Article Text

Abstract
This paper explores whether donor-parents felt coerced to donate a kidney to their child. There is a paucity of UK literature on parental live kidney donors and the voluntariness of their decision-making. Data were gathered as part of a study exploring parental experiences of consenting for live donation at a UK specialist children's hospital. Parents who donated a kidney to their child between September 2006 and December 2010 and who consented at their child's hospital to be referred to an adult unit for consideration for live donation were invited to participate. Of the 19 eligible parents, seven fathers and three mothers consented to be interviewed. Their primary motivation for donation was being a parent (more specifically, the parent of a sick child). Participants expressed this in terms of parental love and concern. Participants conveyed certainty about their decision and viewed live donation as a positive opportunity. Most participants regarded the decision to donate, or not donate, as one every parent is entitled to make for their own reasons. In discussing our findings, we argue that when parents do not separate their child's interests from their own, this does not necessarily compromise autonomous decision-making: using one's own moral values to constrain one's own choices can be compatible with voluntary decision-making. Indeed, choices may be more constrained when parents are unable to donate, because this reduces the options available to parents to help their child.
- Transplantation
- Donation/Procurement of Organs/Tissues
- Family
- Coercion
- Autonomy
Statistics from Altmetric.com
Introduction
During the financial year 2010–2011, 134 paediatric kidney transplants took place in the UK.1 Of these, 65 were live donor transplants. Whilst this study took place in this year, the most recent figures are similar with 124 paediatric kidney transplants taking place between 2013 and 2014, 64 of which were live donor transplants.2 In the majority of cases, the recipient was known to the donor, typically the child's parent.1 ,2 Health professionals aim to present the options of deceased and live donation to parents without favouring live donation.3 It has been argued that parents are expected to agree to live donation in fulfilment of their parental responsibility.4 Some studies report that parents felt so obligated to donate that this contributed to, or resulted in, parents seeing live donation as their ‘only option’.5–7 Such findings are often incidental and not fully explored, but they suggest coercive pressure on parents to donate,6 ,8 raising concerns that their decision to donate is not a truly voluntary one.9 Biller-Andorno10 highlights the complexities of voluntariness in live donation, and makes reference to the concept of ‘pressured consent’ proposed by Fujita et al,11 which is described as encompassing internal pressure to donate as well as pressure applied externally. Whether internal pressure can constitute coercion is debateable,12 ,13 and there is no consensus about whether a parent can make a voluntary decision to donate.8 ,9 ,14 Recent studies suggesting reduced quality of life in parent-donors heighten these concerns and warrant further consideration of the consent process.15 ,16
This paper reports original data on whether parents perceived themselves to have a genuine choice about being a donor for their child, collected in a qualitative study exploring parental experiences of consenting for referral for live donation. The main research questions were: What influences/pressures did parents experience when faced with the decision of whether their child had a living or deceased donation? Did parents feel an obligation to donate?
Methods
Population and sample
Participants were recruited from a UK specialist children's hospital and were parents who donated a kidney to their child between September 2006 and December 2010. In all cases, initial discussions about transplantation and the various options available were conducted by a paediatric team consisting of the consultant, paediatric transplant nursing sister and play therapist. Further counselling, information, consent and workup (medical and psychological) for live donation took place at a different specialist centre to avoid any undue influence (real or perceived) from the paediatric team. To minimise recall bias, the time between post-transplantation and participation did not exceed 4 years. At least 3 months between transplantation and interview allowed any immediate surgical complications to settle. The inclusion criteria were: any parent donating a kidney to their child between September 2006 and December 2010, consented at their child's hospital for referral for live donation, and whose child had an outpatient appointment during the study period. There were 19 eligible participants (six mothers and 13 fathers) from a population of 71 children transplanted at the regional hospital with living or cadaveric organs during the time period. Where individuals did not meet inclusion criteria, this was due to their child not having an outpatient appointment in the timeframe.
The study received a favourable review from South Birmingham Research Ethics Committee and was approved by the trust's research and development department. Parents were invited to participate by a letter from their child's consultant.
Data collection
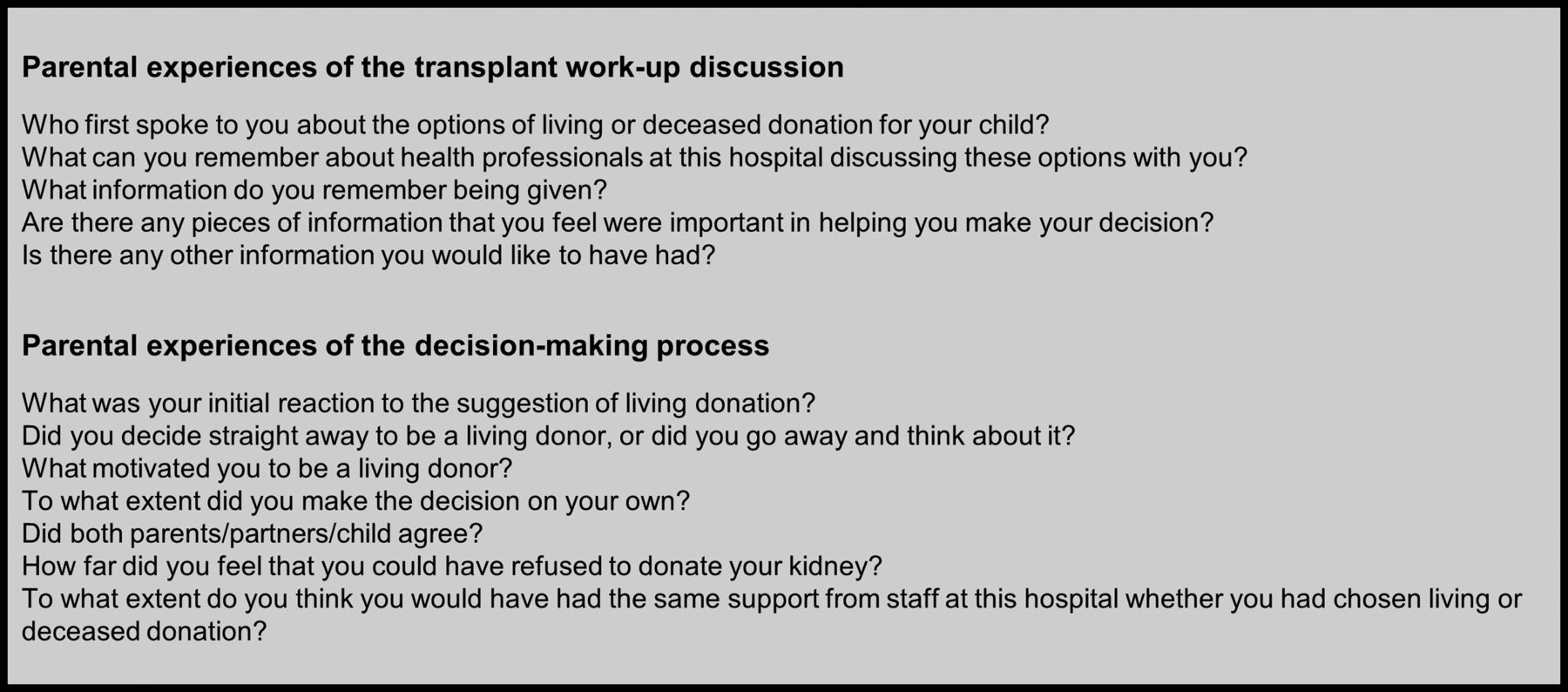
Individual interviews were conducted by PB in a private clinic room at the hospital. The interviews took place while participants waited for their child's routine outpatient test results. Face-to-face, semistructured interviews provided the opportunity for participants to convey their perceptions and allowed the interviewer to explore responses.17 A topic guide provided prompts for key areas (figure 1).

Interview topic guide (extract relevant to data reported in this study).
Questions aimed to be ‘open-ended, neutral, singular and clear’.18 Interviews lasted 52 minutes on average and were recorded, transcribed verbatim and anonymised with pseudonyms allocated. Consent was gained and formally recorded immediately before interviews commenced.
One participant required an interpreter. To maximise data reliability, the interpreter was made aware of the need to interpret as fully as possible. A second interpreter confirmed transcript accuracy.
Data analysis
Qualitative analysis largely followed conventional content analysis, allowing categories to emerge directly from data.19 Data gathering and analysis occurred simultaneously; consequently, analysis shaped subsequent interviews (e.g. probing for disconfirming data).
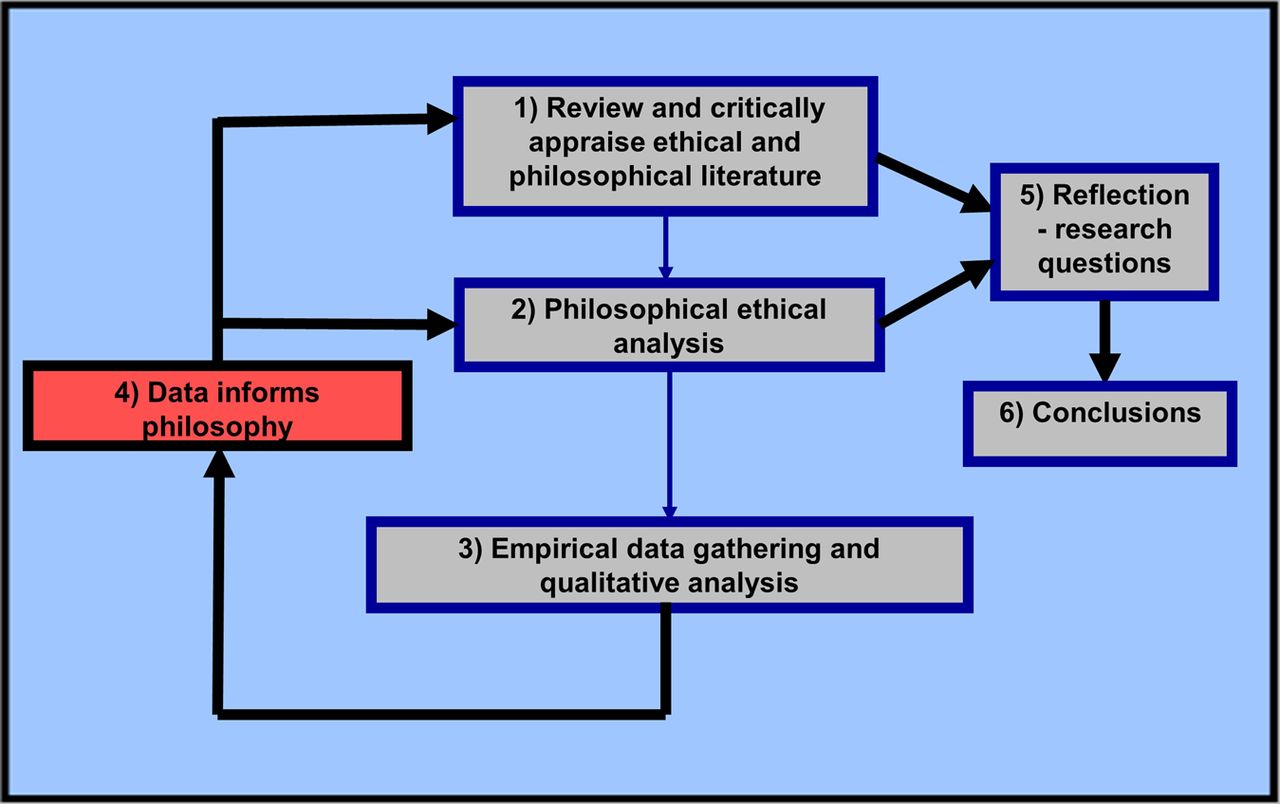
The empirical bioethics approach facilitated a realistic consideration of the ethical issues and analysed empirical data were integrated with ethical analysis.20 A priori philosophical arguments were reconsidered in light of themes that emerged from empirical data. Figure 2 summarises the approach.
{kind=link}
{kind=link}
The empirical bioethics approach used in the study.
Results
Of the data analysed, only (1) parental motivations, (2) perceptions of donation as a parent's decision and (3) donation as an opportunity are presented here. All names used in the reporting are pseudonyms to protect participant identity.
Participant characteristics
Of the 19 potential participants invited (all with successful functioning transplants), 10 consented to be interviewed. Nine were White British and one Asian. Five donations were father-to-son, two were father-to-daughter, one was mother-to-son and two were mother-to-daughter. Half were interviewed within 12 months of transplant; the time elapsed for the others ranged from 15 months to 4 years. Parental age ranged from 24 to 54 years with a mean age of 40 years. The age of the recipient-child at the time of transplant ranged from 4 to 16 years, with a mean age of 8 years.
Motivations for donation
Being a parent
All participants reported ‘just being a parent’ as their over-riding motivation: live donation was a way to help their child. This motivation was usually expressed in terms of parental love/concern, rather than obligation:
As parents there's nothing more dear to my heart than my little boy and girl….It was always going to be yes [to live donation]. (Ben)
Some participants referred to ‘parental nature’. Such statements could be interpreted as reflecting societal expectations, but this would be mistaken. Participants felt that their parental desire to help their sick child was ‘natural’, innate not socially constructed, and was not tied specifically to the donation. Participants felt that parents love their child and therefore want to help them out of danger. Their own behaviour, then, accorded with their view of the nature of being a parent; their decision was communicated in terms of acting on their own desires, and participant responses did not appear to convey a sense of pressure to donate:
I think it's just a natural thing for a parent to want to help their child; if you can, then that's what you have this desire to do. (Susan)
The majority of participants reported that both parents had been willing to donate, and for this reason deciding who would ultimately donate had proved difficult.
No participants reported having previously considered altruistic donation to a stranger nor wanting to be a live donor outside the context of donation to their child.
Being a parent of a sick child
Participants generally tied their motivation as a parent to being a parent of a sick child. Illness was unpleasant for the child and for the parent witnessing their child suffering.
You see your kids smile, it puts a smile on your face…you see your kids cry, you cry with them. (Liam)
Typically, parents wanted normality in their child's life:
All the things she wanted you couldn't give her. “I'm doing this [donating] so she can eat, drink, go to school.” (Lisa)
As a parent, you want to make your child's life whole again. (Elizabeth)
A parent's decision
Generally, participants considered parents in their situation to have a choice and equated ‘choice’ with lack of coercion in the sense of external force or threats to the donor-parent by another individual.21 They described their own situation as one where they felt they had a choice and made their own decision:
We weren't forced down that route at all. It was completely our choice as to what we wanted to do…In my own mind, if I had the opportunity to donate and get him back to good health, that was what we were going to do…It was totally my choice, but to be honest, the thought never came into my mind that I wasn't going to do it. (John)
Two participants did, however, refer to having ‘no choice’. Significantly, it was clear on elaboration that the sense in which they had no choice was that they had eliminated the alternatives themselves. The phrase ‘no choice’ conveyed their strength of feeling in a situation where they felt live donation was the only viable option for them, and that there was never any question in their own mind about the donating:
Interviewer: You said that you and your partner felt you had no choice. Could you tell me more about that?
Ben: We knew what our answer was from the start…If Sam didn't have the kidney transplant he would need dialysis, and we'd be waiting for a kidney off the transplant list. I don't think personally that's the way we could have gone, because I didn't want to see Sam on dialysis if we'd got another option.
My heart wouldn't accept my daughter losing her life, so I decided all we can do is try….I did not have any choice left, I did it for my child….I had the option of saying, even before the last second, I don't want to donate. Lots of thought and consideration goes into making the decision. And I wanted to do it for my daughter. (Farooq)
The majority of participants made reference to choice: they felt that they were making a decision where not donating was a genuine alternative, just not one they personally could countenance. They recognised that donation ‘wasn't right for everyone’, giving as examples: competing interests of other children; not wanting to donate; and being constrained by the need to work. Generally, participants said they did not have a negative impression of parents who decided, for whatever reason, not to donate, because every individual is entitled to their decision:
There's no right or wrong…everybody's got their own choice to make and whichever they decide is entirely up to them. (Susan)
Only two parents expressed disapproval of non-donating parents, notably Gregory:
Interviewer: If a parent said they didn't want to donate, what do you think your reaction would be?
Gregory: I'd be mortified. I'd say ‘why would you do that?’ It's like torturing your own child…If you could help them and you haven't done it, I wouldn't agree with them at all.
Donation as an opportunity
All participants expressed confidence about their decision to donate, and in striking contrast to concerns in the literature, regarded donation as an ‘opportunity’ to be embraced:
It's just, no contest, not a second thought…Never once did I feel unconfident about myself or what I was doing.’ (Liam)
From all the results of the tests it only took one little thing not to be right and that option would be taken away. We hoped all along that that was going to be the route we were going to take….I've got the option to do something for him, and I wanted to do it. (John)
Participants generally viewed donation in a positive light. When they described the first discussion with health professionals about live donation, this was not reported as a situation where they felt pressure to donate. Instead, parents wanted to donate. As one father succinctly put it, parents were given the ‘choice’ but also the ‘chance’ to help their child. Parents were typically pleased that live donation was a possibility:
I never resented being put in that position; it was a brilliant way forward…We were thankful that it was brought to our attention…We were more than happy to do it, and pleased to be able to. (Christopher)
Commonly, participants felt ‘lucky’ when they discovered they could donate and the only circumstance in which they envisaged themselves not donating was if they were tissue incompatible. Some parents described the upset this would have caused for them. Indeed, it was being incompatible that one participant described as being a situation of ‘no choice’:
Both me and my husband could [donate]. I think we're very fortunate; a lot of people aren't in that situation and they have no choice. (Susan)
Similarly Gregory referred to being able to donate as most important for a parent:
I'm just so happy I could have done it for him…As long as your kidney works, that's the main thing, then you can donate.
Having the opportunity to donate was reported as being accompanied by positive emotions such as relief, happiness and excitement immediately prior to transplant.
Brilliant! Hurry up! I was excited. I just wanted to do it. I wasn't nervous……Just get me in, get me out…get the kidney to her. (Lisa)
Limitations
These results are from one transplant centre, although our site covers a wide geographical area, serves a population of 6.5 million and is the only regional site where paediatric renal transplants are undertaken. All willing and eligible participants were interviewed. No new themes emerged in the last two interviews so it is likely data saturation was reached. Parents who decided against donation or were unable to donate were not included as we were interested in whether those who had donated felt at all coerced to do so. Although the sample was therefore arguably biased in favour of donation, it was not necessarily biased in terms of the participants’ experience of coercion. It is possible that those who experienced coercion declined to participate in the study (asking those who declined participation to provide a reason for this would have been beyond the remit of our ethical approval). It is also possible that those who did not donate had a different experience of the consent process. Most donors in the target population and 70% of participants were fathers (as a result of donor workup suitability or family preference). No post-transplant death or graft failure had occurred in either the study population or sample. This may have influenced positive recall of the consent process in the sample. Several of the participants and their recipient-children had, however, experienced postoperative complications (often requiring further surgery, for example the insertion of a percutaneous endoscopic gastrostomy in Gregory's child) and experiences were nonetheless recounted positively.
Discussion
Living donor-parents accept some degree of harm to benefit their child. The extent of the harm is relative to the different kinds of harmi they may experience if their child does not receive a transplant (and continues to suffer or dies).22 Dialysis reduces life expectancy; the probability of a child surviving 5 years on dialysis is 0.8, a mortality of about 1%.23 Parents may be particularly vulnerable to coercion where their children are concerned. When discussing our results, we make several assumptions that enable us to focus on the issue of choice and coercion. These are that the donation holds out a realistic prospect of success, the risks and harms for the donor seem greater than those that usually accompany surgical treatment where the patient is the direct beneficiary, the donor has received and absorbed the information necessary to decide whether or not to consent to donation, and finally that it is not inherently unethical for doctors to facilitate living donation (which we accept is a moot point).
The idea that parents have ‘no-choice-but-to-donate’ derives from the view that parents cannot make voluntary decisions about donation to their children because their parental values prevent them from choosing otherwise. Being a parent entails the curtailment of choices since parents are obliged to place the interests of their children ahead of their own interests. In this respect, parents are supposed to be different to other living donors, for whom the interests of self and others compete on a more level playing field. There are several problems with this line of thought.
First, it tends to equate the influence of internal pressure generated by deeply held values (e.g. about what it means to be a parent) with coercion.6 ,8 This would suggest that all morally motivated behaviour is coerced to the extent that it is based on a set of values and beliefs and precludes potential alternative courses of action. Moreover, the notion that an individual could coerce himself/herself strains the notion of coercion as something that undermines autonomous decision-making.
Zeiler et al argue that moral obligations do not compromise voluntariness provided these obligations are autonomously chosen. Accordingly, where a parent feels that ‘good parents’ should donate, but their internalisation of this moral imperative is not autonomous, voluntariness is compromised.14
Moreover, as Dworkin24 has argued, autonomy need not be considered as ‘substantive independence’. Taking on a commitment does limit one's options and may result in a ‘sense of restraint’ that is compatible with autonomy. So, provided parents have their own reasons for adopting the value that ‘good parents are willing to sacrifice some of their own interests to benefit their child's’, they make this value their own:
What is valuable about autonomy is that the commitments and promises a person makes be ones he views as his, as part of the person he wants to be, so that he defines himself via those commitments.24
Arguably, as long as parent-donors adopt values for their own reasons, they are capable of making a voluntary decision. The situation is analogous to a chess player following the rules of the game. The chess player is not coerced when he only moves the bishop diagonally, because he has chosen to follow this rule. For one's moral values to be one's own, one does not need to be the author of those values, one only needs to choose them.
Parents who feel they ought to donate do have a choice, but their own values determine how they use that choice. In this respect, a parent is no different to any other living donor who holds values that tell in favour of donation.
Healthcare professionals—especially those working with children—are both alert and sensitive to patients expressing values that do not appear to be their own. That said, it is difficult to see how an assessment of the extent to which an autonomous person has autonomously chosen the values in which they believe could be put into operation in practice. But this would call into question how receivers validate a consent—or refusal of consent—in a range of circumstances, and not just that of potential donor-parents.
The second problem with the view that parental choices are constrained may result from drawing an artificial distinction between the interests of the parent and the interests of their child. Frankfurt25 observes that when one person loves another, the lover wants to do that which is good for the beloved, because it is good for the beloved. Parental love may result in a fusion of the parent's and the child's interests such that the latter may seem to compel the former. This might give a false impression that one is not doing what one wants. Ross et al26 suggest this fusion of interests means that a parent does not wish to separate their child's interests from their own. Frankfurt25 concurs: a parent who loves their child ‘invests’ himself/herself in their child such that when the child's interests are harmed not only does the child suffer, but the parent suffers too.
This view was reflected by our participants who expressed their motivations in terms of parental love and concern rather than obligation. They reported donating because improving the well-being of their child was important for that child and therefore for themselves. For our participants, donation also served their own interests because they tended not to separate their child's interests from their own.
In this respect, it may be difficult to determine the extent to which parents form a special category of living donor. Many donors may be motivated to donate by love, and the more intense the love the more difficult it may be to disentangle the interests of self and other. For donors in this position, the choice may also be framed as being between two kinds of harm and risks to themselves: the harms (and potential risks) of donation or the harms of witnessing the suffering of the recipient and/or losing them completely to death.22
Biller-Andorno10 asserts that someone should be regarded as capable of autonomous decision-making where two conditions are met. First, the person must have the moral maturity to decide whether they wish to address their own needs (interpreted here as the needs of the parent) or the needs of others (interpreted here as the needs of the child). Our data illustrate the way in which these two sets of needs may be inextricably fused. Biller-Andorno's10 second condition is that the environment allows for expression of which needs the individual wishes to address. In the context of live donation, this translates into a parent feeling comfortable to communicate a decision not to donate as well as one to donate. While our participants typically thought most parents would want to donate because of parental love and concern, most (8/10) said they would respect the judgement of a parent who did not want to donate (as opposed to being unable to do so). This, assuming honest reporting, suggests they did not anticipate being adversely judged by others if they had decided against donation themselves. Indeed, our participants anticipated receiving the same treatment from hospital staff whether they donated or not.
Where two participants referred to having limited choices, the phrase ‘no choice’ was used to convey their strength of feeling in response to ‘probing’ questions (about their feelings of having a limited choice). They were not describing the absence of a viable alternative per se but rather that live donation was the only option for them.
No parent had previously considered living donation, but instead was responding to the seriousness of and suffering caused by their child's illness. Having a sick child was a definite motivator for donation, but being told about the possibility of donation or being found to be a compatible donor was definitely not experienced by our participants as a negative or coercive pressure. Qualitative findings are not generalisable and we need to be cautious about underestimating the risks of live donation. Nonetheless, health professionals approaching parents to discuss live donation may be somewhat reassured by our findings that live donation was perceived by our participants as a means of regaining control and having a positive opportunity to achieve their most desired aim, namely, to see their child well again.
Conclusions
Our data do not support the suggestion that a parents’ sense of obligation to donate compromises voluntariness by removing choice. Our participants described themselves wanting to donate out of love and concern for their child. They did not appear to regard themselves as being put under, or acting on, pressure to donate. Rather than foreclosing choice, being able to donate was regarded as increasing choice. In their view, ‘no choice’ better described the situation of parents who are found to be unable to donate to their children because such parents do not have the choice or opportunity to help their child.
The extent to which our results are generalisable across a range of different units and circumstances remains to be shown. Clearly, it is important for healthcare professionals to protect potential donor-parents from coercion in the form of external pressure to donate, and also to be open to the possibility that a potential donor-parent may feel obliged to donate but nevertheless be reluctant to do so. Our results do, however, suggest that potential parent-donors can make a voluntary decision to donate, and do not feel that they have no choice other than to donate. Indeed, not raising donation as a possibility will curtail rather than enhance choice.
Acknowledgments
We thank the staff at the research site for their assistance, in particular the paediatric transplant nursing sister. We thank the participants for sharing their experiences so generously.
References
Footnotes
-
Contributors PB participated in research design, data collection and data analysis. S-AH participated in research design and recruitment. HD was the lead supervisor and participated in research design and data analysis. PB wrote the first draft of the article, which was reviewed by HD and S-AH. All authors reviewed and approved the final version.
-
Funding This research was supported by the University of Birmingham's BMedSci Population Sciences and Humanities Programme.
-
Competing interests None.
-
Ethics approval South Birmingham Research Ethics Committee (REC), Redditch, UK. REC Reference Number 11/H1207/3.
-
Data sharing statement The data presented are available on request from the corresponding author.
-
Patient consent Study subjects were parent-donors rather than patients. A specific consent form was devised and approved by the REC. All participants gave informed consent prior to taking part.
-
Provenance and peer review Commissioned; internally peer reviewed.
-
↵i For a general discussion on the balance of harms and benefits of live donation see.22
Linked Articles
- Clinical ethics
- Clinical ethics
- Clinical ethics
Other content recommended for you
- Developing an ethics framework for living donor transplantation
- Who should provide the uterus? The ethics of live donor recruitment for uterus transplantation
- Changes in quality of life (QoL) and other patient-reported outcome measures (PROMs) in living-donor and deceased-donor kidney transplant recipients and those awaiting transplantation in the UK ATTOM programme: a longitudinal cohort questionnaire survey with additional qualitative interviews
- Live liver donation, ethics and practitioners: ‘I am between the two and if I do not feel comfortable about this situation, I cannot proceed’
- Unrelated living organ donation: ULTRA needs to go
- Allowing autonomous agents freedom
- Needs must: living donor liver transplantation from an HIV-positive mother to her HIV-negative child in Johannesburg, South Africa
- Join the Lone Kidney Club: incentivising live organ donation
- Renal transplantation
- Who is willing to take the risk? Assessing the readiness for living liver donation in the general German population