Article Text

Abstract
Clinical ethics has been developing in paediatric healthcare for several decades. However, information about how paediatricians use clinical ethics case consultation services is extremely limited. In this project, we analysed a large set of case records from the clinical ethics service of one paediatric hospital in Australia. We applied a paediatric-specific typology to the case referrals, based on the triadic doctor–patient–parent relationship. We reviewed the 184 cases referred to the service in the period 2005–2014, noting features including the type of case, the referring department(s) and the patient's age at referral. The two most common types of referral involved clinician uncertainty about the appropriate care pathway for the child (26% of total referrals) and situations where the child's parents disagreed with the doctors’ recommendations for the child's care (22% of total referrals). Referrals came from 28 different departments. Cancer, cardiology/cardiac surgery and general medicine referred the highest numbers of cases. The most common patient age groups were children under 1, and 14–15 years old. For three controversial areas of paediatric healthcare, clinicians had initiated processes of routine review of cases by the clinical ethics service. These insights into the way in which one very active paediatric clinical ethics service is used further our understanding of the work of paediatric clinical ethics, particularly the kinds of ethically challenging cases that paediatricians view as appropriate to refer for clinical ethics support.
- Paediatrics
- Clinical Ethics
- Ethics Committees/Consultation
Statistics from Altmetric.com
Introduction
Clinical ethics case consultation began emerging as a feature of paediatric healthcare in the mid-1970s.1 ,2 Since that time, the availability of clinical ethics support has become increasingly widespread and is now established in various forms in many paediatric hospitals in North America, Europe and elsewhere.3 ,4 However, there are few studies of paediatric clinical ethics case consultations. Some sets of paediatric cases are reported within larger studies from hospitals that treat both adults and children5 and there are some older studies from paediatric hospitals.6–8 Recently, several paediatric-specific studies have also been published, primarily from the US context.9–14 Three themes that emerge from existing studies are the large proportion of case referrals for children less than a year old,7–9 ,13 ,14 the diversity of case typologies used,9 ,10 ,15 ,16 and the way in which the case sets vary depending on the nature and focus of the hospital.10 ,17
In this paper, we aim to contribute to this body of knowledge by reporting on the 184 clinical ethics case referrals that occurred at the Royal Children's Hospital in Melbourne, Australia, over a 10-year period. Our project addressed the following research question: What kinds of cases do paediatricians refer for clinical ethics case consultation? Insights into the way in which one paediatric clinical ethics service is used can further our understanding of the work of paediatric clinical ethics, particularly the kinds of ethically challenging cases that paediatricians view as appropriate to refer for clinical ethics support.
The clinical ethics service at the ROYAL CHILDREN'S HOSPITAL
The Royal Children's Hospital (RCH) has approximately 330 beds and is the major tertiary paediatric hospital in the Australian state of Victoria. The hospital provides a full range of clinical services to children and young people.18 It includes a neonatal intensive care unit (NICU), a paediatric intensive care unit, a mental health unit and an emergency department.15
The RCH clinical ethics service was established in 2005. Its genesis and structure have been described in detail elsewhere.19 ,20 It currently receives salary support for four part-time ethics staff (equivalent to a total of 1.1 full-time staff) and one part-time (0.6) administrator. Any hospital staff member can refer a case for clinical ethics consultation. However, as has been reported at some other paediatric centres8 ,10 almost all referrals come from senior paediatricians.
Case consultations are usually conducted by the Clinical Ethics Response Group (CERG). The CERG is a multidisciplinary group with a total membership of approximately 40 RCH staff members. Depending on availability, approximately 6–8 CERG members are present at each meeting. CERG meetings can be convened promptly (within approximately 24–48 h) after a referral is made. The CERG includes ethicists with a philosophy background. It also includes a range of healthcare professionals, some with formal academic training in ethics. CERG members come from clinical backgrounds including medicine, nursing, psychology and speech pathology, as well as pastoral care staff. Each CERG case consultation involves at least one ethicist and multiple clinicians from the CERG; no specific composition of CERG members is mandated.
The CERG uses a collaborative approach to clinical ethics case consultation. Members of the treating team are directly involved in the process of ethical deliberation.20 ,21 This approach links closely to the idea of ‘naturalized clinical ethics’ described and advocated by Verkerk and Lindemann.22 Patients and/or parents are not usually present at CERG meetings and, in some cases, may not be aware that their case was discussed. While the involvement of patients and/or parents is a key element of case consultation in many settings, this centre's ethics service was initiated by clinicians with the specific aim of facilitating good ethical decision making by clinicians through structured peer support. The CERG functions to support the treating team in exploring the options and their ethical implications, rather than to mediate between parties or to make binding decisions. As such, contact between the ethics service and the family is not standard, and is instead considered on a case-by-case basis by the ethics service together with the treating clinicians.
Approximately 70% of case referrals proceed to case consultation performed by the CERG. However, other modes of case consultation are available and the clinical ethics service is guided by the referring clinician's preference; a referral would not proceed to case consultation by the CERG without the agreement of the referring clinician. Some cases are discussed informally with one or more of the clinical ethics staff. Some cases are discussed retrospectively at departmental education sessions. Sometimes referrals do not proceed to a case consultation when the clinical situation changes; for example, when parents consent to a medically recommended treatment that they had previously refused, or the child becomes medically unsuitable to undergo a treatment that the treating team was uncertain about whether to offer. The present analysis included all case referrals.
For three separate areas of paediatric healthcare, doctors have approached the clinical ethics service seeking ethics input as a routine element of care when offering particular treatments. The three treatments are surgery aimed at fertility preservation (primarily for children with cancer), surgery to alter the genitals and/or remove the gonads of children with disordersi of sex development (DSD) and the administration of puberty blockers or cross-sex hormones to treat gender dysphoria. For each area, doctors were aware that there was a diversity of practice among clinicians and centres in relation to offering these treatments, and that these treatments had also attracted controversy in the wider community. Routine referrals came from:
cancer, gynaecology and immunology for fertility preservation cases;
endocrinology, gynaecology and general surgery for DSD cases;
endocrinology, adolescent health and mental health for gender dysphoria cases.
This analysis included routine referrals, but focuses primarily on non-routine referrals. Routine referrals will be discussed in greater detail in a future paper.
Method
Since its first clinical ethicist was appointed in May 2005, the clinical ethics service at RCH has kept electronic records of all case referrals received. The data for this study were extracted from these records. For each case referral, we noted the following features into a new table:
year of referral;
referring department(s);
patient's age at referral;
patient's medical condition;
whether the case referral was a repeat referral for a patient who had already had a case referred to clinical ethics;
whether the case referral related to more than one patient (eg, twins);
synopsis of the case;
the key ethical question(s) raised by the referred case as identified by the referring clinician and/or the lead clinical ethicist.
For cases that were referred by multiple departments, we counted each department as a referring department. For example, we counted a case that was jointly referred by the adolescent health and cancer departments as one case referral by adolescent health, and one case referral by cancer.
Using the information in the ‘case synopsis’ and ‘key ethical questions’ fields, we then independently allocated each case to a single category. We used the typology described below (plus the three types of routine referrals). Our categorisation aligned for 165 (90%) of the 184 case referrals. For the 19 cases where we disagreed, we discussed each case referral until we reached agreement about the most appropriate category.
The protocol was approved by the Human Research Ethics Committee of the RCH (HREC: 33142B).
Typology
The appropriate way to classify paediatric clinical ethics cases is a contested issue in the existing literature.9 ,16 In the absence of a standardised typology for paediatric clinical ethics cases, our analysis used a paediatric-specific working typology for ethics consultations. This typology is based on the doctor–patient–parent triad and focuses attention on the moral agents involved in the situation. We have described this typology and its rationale in detail elsewhere.15 The categories are conceptualised as a working typology, which evolves as new cases are referred and sets of cases are analysed. As such, the current list of five broad categories differs in some respects from the list described previously. For example, refinements during this project included changing the type ‘Parents disagree with one another about treatment options’ to refer instead to ‘family members’, as there was a case referral where a parent and a grandparent disagreed. We also combined two types into one. The two original types were ‘Clinician is uncertain about the appropriateness of offering a particular treatment’ and ‘Clinicians and parents are both uncertain about the best way to proceed when a variety of options are available’. The two types were insufficiently distinct in this group of case records, and so became the single type ‘Treating team uncertain about the appropriate care pathway’.
Thus, the typology currently consists of five broad categories of ethical challenge:
Treating team uncertain about the appropriate care pathway
Parents disagree with treating team's recommendations
Family members disagree with one another about treatment options
Adolescent/potential mature minor disagrees with treating team's recommendations
Child is resisting treatment
A brief example of each type of case is given in table 1 to illustrate the categories. These examples represent real case referrals but with identifying details altered for confidentiality.
Examples of case types
Results
Number and types of referrals
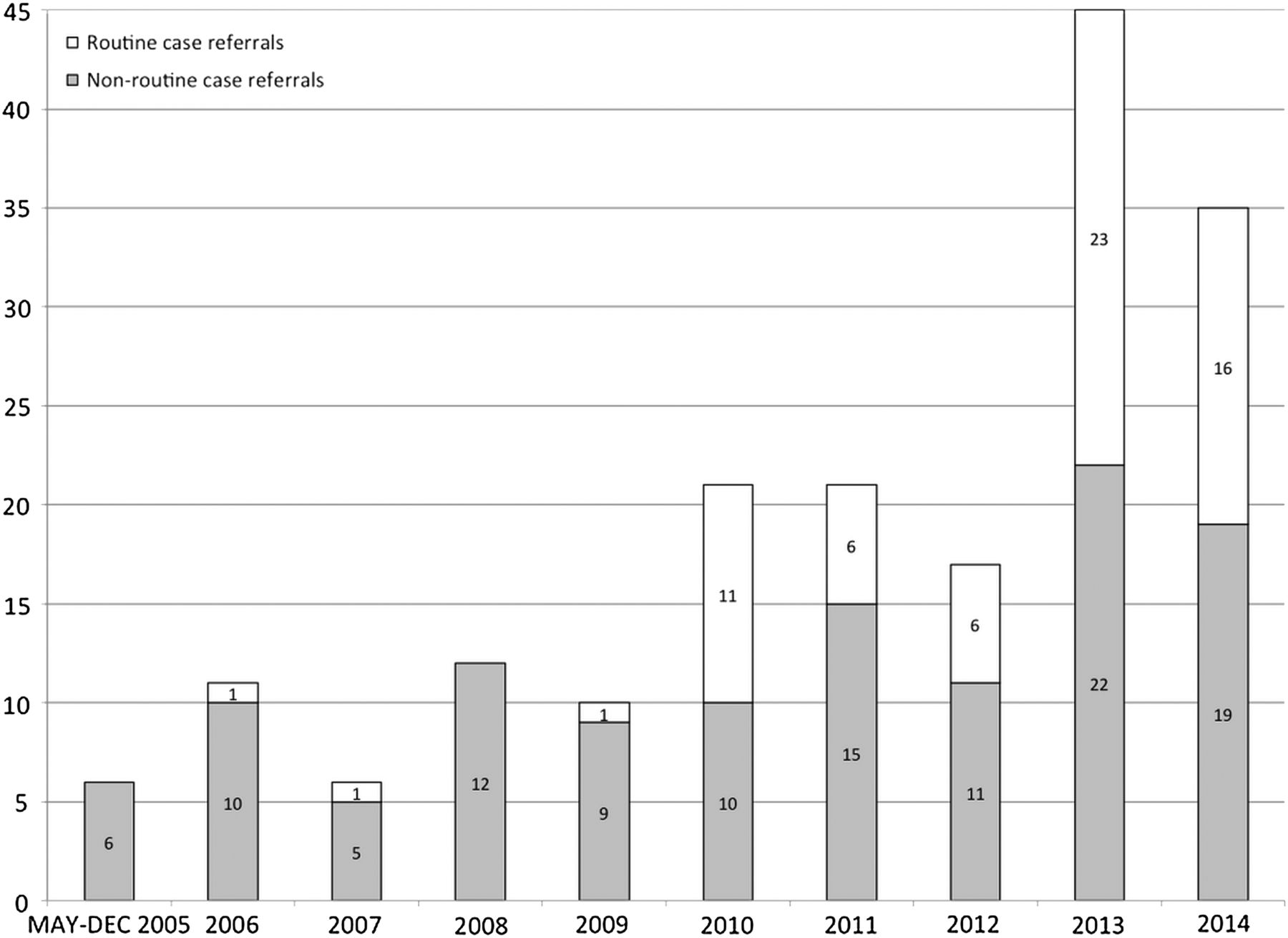
There were 184 case referrals in total in the period under review (May 2005–December 2014). There were 176 different patients associated with clinical ethics case referrals. The number of referrals is presented year by year in figure 1. The number of referrals varied each year, with a general trend of increase. The sharp increase between 2012 and 2013 is partly attributable to the introduction of routine referral for fertility preservation surgery. Excluding 2005 (as it was less than a complete year), the mean number of referrals per year was 20. The mean number of non-routine referrals per year was 13. The types of referrals are detailed further in table 2.
Types of case referrals at the RCH

Number of ethics case referrals per year.
Patient ages
A summary of patient ages is presented in figure 2. Infants less than a year old were the most common age group, followed by 15-year-olds and 14-year-olds. Two referrals involved fetal patients. Age data was not analysed for routine referrals, as these generally relate to patient populations of specific ages (eg, infants for DSD surgery cases).

{kind=link}
{kind=link}
Patient ages.
Nine patients had multiple referrals: eight patients were the subjects of two clinical ethics case referrals in the same year, and one patient was the subject of four clinical ethics case referrals across four different years. Three referrals each involved two children in the same family.
Referring departments
Outside the routine referral processes, most referrals came from a single department (112/119). Of the remaining seven, six were jointly referred by two departments and one was jointly referred by four departments. An overview of the different departments that referred cases for clinical ethics consultation and the number of referrals by each department is presented in table 3. In the case consultations themselves, multiple departments are almost always involved. A very wide range of medical conditions was represented in the referrals, reflecting the breadth of conditions treated at this hospital.
Referring departments for the non-routine case referrals
Discussion
The RCH clinical ethics service received a mean of 20 referrals per year (or, excluding routine referrals, 13 per year), with a trend of increasing numbers. This is high in the context of published data on referral volume at other centres. For example, a recent survey of ethics consultation volume at 44 US children's hospitals found a median number of eight consultations per year (with a range of 1–57).25 Similarly, when Kesselheim and colleagues surveyed 33 US paediatric clinical ethicists, 46% reported that their services conducted 6–10 formal ethics consultations in the previous 12 months and a further 24% reported a figure of 1–5 consultations.3 However, the high volume of referrals at RCH is similar to the volume reported in a 5-year study at Zurich University Children's Hospital.13 In addition to receiving a high volume of referrals relative to many other centres, the RCH clinical ethics service experienced a trend of increasing numbers of consultations over time. This is not a universal feature of paediatric clinical ethics services. For example, Johnson and colleagues, in their review of cases at St Jude Children's Research Hospital in the period 2000–2011, report that ‘[t]he annual number of consults varied and did not increase over time’.10
There are various possible reasons for the relatively high and increasing volume of case referrals at this centre, beyond the size of the hospital. There is financial support for the operation of the clinical ethics service and the clinical ethics staff consists of experienced clinicians and PhD-qualified ethicists.3 ,26 The service has been formally recognised by peers as being of high quality (winning the Hans Joachim Schwager award for excellence in clinical ethics, at the 9th International Conference on Clinical Ethics Consultation). The high volume could also reflect the history of the service, which was clinician-initiated and has deliberately focused on a ‘ground-up’ approach in all of its activities. The clinical ethics staff run various education sessions throughout the hospital, including a 3-day conference held annually since 2009 which is well attended by hospital staff. The clinical ethics staff also undertake departmental visits. These activities have presumably increased awareness of the service since its inception, which may partly account for the increasing number of referrals.
Reflecting on the types of cases that have been referred by paediatricians to clinical ethics, it is interesting to note that a quarter of the total case referrals were situations in which the treating team were uncertain about the appropriate care pathway for the child. The conflict resolution function of clinical ethics case consultation is often emphasised. Delany and Hall, for example, describe clinical ethics committees as ‘aim[ing] to resolve conflict, facilitate communication and ease moral distress’.21 However, this set of cases highlights an additional important role that paediatricians see for clinical ethics, at least in this setting: as a forum for thinking through a problem. These paediatricians seem to be using the clinical ethics case consultation process in part to help form a view, rather than only to mediate conflicting views. This aligns with the position put forward by the American Academy of Pediatrics, that clinical ethics case consultation can be an appropriate source of support ‘when uncertainty or conflict exists’.27
Our analysis of patient age at referral showed a cluster of case referrals for infants less than a year old and another cluster of case referrals for adolescents aged 14 and 15 years. Approximately a quarter of referrals related to patients aged less than 1 year (setting aside routine review processes). Despite being the most common age for patients referred to clinical ethics at RCH, this age group constituted a smaller proportion of patients in this study compared with other studies that identify children under a year old in their demographic data.7–9 ,13 This may reflect the fact that babies born prematurely are usually cared for in the nearby women's hospital, coming to RCH only for surgery. The issues around life-sustaining interventions for these patients are therefore primarily encountered at the women's hospital rather than at RCH.24 Previous studies do not report patient age data in a way that enables identification of patients aged 14–15 years. Given the well-recognised ethical complexity of adolescents' emerging autonomy, it is perhaps not surprising that paediatricians sought clinical ethics support relatively frequently in caring for this age group.
The most common referring departments were cancer, general medicine, cardiology/cardiac surgery and NICU (setting aside the three routine referral processes). These align with the most common primary medical teams in a recent review of another large set of paediatric ethics cases from the US.14 Although the order and proportions are different in the two studies, the prominence of these departments may suggest that they are ethical hotspots in paediatric hospital care or perhaps that clinicians trained in these specialties are particularly alert to ethical complexity and the availability of clinical ethics support. In a Swiss study of 95 cases, ICU and rehabilitation were the most prominent departments.13 Other large case sets are from a hospital primarily treating oncology patients10 or report in terms of ‘primary diagnosis’9 or ‘place of consult’11 rather than referring department.
There are some important limitations to this study. First, the data are from only one site and so cannot be generalised. However, this set of case referrals contributes to the small but growing body of literature on paediatric clinical ethics cases from various centres around the world. The different typologies used by different authors make it difficult to compare and potentially aggregate data across centres. A standardised typology for paediatric clinical ethics cases would facilitate this. However, it may be the case that different typologies suit different contexts and purposes, and that continued diversity is both inevitable and useful. A further limitation of this study was that the ‘case synopsis’ and ‘key ethical questions’ data were only used for categorising the referral. We did not analyse the complex details of the cases, nor ourselves put forward an interpretation of the situation or the ethical issues involved. Our aim in this study was to present an overview of this large dataset but there is clearly scope for more in-depth qualitative analysis of this data. Another limitation is the lack of data on the impact of the referral on the child's care. As Kilham and colleagues have recently highlighted, measuring a comprehensive range of outcomes following clinical ethics case consultation is important.28 Gathering follow-up data is now part of the clinical ethics consultation process at RCH but such information was not available for the case referrals analysed here.
Conclusion
In this hospital, paediatricians from a wide range of specialities referred cases to clinical ethics. Clinical ethics support was sought in relation to paediatric patients of all ages, but particularly for children under 1 and for adolescents. Cases were sometimes referred because of an impasse between conflicting views, and sometimes because clinicians wanted assistance in forming a view. Clinical ethics was also used by some groups of paediatricians as a way of embedding ethical review into some patient care pathways that were known to be controversial.
This analysis only captured ethically challenging situations that paediatricians referred to the clinical ethics service. There may be many other ethically challenging situations encountered by this group of clinicians. Ethically challenging situations may be dealt with in other ways (such as peer discussion) or may not be perceived as ethically difficult. It would be useful to more directly investigate paediatricians' perceptions of the role of clinical ethics case consultation and their experiences of it, at RCH and elsewhere. It would also be useful to know much more about how clinical ethics services form recommendations, and how these recommendations influence clinicians' practice, families' experiences and the quality of children's healthcare.
References
Footnotes
Contributors RM designed the study. RM and LN analysed the data and drafted the manuscript.
Funding Australian Research Council Discovery Early Career Researcher Award (DE120100488).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
↵i We use the term ‘disorders of sex development’ in this paper, as this is the term used by the hospital. However, we acknowledge that some authors and groups prefer to use the more neutral term ‘differences of sex development’ instead.23
Other content recommended for you
- Paediatric clinical ethics in Australia and New Zealand: a survey
- Development of clinical ethics services in the UK: a national survey
- Clinical ethicists’ perspectives on organisational ethics in healthcare organisations
- Ethics of fertility preservation for prepubertal children: should clinicians offer procedures where efficacy is largely unproven?
- Project Examining Effectiveness in Clinical Ethics (PEECE): phase 1—descriptive analysis of nine clinical ethics services
- Clinical bioethics integration, sustainability, and accountability: the Hub and Spokes Strategy
- Sources of bias in clinical ethics case deliberation
- The need for a clinical ethics service and its goals in a community healthcare service centre: a survey
- Objectives and outcomes of clinical ethics services: a Delphi study
- Taking the burden off: a study of the quality of ethics consultation in the time of COVID-19