Article Text

Abstract
In all fields of clinical medicine, there is an increasing awareness that outcome must be assessed in terms of quality of life and cost effectiveness, rather than merely length of survival. This is especially the case when considering decompressive craniectomy for severe traumatic brain injury. The procedure itself is technically straightforward and involves temporarily removing a large section of the skull vault in order to provide extra space into which the injured brain can expand. A number of studies have demonstrated many patients going on to make a good long-term functional recovery, however, this is not always the case and a significant number survive but are left with severe neurocognitive impairment. Unfortunately, many of these patients are young adults who were previously fit and well and are, therefore, likely to spend many years in a condition that they may feel to be unacceptable, and this raises a number of ethical issues regarding consent and resource allocation. In an attempt to address these issues, we have used the analytical framework proposed by Jonsen, that requires systematic consideration of medical indications, patient preferences, quality of life and contextual features.
Statistics from Altmetric.com
Introduction
Over the past two decades, there has been a resurgence of interest in the use of decompressive craniectomy for patients with traumatic brain injury (TBI), however, use of the procedure remains controversial. By temporarily removing a large segment of the skull, extra space is provided into which the injured brain can expand, and there appears little doubt that the procedure can reduce intracranial pressure. A number of studies have demonstrated that many patients go on to make a good long-term recovery, however, this is not always the case.1 ,2 A very significant number of patients survive but remain severely disabled, and to what degree that outcome is acceptable to those patients is difficult to establish.
A recent study found that for patients who had survived having had a decompressive hemicraniectomy for ischaemic stroke, retrospective consent would not have been obtained from those patients who were left with a very poor functional status.3 Currently, the same cannot be said for those patients who survive a serious TBI, however, this does raise a number of ethical considerations. Many of these patients are young adults who were previously fit and well and, as such, are likely to live for many years in a condition that they feel to be unacceptable. In addition, their level of dependency places a considerable burden not only on their immediate family but also on the wider community.
In an attempt to address these issues, we have used the analytical framework proposed by Jonsen, that requires systematic consideration of medical indications, patient preferences, quality of life and contextual features.4
Medical indications
It is likely that decompressive craniectomy will remain a valuable tool in the management of patients with severe TBI, however, there continues to be a debate regarding surgical indications and patient selection. While it has to be acknowledged that raised intracranial pressure following TBI is highly predictive of mortality or poor long-term outcome, obtaining a lower intracranial pressure by surgical decompression does not necessarily translate into an improvement in outcome, and this is for two reasons. In the first instance, there is the issue of surgical morbidity.
Surgical morbidity
Performing a decompressive craniectomy is technically straightforward, however, there is an increasing awareness that the procedure is associated with a significant number of complications.5 This was confirmed by the recent DECRA study that compared early bifrontal decompression with standard medical therapy for patients with severe TBI.6 The trial findings were that while the intracranial pressure was lower in patients in the surgical arm of the trial, their outcome was worse than those patients who received standard medical therapy. There has been considerable criticism of the trial, the most notable of which was the relatively low and transient intracranial pressure threshold at which patients were randomised (intracranial pressure (ICP)>20 mm Hg for more than 15 min). This has led many observers to state that the patients on whom decompressive surgery was performed were not representative of current clinical practice.7 However, this fails to recognise the hypothesis on which the trial was based, which was that early ‘prophylactic’ decompression would lower the intracranial pressure, reduce secondary insults and improve outcome. At the time of inception, the study was based on genuine clinical equipoise, and if early decompression had provided benefit, then rather than the patients in the trial not being representative of normal clinical practice, the patients in the trial would in fact have come to represent the clinical practice of the future, and this would have had significant impact on neurosurgical resources. What the trial has clearly established is that when there is relatively mild and transient intracranial hypertension, any benefit obtained by surgical decompression is offset by surgical morbidity.8
What remains to be established is the of role decompressive craniectomy when the intracranial pressure continues to rise above 20 mm Hg and beyond, and the ongoing RESCUEicp (Randomised Evaluation of Surgery with Craniectomy for Uncontrollable Elevation of Intra-Cranial Pressure) hopes to address this issue.9 Notwithstanding the outcome of this trial, the interpretation of any clinical trial attempting to demonstrate an improvement in outcome over and above standard medical therapy must be tempered with the realisation that this is not necessarily a reflection of clinical practice. In most centres, a decompressive craniectomy is carried out, not so much as to prevent secondary brain injury, but rather, once all medical therapy has failed and the patient is thought unlikely to survive without surgical intervention. This raises two important, and perhaps, insurmountable ethical issues. In the first instance, once a patient has failed medical therapy, can they realistically be randomised to further medical therapy? Second, while many patients survive and go on to make a good functional recovery, a significant number remain severely disabled. This raises the issue of the severity of the primary brain injury and patient selection.
Importance of primary brain injury in determining final outcome
In the second instance, a number of studies have demonstrated that in the context of intractable intracranial hypertension that does not respond to medical therapy (>30 mm Hg), surgical decompression can be potentially lifesaving.1 ,2 Unfortunately, there has to come a point where the primary brain injury is so severe that if the patient survives they are highly likely to remain severely disabled. Until recently, the difficulty has always been that of how to make an accurate and objective assessment of the severity of the primary brain injury so that appropriate clinical decisions can be made regarding patient selection. The recently developed CRASH collaborators web-based outcome prediction model has gone some way to address this issue.10 Based on data collected on the 10 000 patients in the CRASH steroid trial,11 the model provides a predicted risk of an unfavourable outcome at 6 months following TBI (unfavourable outcome is defined by the Glasgow Outcome Scale (GOS) as: severely disabled, vegetative state or dead).
Previous studies have shown how the predicted risk of unfavourable outcome can be used to stratify patients according to injury severity, thereby acting as a surrogate index of injury severity.12 When the predicted risk (or injury severity) is relatively low, the majority of patients are observed to achieve a favourable long-term outcome (defined by the GOS as good outcome or moderately disabled) (figure 1). As the predicted risk increases, so does the likelihood of unfavourable long-term outcome; and once the prediction of an unfavourable outcome is greater than 80%, most patients either died or survived with severe disability, or ended up in a permanent vegetative state.
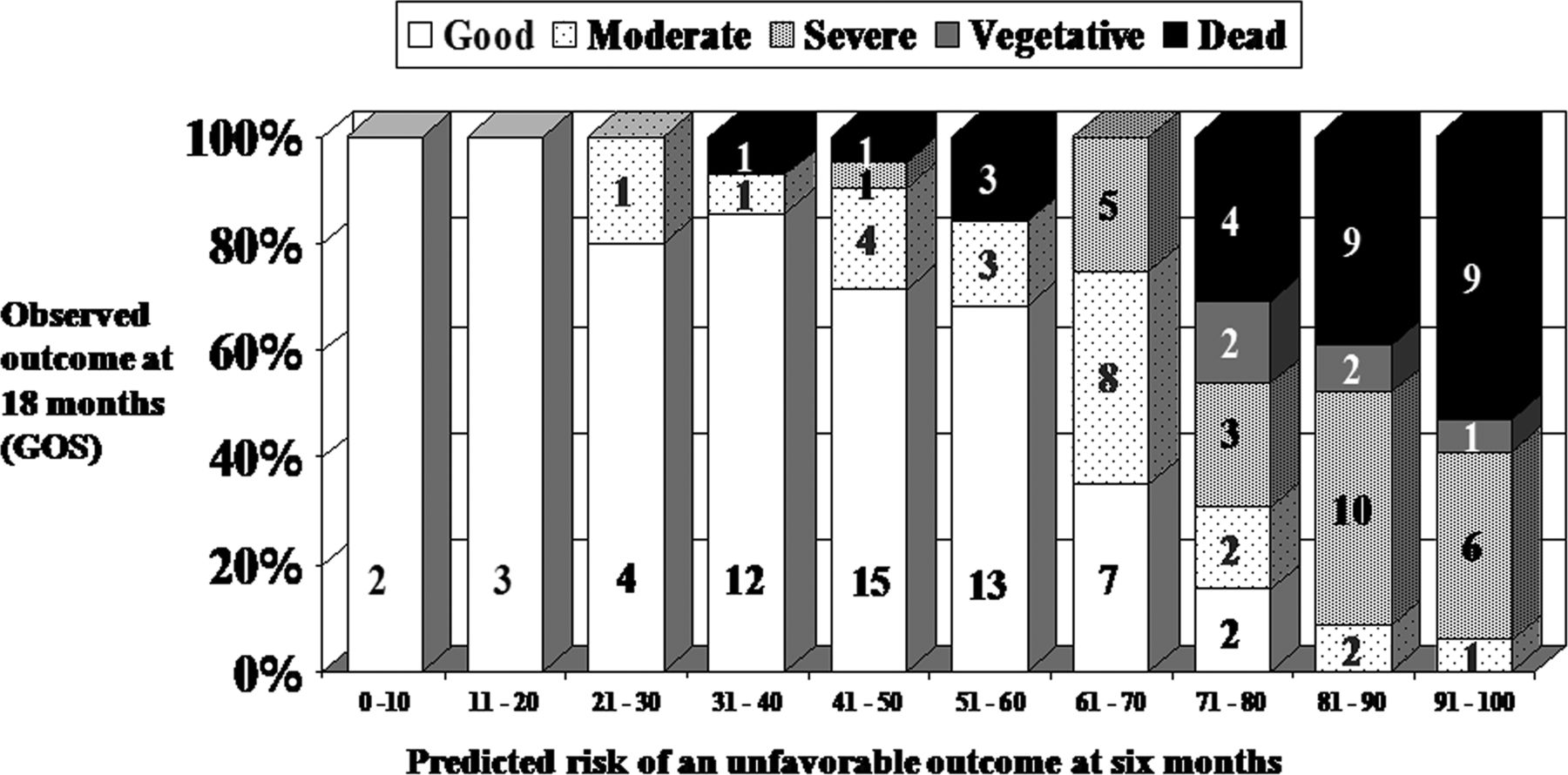
Outcome stratified according to severity of primary cerebral injury. The prediction of an unfavourable outcome at 6 months (x axis) and the observed outcome at 18 months among 137 patients on whom follow-up was available. Numbers within the bar chart represent absolute patient numbers. (Reproduced with kind permission, Mary Ann Liebert, Inc., publisher).
On superficial examination, this data would appear to provide compelling evidence that surgical decompression should not be performed on those patients with a high predicted risk of unfavourable outcome. However, from a patient's perspective, there are two issues that require careful consideration. In the first instance, probability is not equivalent to certainty. Although the most likely outcome if the patient survives may be one of severe disability, there will always be a chance, no matter how small it is, of a good outcome. Second, we should not necessarily assume that survival with severe disability is unacceptable to our patients. This leads us to consider the next component of the ethical framework; that of patient preferences.
Patient preferences
Everyone has the right to make decisions regarding their health and medical treatment, and the importance placed on the need to obtain informed consent is a reflection of those rights and individual preferences. This requires that an individual has a clear understanding of the facts, implications and future consequences of an action, and has sufficient reasoning faculties, such that they are competent.13 When considering decompressive surgery for severe TBI, these principles are challenged because the patients themselves will be in no position to participate in any discussion regarding treatment options. The fundamental question is, what we would want for ourselves if we were unfortunate enough to be in this position. On one hand, there is the chance of a good functional recovery. On the other hand, there is the possibility of survival in a state we may find to be unacceptable. As severity of the primary injury increases (as adjudged by the prediction of an unfavourable outcome), so does the possibility of that outcome occurring. If survival with severe disability is deemed unacceptable, the obvious question relates to the stage at which one would say that the risk of that outcome occurring is so high that most people would not give their consent for the procedure.
In an attempt to address this issue, a number of studies have explored whether access to accurate objective information on outcome data, as shown in figure 1, would affect a person's willingness to provide consent for lifesaving, but potentially non-restorative surgery. The study was initially conducted among a small group of neurosurgeons and intensivists who were very familiar with the procedure.14 Thereafter, the study was expanded to involve a wide variety of healthcare workers many of whom were unfamiliar with the surgical procedure and outcome following severe TBI.15 The studies consisted of a two-part structured interview in which the participants were shown three clinical cases. They were provided with clinical details (eg, age, initial Glasgow Coma Scale, pupillary response, presence of other injuries) and initial radiological findings. They were told that the injury severity was progressively worse from cases 1 to 3, but were given no other information regarding prognosis. The participants were presented with a situation in which the patient has had progressively rising intracranial pressure despite maximal medical management, and consideration was being given to decompressive surgery as a lifesaving procedure. They were then asked to rate their opinion regarding surgical intervention using a simple visual analogue scale that measured from 1 to 10. (1—strongly disagree, 10—strongly agree). A number of scenarios were provided, and in one of these scenarios, the participants themselves were the injured parties. The implication which was clearly stated, was whether they would provide consent if they were the patient, based on what they perceived to be the most likely outcome, and whether that outcome would be acceptable. They were then shown the predicted and observed risks of unfavourable outcome (figure 1), and the participants were then asked to rate their opinions again based on their interpretation of this data.
The results of these studies were that all participants, irrespective of age, religion and background were strongly influenced by an objective assessment of outcome, and the majority of the participants were of the opinion that survival with severe neurological disability would be unacceptable for themselves.
The obvious question is whether the results of these studies are a true representation of the preferences of these healthcare workers if they were unfortunate enough to actually find themselves in these circumstances. On superficial examination, it seems that the criteria for informed consent would have been fulfilled. The participants were interviewed in a controlled setting, and the circumstances and the severity of the injury, as adjudged by the prediction model, was clearly established. The observed outcome data at 18 months provided clear information about the implications and future consequences of surgical intervention, and presumably, all participants were competent. However, while it could be suggested that surgical intervention should be withheld for all patients when the predicted risk of an unfavourable outcome is extremely high, there are a number of issues that require consideration. In the first instance, these surveys were conducted entirely among healthcare workers, and these preferences may not necessarily reflect those of the general population. For example, previous studies have shown that healthcare professionals are considerably less likely than the general public to want cardiopulmonary resuscitation (CPR) for themselves, and although this may reflect a greater insight or knowledge, it does not change the fact that their preferences are different.16 Furthermore, these differences may not necessarily be due to the clinical experience, but rather, may be a reflection of the different socio-demographic background that healthcare workers have from the general population.17 A final consideration is that there may be a significant bias towards cognitive competence among healthcare workers because this is critical to their professional life and identity. Notwithstanding these limitations, if we acknowledge that these observations cannot necessarily be extrapolated to the general population (and further work will be require in order for this to be confirmed), it is still not possible to adopt the position that among healthcare workers, surgical intervention should be withheld until we consider the next component of the ethical framework, that of quality of life.
Quality of life
Although there is an increasing awareness of the need to evaluate quality of life as an outcome measure, it must be acknowledged that there are significant limitations when making abstract statements such as ‘I would rather be dead than alive with severe disability’. In the first instance, competent people do not necessarily accurately predict what they will later find acceptable or unacceptable as quality of life, and this was clearly demonstrated by the SUPPORT study.18 When actually faced with the choice of life and death, most people choose life. Furthermore, many people do adapt to unfortunate events in life by ‘re-calibrating’ and learning to accept a degree of disability they would previously have adjudged as unacceptable. In addition, despite the considerable progress in the development of documentation, such as advance directives and living wills, both of which aim to validate the healthcare wishes of competent persons in the event of them becoming incompetent, a number of studies have demonstrated that these directives may have some limitations in the clinical setting.19 ,20 In the context of severe TBI, the individuals involved are most likely to be young adults, and even if they had discussed their wishes were they to be involved in such a situation, they are highly unlikely to have had these actually documented. In these circumstances—and it is quite likely— an authorised third-party decision maker who had prior knowledge of these preferences may provide an effective means for making such difficult decisions.
A second consideration is quality-of-life assessment. Not only is this difficult to define, but it may vary depending on who is making the evaluation. For example, physicians consistently rate their patients’ quality of life lower than the patients rate themselves. In addition, several long-term studies have documented that some patients may make continuous improvement for many years after the initial TBI.21 Our previous study also showed that delayed neurological recovery after 6 months, from unfavourable outcome to favourable outcome, occurred at least in 25% of the patients who had had a decompressive craniectomy.22 What remains to be established is whether those who remained severely disabled at 18 months after decompressive craniectomy go on to make further neurological improvement beyond 18 months, and this must be the focus of future research.
A final consideration is how those patients who survive with severe disability perceived their own quality of life and, unfortunately, while this is the most important information, it is also the most difficult to obtain. Any subjective data is likely to be biased towards those patients who are able to understand the questions and communicate their answers effectively. Indeed, it may have to be accepted that attempts at obtaining a perceived quality-of-life assessment from those patients who remain minimally conscious or in a vegetative state may be unrealistic. Recent studies have suggested that some of these patients may actually have higher levels of awareness than was previously realised, and functional imaging has suggested that there may be potential for re-establishment of neural networks.23 ,24 What has yet to be determined is the clinical significance of these findings. While the activation of neuronal networks in response to clinical stimulation may form the basis of neurological recovery, this may not necessarily be perceived as beneficial. Indeed, increasing awareness of their situation may either promote a sense of belonging, or may only serve to emphasise their social isolation.25 Likewise, complex neuro-imaging may demonstrate neuronal activation that has no functional correlation with outcome, let alone quality of life.
More work will obviously be required to establish the clinical significance of some of these findings, and also to continually develop rehabilitation strategies that may improve outcome, however, the final component that requires consideration is the burden placed on society. This leads on to the final aspect of the framework, that of contextual issues.
Contextual issues
Although accepting that the category of severe disability covers a wide range of neurological functions, these patients have, by definition, lost their independence. Many will require 24 h care in either a nursing home, rehabilitation facility or in a supportive home environment, and this will place a considerable burden on the healthcare system. Justifying this, use of resources has to balance two seemingly opposite positions. In the first instance, there is a utilitarian approach which acknowledges that all healthcare systems have resources limitations, and any medical intervention must always be justified by clinical evidence of benefit at a reasonable cost to the community. This manifests as traditional cost effectiveness by which the cost of each service should be weighed against some measure of benefit. There are, however, a number of difficulties when comparing a neurosurgical procedure, such as decompressive craniectomy, with other treatments that have to justify cost effectiveness, such as organ transplantation or expensive chemotherapy. In the first instance, the decision to decompress must be made in the context of acute neurotrauma in which there is limited time to consider not only the long-term outcome but also the long-term resource implications. Second, the procedure itself is technically straightforward, and the costs incurred at the time are no more than most routine neurosurgical procedures. It could be argued that because of the burden of long-term survival with severe disability, the procedure should be withheld entirely. However, if this were the case, then the possibility of a good outcome would be denied to those patients who obtain clinical benefit from appropriate and timely decompression. It is for these reasons that clinically useful information can be obtained by stratifying patients according to the severity of the primary brain injury.
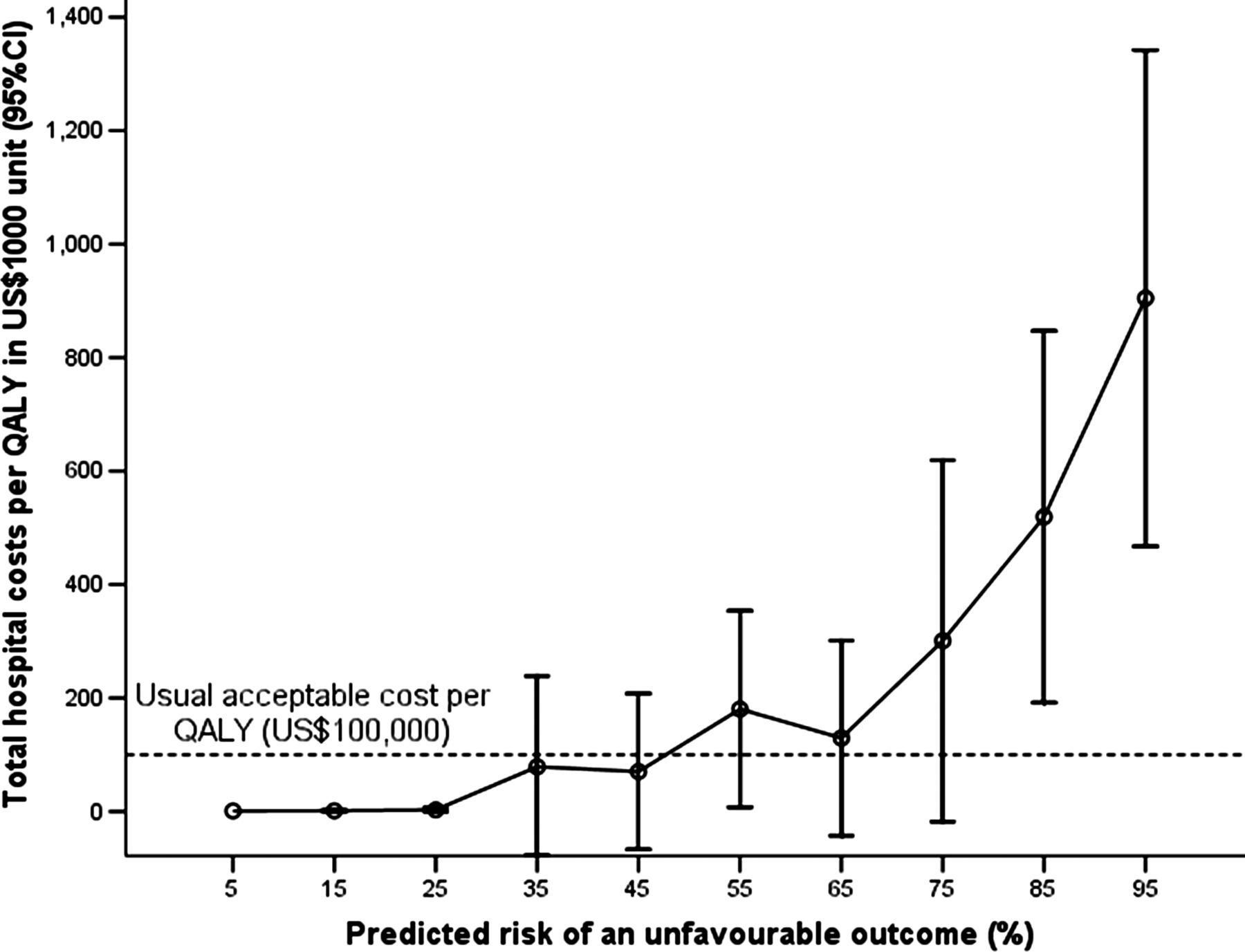
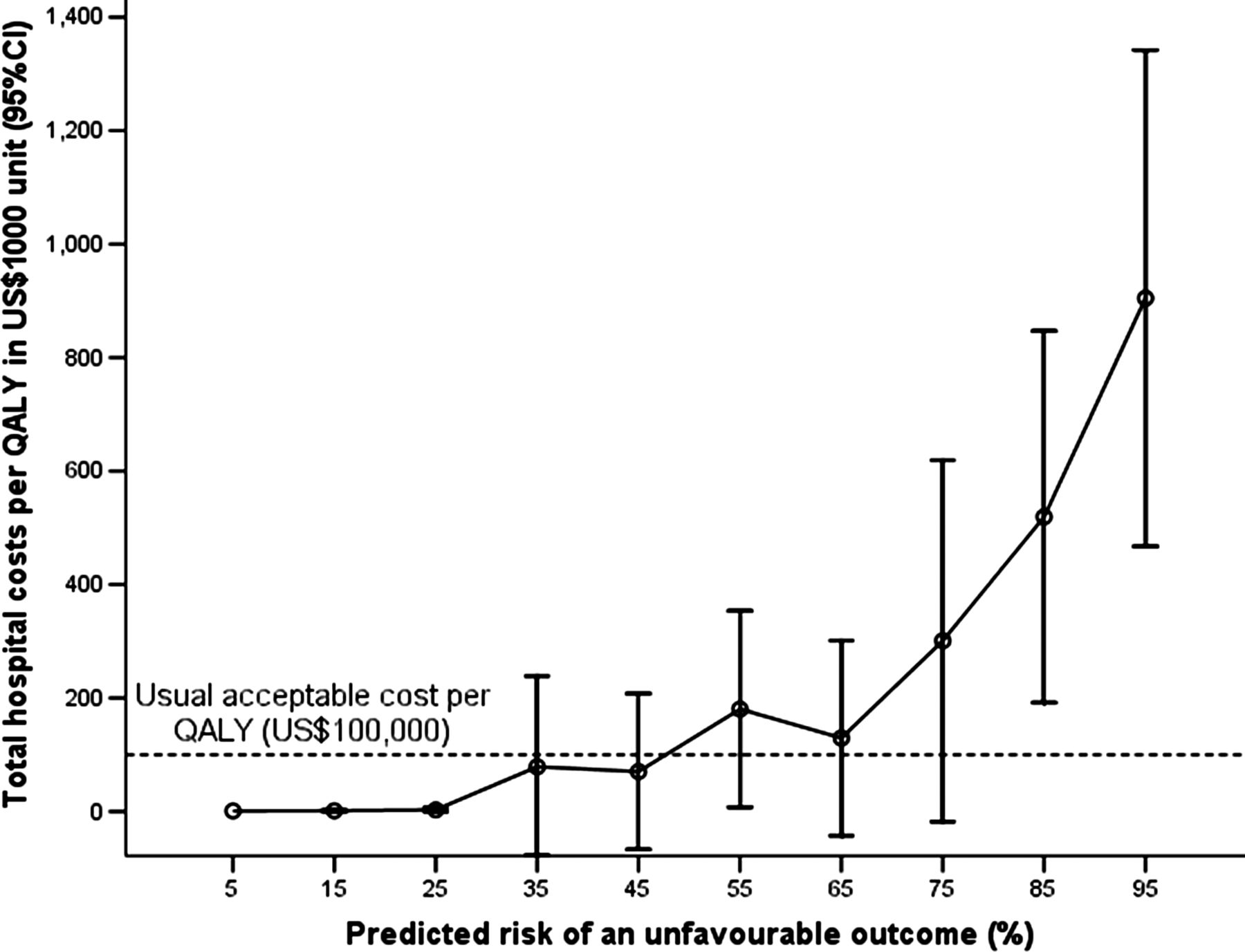
A previous study has investigated the cost per quality-adjusted life-year (QALY) for 168 patients who had had a decompressive craniectomy for severe TBI between 2004 and 2010 in Perth, Western Australia.26 The CRASH collaborators model was used to stratify patients according to injury severity, and as shown in figure 2; as the severity of injury increases, so does the cost per QALY.26
{kind=link}
{kind=link}
Estimated total hospital costs including neurosurgical procedural costs per quality-adjusted life-year (QALY) in US $1000 unit for 168 patients who had had a decompressive craniectomy in Western Australia between 2004 and 2010. Patients are stratified by the severity of illness in predicted risk of an unfavourable outcome.26 (CI). (Reproduced with kind permission, Lippincott Williams & Wilkins, Inc., publisher).
From a purely utilitarian standpoint, it is difficult to justify lifesaving intervention when the probable outcome is severe disability, with that individual reliant on long-term medical and nursing care at considerable cost to society. However, this position fails to recognise that conveying the message that life is precious and worth a great deal of effort to preserve is in itself a source of social utility. People obtain benefit from the belief that they live in a compassionate society caring for the needs of each constituent member, and where those in most desperate need of help will not be ignored merely on the basis of cost. This principle is manifested in the rule of rescue which describes the ethical imperative to intervene in an attempt to save the life of a young person even when the money and resources might be more efficiently used elsewhere.27 ,28 The difficulty comes when the procedure is no longer able to achieve an acceptable outcome for the individual, and their families and the community are left with a large psychological and financial burden.
Conclusions
Overall, it would appear that for carefully selected patients, there is a medical indication for performing a decompressive craniectomy following severe TBI. The development of a reliable outcome prediction model allows patients to be stratified according to injury severity, and by comparing the predicted risk with the observed long-term outcome it is possible to provide an objective assessment of the most likely outcome for those patients who require decompression. This information may be clinically useful when considering patient preferences and resource implications. However, it must be recognised that there are limitations when making abstract judgements based on what, by definition, must be historical data. While further research will be required to establish the role of decompressive craniectomy in the management of severe TBI, a broader debate is required into outcome prediction and the use of a medical intervention that may leave a person, not only in a condition that they may feel to be unacceptable, but that also places a considerable burden on society.
References
Footnotes
-
Contributors All authors contributed equally to the preparation of this manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Commentaries
- The concise argument
Other content recommended for you
- Neurotrauma and the rule of rescue
- Long-term survival with unfavourable outcome: a qualitative and ethical analysis
- Traumatic brain injury in adults
- Traumatic brain injuries in older adults—6 years of data for one UK trauma centre: retrospective analysis of prospectively collected data
- IMPACT and CRASH prognostic models for traumatic brain injury: external validation in a South-American cohort
- Survival after traumatic brain injury improves with deployment of neurosurgeons: a comparison of US and UK military treatment facilities during the Iraq and Afghanistan conflicts
- Neuropsychological outcomes following traumatic brain injury
- Traumatic subdural haematoma: integrating case-based clinical judgement with guidelines
- Prospective observational cohort study on epidemiology, treatment and outcome of patients with traumatic brain injury (TBI) in German BG hospitals
- Acute subdural haematoma in the elderly: to operate or not to operate? A systematic review and meta-analysis of outcomes following surgery