Article Text

In assisted dying, the end-of-life trajectory is shortened to relieve unbearable suffering. Unbearable suffering is defined broadly enough to include cognitive (early dementia), psychosocial or existential distress. It can include old-age afflictions that are neither life-threatening nor fatal in the “vulnerable elderly”. The voluntary refusal of food and fluids (VRFF) combined with continuous deep sedation (CDS) for assisted dying is legal. Scientific understanding of awareness of internal and external nociceptive stimuli under CDS is rudimentary. CDS may blunt the wakefulness component of human consciousness without eradicating internal affective awareness of thirst and hunger. Patients may suffer because of the slow dying process following dehydration and starvation. The difficulty to adequately control distress, without bringing the dying process to a rapid conclusion by lethal pharmacological interventions, can cause feelings of guilt among hospice and medical staff. Furthermore, the double-effect principle is not applicable in these situations because the primary objective of VRFF is to hasten death. Legal and societal debate should focus on sharpening the boundaries between assisted dying and palliative care. This separation is necessary to: 1) uphold trust in the patient-phyician relationship, and 2) preserve integrity and ethics of the medical profession.
- Physician-assisted dying
- palliation
- euthanasia
- end-of-life care
- suffering
- sedatives
- opioids
- dehydration
- starvation
- definition/determination of death
- care of the dying patient
- attitudes toward death
- autonomy
- ethics committees/consultation
- informed consent
- philosophical ethics
Statistics from Altmetric.com
- Physician-assisted dying
- palliation
- euthanasia
- end-of-life care
- suffering
- sedatives
- opioids
- dehydration
- starvation
- definition/determination of death
- care of the dying patient
- attitudes toward death
- autonomy
- ethics committees/consultation
- informed consent
- philosophical ethics
Introduction
There is a growing trend to practise physician-assisted dying (death) (PAD) under the premise of providing quality palliative care in consensual and non-consensual life-ending situations.1 The WHO envisages palliative care as a comprehensive system of managing pain and distressing symptoms without intending to shorten the end-of-life (EOL) trajectory.1 In assisted dying, the EOL trajectory is shortened to relieve suffering.1 Bundling PAD with palliative care is precarious because PAD: (1) contravenes the Hippocratic principle of ‘do not kill’; (2) transgresses cultural and religious values of some patients, families and healthcare professionals; and (3) violates basic human rights.2
Voluntary refusal of food and fluids (VRFF) is a legal method of PAD, although medical and societal acceptability is uncertain.3 Etkind reported a patient with amyotrophic lateral sclerosis who desired to end life because of mental anguish and fear of unbearable future suffering.4 The patient chose VRFF to hasten death after the onset of bulbar disease progression. In this paper we comment on: (1) unbearable suffering as an indication for PAD; (2) VRFF as a means to hasten death; (3) efficacy of continuous deep sedation (CDS) for optimal control of distress from VRFF; and (4) bundling assisted dying with palliative and hospice care.
Unbearable suffering
When deciding on the use of CDS, severity of suffering is difficult to quantify objectively.5 The interpretation of the adjectives ‘refractory’ and ‘unbearable’ is subjective. The Dutch Medical Society (KNMG) states that suffering must be lasting and unbearable to request euthanasia.6 Persons ineligible for euthanasia but desiring to die can opt for VRFF and CDS.6 Unbearable suffering is defined broadly enough to include cognitive (early dementia), psychosocial or existential distress.6 It may also include various ‘… old-age afflictions that are neither life-threatening nor fatal in the vulnerable elderly’ (p23)6 such as diminished vision, hearing, mobility, fitness or independence:
In the future, physicians will be confronted more than ever before with seniors in vulnerable positions, ever-more advanced in age and, moreover, keen to live independently for as long as possible (p22).6 Many older people have various afflictions that are not actually life-threatening but do make them vulnerable … [I]t is wholly justifiable that vulnerability—extending to such dimensions as loss of function, loneliness and loss of autonomy—should be part of the equation physicians use to assess requests for euthanasia (p22).6
VRFF and hastening of death
Although VRFF may be legal, it can also result in a slow dying process. Etkind's case report illustrated the challenges of achieving optimal control of suffering from VRFF.4 Nevertheless, VRFF is promoted as a legal and peaceful method of hastening death.7 The KNMG even endorses VRFF for patients who are ineligible for euthanasia and whose ‘… suffering is not unbearable and lasting within the meaning of the Euthanasia Law’ (p34).6 ‘(A) patient with a strong wish to die may decide for himself to deny food and drink. In that case, the patient is making a conscious choice to hasten death’ (p34).6 The KNMG obligates physicians to provide due care with CDS or intermittent deep sedation regardless of agreement with the patient's decision. ‘When a patient dies due to not eating and drinking this constitutes a natural death, even if the patient was under continuous sedation according to accepted treatment’ (p36).6 However, the premise that death under CDS is ‘natural’ has been refuted.8 Hastening death by VRFF and CDS may even inflict additional harm and suffering.9–11
Efficacy of CDS in VRFF
Etkind's VRFF scenario compounded the patient's distress by the additional burden of physical manifestations of acute metabolic derangement from dehydration including agitation and bulbar weakness.4 A vicious pathophysiological cycle was set in motion: worsening metabolic derangement from dehydration, uncontrollable agitation and escalating doses of sedatives (figure 1).3 It is a misconception that high doses of sedatives to obliterate consciousness always eradicate inner affective awareness of thirst and hunger. CDS may blunt the wakefulness component of human consciousness without abolishing internal awareness.10 ,11 However, absent wakefulness prevents interacting with the environment. Scientific understanding of awareness of internal and external nociceptive stimuli under CDS is rudimentary.11 Functional neuroimaging of the human brain in pharmacological and pathological states of coma heightens concerns that sedatives will not always abolish inner awareness of suffering.11 Commentators have expressed reservations about whether CDS is the ideal method of achieving the goal of a rapid painless death9–11 because the clinical efficacy of CDS remains unproven.
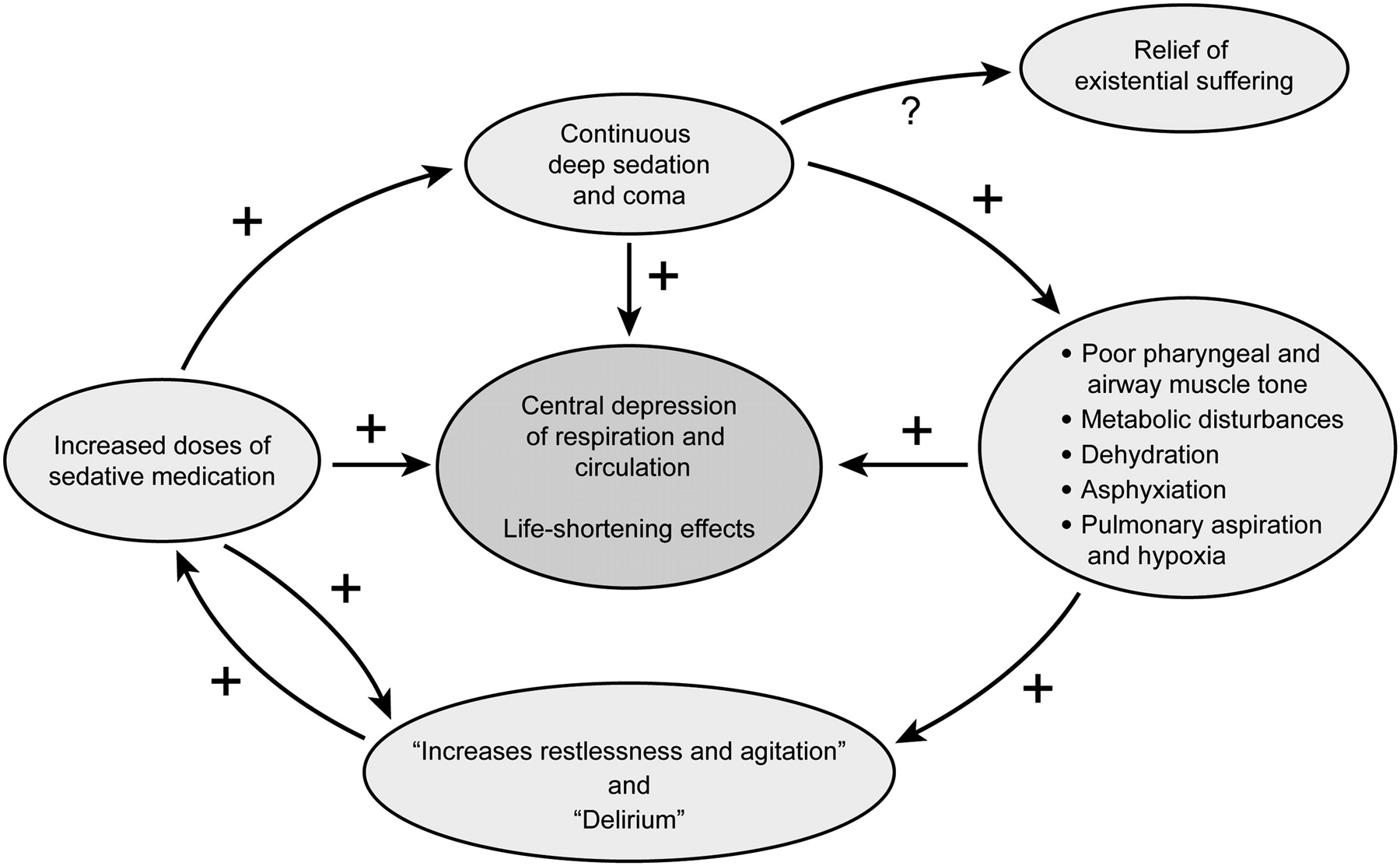
{kind=link}
Self-perpetuating cycle of life-shortening pathophysiological events triggered in continuous deep sedation. Reproduced from Rady and Verheijde.3 The publisher SAGE waived the need for permission to reuse (© SAGE).
Assisted dying and the double-effect principle
Moral and professional obligations demand delivering optimal and comprehensive palliative care to the terminally ill patient. However, confusing the terminally ill patient with the imminently dying patient does not constitute a justification for hastening death. To differentiate assisted death from natural death, we objectively defined the term ‘imminently dying’ by the onset of new lethal pathophysiology from acute life-threatening illness or fatal complications of the underlying disease.12 For instance, the onset of bronchopneumonia secondary to bulbar palsy would constitute natural death in Etkind's case. On the other hand, VRFF and CDS introduce new lethal pathophysiology intended to hasten death.3 The intent of VRFF (first act) is to consciously hasten death and the second act (use of sedatives) becomes a direct and predictable consequence of the first act. We have argued that administering sedatives and opioids in planned life-ending interventions based on the analysis of the double-effect principle—intention and causation of death—is not palliative care.1 ,3 The use of sedatives with VRFF is commensurate with euthanasia.
Assisted dying and hospice care
Deliberately hastening death by VRFF has unintended consequences. Patients suffer because of the slow dying process following dehydration and starvation. The difficulty of adequately controlling distress without bringing the dying process to a rapid conclusion by lethal pharmacological interventions can cause feelings of guilt among hospice and medical staff. We recommend that terminating life or assisted dying should not be conflated with palliative and hospice care. The Dutch KNMG arbitrarily defines VRFF with sedation to end life as ‘natural death’ and obligates physicians to participate in due care during this procedure.6 Owing to the absence of empirical evidence for the efficacy of CDS in managing distress, it may be argued that VRFF with sedation may represent a cruel and inhumane method of terminating life. Narratives of physicians who have engaged in CDS have suggested that there is a real need to separate the practice of assisted dying from the practice of medicine.13 Ultimately, the question that the medical profession and society must address is how to deal with patients requesting assistance with ending their lives. We urge that both the legal and societal debate should focus on sharpening the boundaries between assisted dying and palliative care. This separation is necessary (1) to uphold trust in the patient–physician relationship and (2) to preserve the integrity and ethics of the medical profession.
Conclusion
Although VRFF combined with CDS is a legal method of PAD for unbearable suffering, it can also result in a slow dying process. CDS may blunt the wakefulness component of human consciousness without eradicating inner affective awareness of thirst and hunger. Owing to the absence of empirical evidence on the efficacy of CDS in managing distress, it may be argued that VRFF with sedation represents a cruel and inhumane method of terminating life. Legal and societal debate should focus on sharpening the boundaries between assisted dying and palliative care.
Footnotes
Linked article 100213.
Correction notice This article has been corrected since it was published Online First. An earlier version was uploaded in error.
Competing interests None.
Provenance and peer review Commissioned; internally peer reviewed.
Linked Articles
Other content recommended for you
- Euthanasia and palliative sedation in Belgium
- Terminal sedation and the “imminence condition”
- Approaches to suffering at the end of life: the use of sedation in the USA and Netherlands
- Continuous deep sedation for patients nearing death in the Netherlands: descriptive study
- Continuous palliative sedation until death: practice after introduction of the Dutch national guideline
- A response to critics: weakening the ethical distinction between euthanasia, palliative opioid use and palliative sedation
- Palliative sedation determinants: systematic review and meta-analysis in palliative medicine
- Palliative sedation: not just normal medical practice. Ethical reflections on the Royal Dutch Medical Association's guideline on palliative sedation
- Ethics of crisis sedation: questions of performance and consent
- Expanded terminal sedation in end-of-life care