking the burden off: a study of the quality of ethics consultation in the time of COVID-19
- Optimising the documentation practices of an Ethics Consultation Service