Article Text

Abstract
The distribution of scarce healthcare resources is an increasingly important issue due to factors such as expensive ‘high tech’ medicine, longer life expectancies and the rising prevalence of chronic illness. Furthermore, in the current healthcare context lifestyle-related factors such as high blood pressure, tobacco use and obesity are believed to contribute significantly to the global burden of disease. As such, this paper focuses on an ongoing debate in the academic literature regarding the role of responsibility for illness in healthcare resource allocation: should patients with self-caused illness receive lower priority in access to healthcare resources? This paper critically describes the lower priority debate's 12 key arguments and maps out their relationships. This analysis reveals that most arguments have been refuted and that the debate has stalled and remains unresolved. In conclusion, we suggest progression could be achieved by inviting multidisciplinary input from a range of stakeholders for the development of evidence-based critical evaluations of existing arguments and the development of novel arguments, including the outstanding rebuttals.
- Allocation of healthcare resources
- allocation of organs/tissues
- health care for specific diseases/groups
Statistics from Altmetric.com
- Allocation of healthcare resources
- allocation of organs/tissues
- health care for specific diseases/groups
The distribution of scarce healthcare resources is an increasingly important issue due to factors such as expensive ‘high tech’ medicine, longer life expectancies and the rising prevalence of chronic illness. Part of the healthcare resource allocation debate centres on the question of whether individual patient characteristics should be considered in decision-making.1 Characteristics proposed to be relevant include: (1) an individual's relationship to others (eg, the individual is a criminal, has dependents or rare skills); (2) an individual's personal attributes (eg, gender or cultural background); and (3) an individual's relationship to their illness (eg, the individual's disease is due to genetic, environmental, or lifestyle factors).1
Characteristic three, the individual's relationship to their illness, is particularly pertinent to the current healthcare context in which lifestyle-related factors such as high blood pressure, tobacco use and obesity are believed to contribute significantly to the global burden of disease and individual behaviour is seen as a responsible for many health problems.2 3 As such, this paper focuses on an ongoing debate in the academic literature regarding the role of responsibility for illness in healthcare resource allocation: should patients with self-caused illness receive lower priority in access to healthcare resources?
This debate began in earnest during 1991 with the publication of opposing papers by Moss and Siegler4 and Cohen and Benjamin5 in the Journal of the American Medical Association. Moss and Siegler4 argued that patients with alcohol-related liver disease should have lower priority in access to liver transplantation, while Cohen and Benjamin5 argued the contrary. In 1993, the debate gained momentum with the publication of two further papers in the British Medical Journal for6 and against7 a lower priority for smokers in access to coronary artery bypass surgery. These articles prompted numerous letters to the editor in subsequent issues of the British Medical Journal.8–24 Currently, the debate remains unresolved and new articles continue to emerge (eg, Ho 2008,25 Feiring 2008,26 Glannon 200927). One factor hindering the progression of the lower priority debate is the lack of an overall description or ‘map’ detailing the nature of the arguments and their relationships. Therefore, the primary purpose of this article is to present a comprehensible and comprehensive ‘map’ of the debate. In conclusion, the analysis reveals that the debate has stagnated and suggestions for new ways forward are briefly discussed.
Method
Articles containing lower priority arguments were identified by a literature search using PubMed and Google Scholar (up to June 2009). Search terms included: ‘priority’, ‘responsibility’, ‘resource allocation’, ‘responsibility for health’, ‘liver transplantation’, ‘heart’, ‘alcoholism’ and ‘ethics’. In addition, reference lists of identified articles were hand searched. Analysis consisted of the extraction of pro- and anti-lower priority arguments and the determination of differences, similarities and relationships. Critical descriptions of the arguments and a map of relationships between arguments were produced and are the basis of this analysis.
Critical descriptions of the lower priority arguments
The medical argument
The medical argument is concerned with the efficient use of resources by maximising benefits gained from medical treatment. This argument asserts patients with self-inflicted illness (eg, obesity-related disease)26 should have lower priority in access to health care because they are more likely to experience poor medical outcomes. For example, some argue that the best use of resources is achieved by giving smokers lower priority in access to coronary bypass surgery because they have higher rates of coronary artery disease recurrence and re-operation, and a higher risk of postoperative complications compared with non-smokers.6 10 13 17 19 28–31
Counter argument 1: the no evidence argument
In opposition to the medical argument, the no evidence argument says there is no evidence to support the claim that unhealthy behaviours such as smoking or excessive alcohol consumption result in poorer medical outcomes.5 11 12 20 22 32–38 For instance, proponents of the no evidence argument cite studies that show similar survival rates and transplant rejection rates for alcohol-dependent and non-alcohol-dependent individuals following liver transplantation.34 36 39 40
Counter argument 2: the no precedent argument
The second counter to the medical argument is the no precedent argument. This argument claims that there is no precedent in health care to support prioritisation on the basis of anticipated medical outcome. For example, some argue it is unfair to give alcohol-dependent individuals or smokers lower priority in access to healthcare resources when other patients with predicted poorer medical outcomes (such as those with hypertension, diabetes, older age, female gender, obesity, or hypercholesterolaemia) are not.5 7 23 35
The policy arguments
The policy arguments are concerned with the broad social effects of resource allocation decisions involving patients with self-caused illness. The policy arguments include the behaviour change argument and the public support argument.
The behaviour change argument
The behaviour change argument claims that the threat of lower priority will generally encourage healthy behaviour/discourage unhealthy behaviour.41 For instance, some argue that policies that deny smokers coronary bypass surgery or refuse/reduce benefits paid for chronic respiratory disease care are likely to encourage smokers to give up smoking.13 42 Others even argue that a policy of equal access would cause irresponsible health behaviour.43
The public support argument
The public support argument predicts a decline in public support for particular healthcare resources due to a perception of injustice if those who have caused their own ill health are given equal access. The public support argument is particularly concerned with healthcare resources that require altruistic public donations such as liver donations for transplantation will decline if alcohol-dependent patients with alcohol-related liver disease are allowed equal access to transplantation.4
Counter argument 1: rebuttal of the public support argument
This rebuttal counters the public support argument by asserting that public attitudes are not a morally defensible basis for policy. This is because public attitudes may be based on prejudices rather than factual information.32 37 44 For example, Shelton and Balint44 reason that if public opinion is racist, policy based on public opinion may unethically disadvantage certain racial groups.
The moral arguments
The moral arguments are concerned with the individual's moral responsibility to maintain their own health. There are two moral arguments: (1) the harm argument, which focuses on individuals' obligation to others and (2) the self-respect argument, which focuses on individuals' responsibility to themselves.
The harm argument
The harm argument claims that patients with self-inflicted illness should receive lower priority because ‘innocent’ patients (ie, patients who did not cause their illness) will be harmed if equal access is allowed. This is because patients with self-caused illness will deprive ‘innocent’ patients of resources that would have otherwise been theirs'.4 17 26 30 43 45 46 Therefore, the harm argument implies that individuals have a moral obligation to others to maintain their health because ‘inequalities in health expectancies that derive from unchosen features of people's circumstances are unjust and should be compensated, while inequalities that reflect personal choices of lifestyle may not.’26 33
The self-respect argument
The self respect argument claims that individuals have a moral responsibility to themselves to maintain their health. According to the self-respect argument, it is the failure of patients with self-caused illness to fulfil this responsibility that justifies giving them lower priority in access to healthcare resources.17 42 47 48
Assumptions underlying the moral arguments
The moral arguments rest on two assumptions: (1) that a link exists between unhealthy behaviour and responsibility for ill health; and (2) that responsibility for illness logically results in a decreased claim to healthcare resources. These assumptions (and therefore the moral arguments generally) are countered by the not responsible argument and the role of the healthcare professional argument, respectively.
Counter argument 1: the not responsible argument
The not responsible argument challenges the moral arguments' assumption that a link exists between unhealthy behaviour and responsibility for ill health with three reasons for why patients should not be held responsible for their illness. These reasons are: (1) the inability to control unhealthy behaviours (‘the no control reason’); (2) the existence of other, uncontrollable, risk factors for ill health (‘the other causes reason’); and (3) the value of risk-taking (‘the value reason’).
Reason 1: the no control reason
The first reason why patients are not responsible for their ill health suggested by the not responsible argument is that individuals are not in control of their unhealthy behaviour. For instance, some claim patients are not responsible for their unhealthy behaviours because many such behaviours are addictive,7 14 35 41 44 49–51 occur as a result of mental illness,32 50 or are influenced by forces such as culture and advertising,8 12 14 32 41 52 or biology/genetics.32 41 44 51 53
Reason 2: the other causes reason
The second reason proposed for why those with self-caused illness are not responsible for their ill health is that unhealthy behaviour is not the sole cause of illness. For example, Olsen49 argues that smokers cannot be held responsible for their lung cancer because, in addition to the unhealthy behaviour of cigarette smoking, numerous uncontrollable risk factors such as environmental radiation, air pollution and genetics may contribute to the incidence of lung cancer.
Reason 3: the value reason
The third reason offered for the rejection of responsibility for ill health is that unhealthy behaviours should sometimes be allowed or excused because there is positive value to risk-taking behaviour.21 37 21 37 53 For example, Martens53 argues that risk-taking behaviour can play an important role in maintaining psychological wellbeing as strict risk-avoidance can cause fear and anxiety.21 37
Counter argument 2: the role of the healthcare professional argument
The role of the healthcare professional argument questions the moral arguments' assertion of the logical connection between responsibility for illness and a decreased claim on healthcare resources by (1) ‘the trust reason’ and (2) ‘the non-judgement reason’.
Reason 1: the trust reason
The trust reason claims that linking responsibility for illness with a decreased claim on healthcare resources (eg, a lower priority policy for those with self-inflicted illness) should not be allowed because it would inhibit trust between the patient and their healthcare professional.36 44 The trust reason asserts that the quality of healthcare would be compromised because patients could not trust their physician with important information regarding their unhealthy behaviours for fear of receiving lower priority.36 44
Reason 2: the non-judgement reason
The non-judgement reason claims that a lower priority policy is unethical because it would require healthcare professionals to perform an inappropriate role judging or punishing patients. According to this reason, healthcare professionals should treat patients irrespective of the cause of illness, solely on the basis of medical need.9 14–16 18 20 22 24 32 35 37 40 50
The impracticality of application argument
The impracticality of application argument claims a policy of lower priority could not be implemented because it would be impossible or impractical to determine each patient's level of responsibility for ill health. There are four reasons why determining responsibility is said to be impractical or impossible: (1) ‘the time reason’; (2) ‘the bias reason’: (3) ‘the confounding factors reason’; and (4) ‘the foresight reason’.
Reason 1: the efficiency reason
The first reason why determining responsibility for illness is proposed to be impractical or impossible is because it would result in an inefficient use of time and/or resources. For example, Benjamin33 and Martens53 claim the determination of patient responsibility would be impractical or impossible due to the large amount of time and resources needed to gather the required information (eg, education, coping styles, cultural background, etc.).
Reason 2: the bias reason
The second reason this task is thought to be impractical or impossible is that it would be impossible to determine responsibility fairly for illness because of the influence of social biases against some unhealthy behaviours such as alcoholism.51
Reason 3: the confounding factors reason
The third reason suggested is that it would be impossible or impractical to determine the extent or degree to which unhealthy behaviours have contributed to ill health when there are confounding factors such as viral infections or predisposing medical conditions32 and genetic or environmental factors.41 54 For example, Aulisio and Arnold argue that the determination of responsibility would be impossible due to ‘insurmountable practical difficulties’ in ‘determining the degree to which a person's illness may be due to genetic or environmental factors over which she may have had no control’.54 279
The universalisation argument
The universalisation argument claims a lower priority policy would only be fair if it applied to all self-caused ill health, such as illness resulting from diet and sedentary lifestyle, employment in stressful or dangerous jobs, participation in dangerous sports, and the use of power tools or the ownership of large dogs. The universalisation argument concludes that a universal lower priority policy would be morally absurd due to the large number of dangerous activities that would need to be covered.7 34 41 44
Map of the lower priority debate
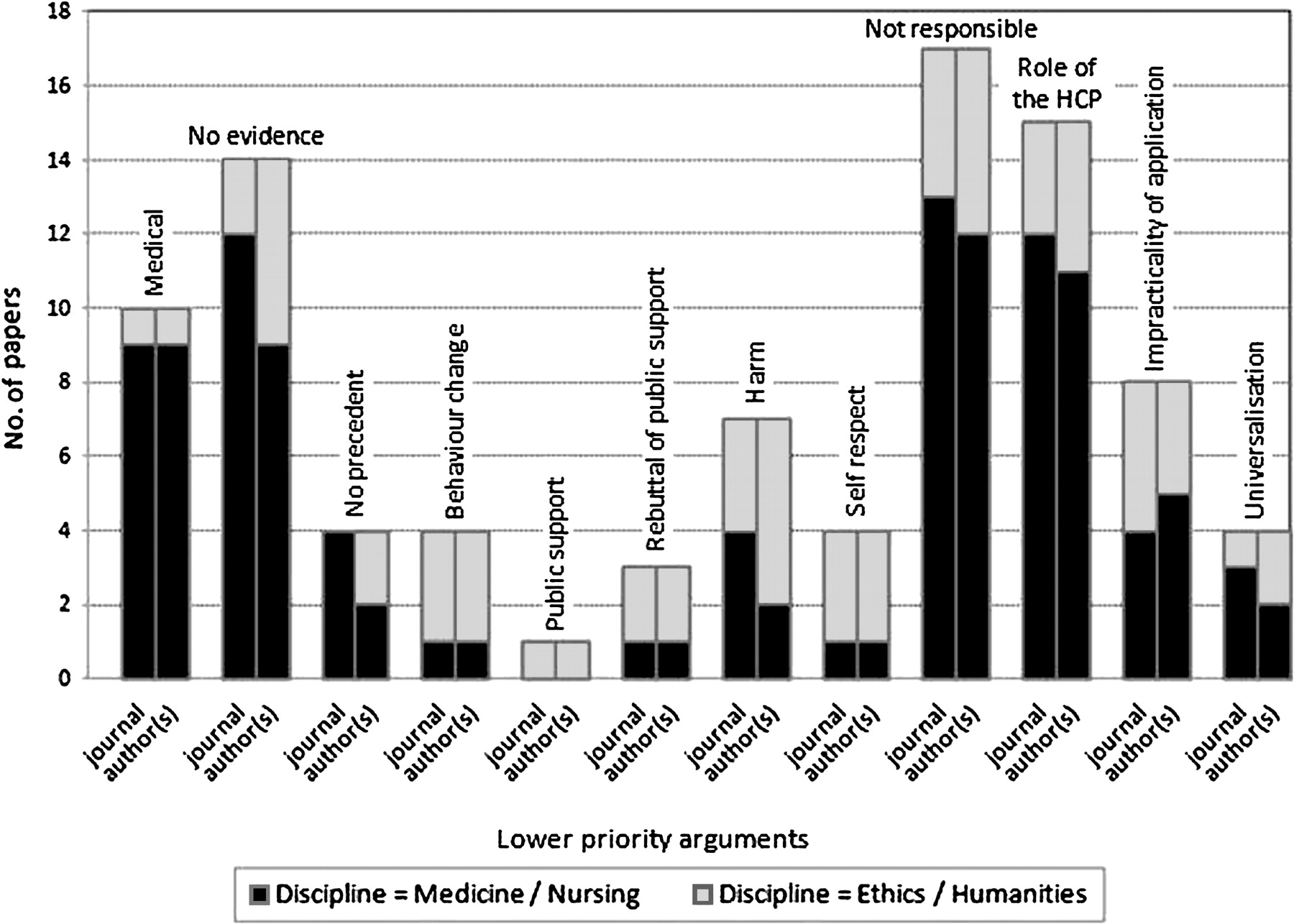
A visual representation or ‘map’ of the lower priority debate is presented in table 1 to complement the critical descriptions presented above. This map shows the pro and anti-lower priority arguments and their respective counter arguments (or lack of). In addition, figure 1 demonstrates the number of articles that assert each of the lower priority arguments as well as the discipline (‘medicine/nursing’ or ‘ethics/philosophy’) of their author(s) and journal of publication.
Map of the lower priority debate

{kind=link}
The number of articles that assert each argument and the discipline of their author(s) and journal of publication. (HCP = healthcare professional)
Suggestions for progression of the lower priority debate
Overall, this analysis reveals that the lower priority debate has stagnated. After almost 20 years of academic debate, recently published articles only re-emphasise previously presented arguments. For example, Ho55 re-presents the no evidence, the not responsible, the impracticality of application, and the role of the healthcare professional arguments, and Glannon25 re-presents the moral argument in favour of lower priority. Given the o-going importance of resource allocation and the trend in medical research towards identifying more lifestyle contributions to disease, this is a significant problem and progression of the debate is needed. We suggest at least the following: (1) evidence-based critical evaluation of existing arguments; (2) development of novel arguments, including responses to the as-yet-unrefuted arguments; and (3) multidisciplinary input from a range of stakeholders.
Evidence-based critical evaluation of existing arguments
As shown in table 1 and figure 1, there are seven original arguments and five rebuttals published in over 50 articles in the lower priority debate to date. Despite this, these existing arguments are generally underdeveloped. This is because they have mostly been published in brief letters to the editor,8–24 31 47 or in papers that spread their efforts across the assertion of multiple arguments.32 35 44 Therefore, one avenue for progression is the further critical evaluation and development of the existing arguments (with support from sound empirical evidence when appropriate).
Development of novel arguments, including responses to the unrefuted arguments
The second suggestion for the progression of the debate is the development of novel lower priority arguments including rebuttals of the as-yet-unrefuted arguments: the behaviour change, the impracticality of application and the universalisation arguments (table 1). This could begin with a re-appraisal of the scope of existing rebuttals in terms of their ability to counter multiple arguments. For example, although there is no direct counter to the behaviour change argument, the no evidence argument could provide a pre-emptive rebuttal because, if the no evidence argument's claim that there is no evidence to support the claim that unhealthy behaviours result in poorer medical outcomes was substantiated, there would be no need to consider the behaviour change argument.
Multidisciplinary input from a range of stakeholders
Finally, the debate has been dominated by the field of medicine, with most articles authored by medical professionals and/or published in medical journals (figure 1). We anticipate a collaborative, multidisciplinary approach to the processes already described (ie, the critical evaluation of existing arguments and the development of new arguments/rebuttals) will be key to the development of the lower priority debate. This is because stakeholders such as healthcare consumers, a broad range of healthcare professionals, ethicists, behavioural scientists, sociologists, health economists and policy-makers will bring new concepts (eg, culture, power, class, gender), theoretical frameworks (eg, theories about behaviour change and coping styles) and methods (eg, economic analysis and qualitative research methods) to the currently stagnant debate.
Conclusion
Our analysis has identified, described and mapped the relationships between the 12 key arguments in the ongoing and increasingly important debate as to whether patients who have caused their own illness should receive lower priority in access to healthcare resources compared with those who have not. It has also revealed that the debate has stalled and remains unresolved. We suggest progression could be achieved by inviting multidisciplinary input from a range of stakeholders for the development of evidence-based critical evaluations of existing arguments and the development of novel arguments, including the outstanding rebuttals.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; not externally peer reviewed.
Linked Articles
- The concise argument
Other content recommended for you
- Personal responsibility within health policy: unethical and ineffective
- Moral responsibility for (un)healthy behaviour
- Prevention in the age of personal responsibility: epigenetic risk-predictive screening for female cancers as a case study
- Coronary artery bypass graft surgery: socioeconomic inequalities in access and in 30 day mortality. A population-based study in Rome, Italy
- Alcoholic and non-alcoholic fatty liver disease and associations with coronary artery calcification: evidence from the Kangbuk Samsung Health Study
- Phase-dependent justification: the role of personal responsibility in fair healthcare
- Preoperative factors affecting cost and length of stay for isolated off-pump coronary artery bypass grafting: hierarchical linear model analysis
- Responsibility in health care: a liberal egalitarian approach
- Unhealthy behaviours and disability in older adults: Three-City Dijon cohort study
- One-year costs of bilateral or single internal mammary grafts in the Arterial Revascularisation Trial