Article Text

Abstract
The recent report of the UK government's Organ Donation Taskforce is in favour of continuing with the current organ donation system rather than changing to an opt-out system where people are assumed to be willing to donate. How did it reach this decision and is it correct?
- Donation/procurement of organs/tissues
Statistics from Altmetric.com
Introduction
The government needs to increase organ donation in the UK to meet the increasing demand for organs. Scientific breakthroughs in transplant technology and the introduction of immunosuppressive drugs have revolutionised the potential benefit of organ transplantation. Furthermore, the demand for these sophisticated surgical procedures has increased significantly as the population ages, the incidence of predisposing diseases rises and the care of co-existing diseases improves. The number of patients on the waiting list for organs currently exceeds 9000, and has increased by 40% since 2001. Moreover, this figure is likely to radically underestimate the number who would benefit from transplantation, given that the shortage of organs dissuades doctors from recommending patients for transplants and as patients who become too ill to undergo surgery are taken off the list. Meanwhile, the number of heart-beating cadaveric donors, the most common source of deceased donation in the UK, has fallen by 13% since 2004; these are individuals who have suffered a catastrophic injury and are ventilated before death. The number of people on the Organ Donor Register (ODR) has doubled from 8 to 16 million between 2001 and 2009.i Thus there is a widening gap between the number of organs available and the number of patients awaiting organs for transplantation, with the inevitable tragic consequences.
Perhaps the most poignant reminder that the current system of organ donation is failing us is the number of those dying prematurely on the waiting list: now at approximately 1000 every year.1 3
One way to increase organ donation might be to change the system of donation. At the request of the government, the Organ Donation Taskforce (referred to here as the Taskforce) carried out two studies. The first focused on optimising the infrastructure and public awareness of organ donation,1 and the second on the potential impact of an opt-out system of donation.2 This second report, published in late 2008, concluded that policy changes should not happen ‘at the present time’.
In this article I outline the current and proposed systems and appraise the second Taskforce report, examining its ethical position and its assessment of empirical data under three headings: assessment of public opinion, analysis of faith and belief groups, and the impact of opt-out systems. I shall conclude that both the ethical position and the assessment of data are inadequate and the conclusion is wrong.
Current and proposed systems
The current system
Since the Human Tissue Act 2004 (which was enforced in 2006), the UK employs an ‘opt-in’ system. Theoretically, it requires those wishing to donate organs after death to join the ODR and/or carry an organ donor card, or to otherwise clearly express their wishes. In this way wishes regarding organ donation are made clear in life and can be respected in death. In reality this rarely happens. Thus families are often relied upon in the difficult time around the death to decide whether organ donation should take place. Indeed, over 80% of current donations are agreed to by the family without a background of official registration.i Meanwhile, the high family refusal rate in the UK, averaging 40% and approximately 45%i in situations where the potential donor has not registered on the ODR, is the major factor limiting the number of potential donors who go on to donate.2 Furthermore, a minority (10%) of families refuse despite the deceased having registered a wish to donate on the ODR. While the family's ‘power’ to refuse permission for organ donation has no legal basis, in practice their wishes are often given precedence over the autonomy of the donor. Despite the NHS declaring a doubling of the ODR between 2001–2009, currently only 28% of the population are registered and any rise has not translated into increases in organ donation; indeed, the number of heart-beating donors has fallen since 2004.
Proposed: an opt-out system for organ donation
The possibility of introducing an opt-out system of organ donation has received strong support from the Prime Minister, the British Medical Association,3 the Chief medical Officer and, according to various polls, a significant majority of the public.
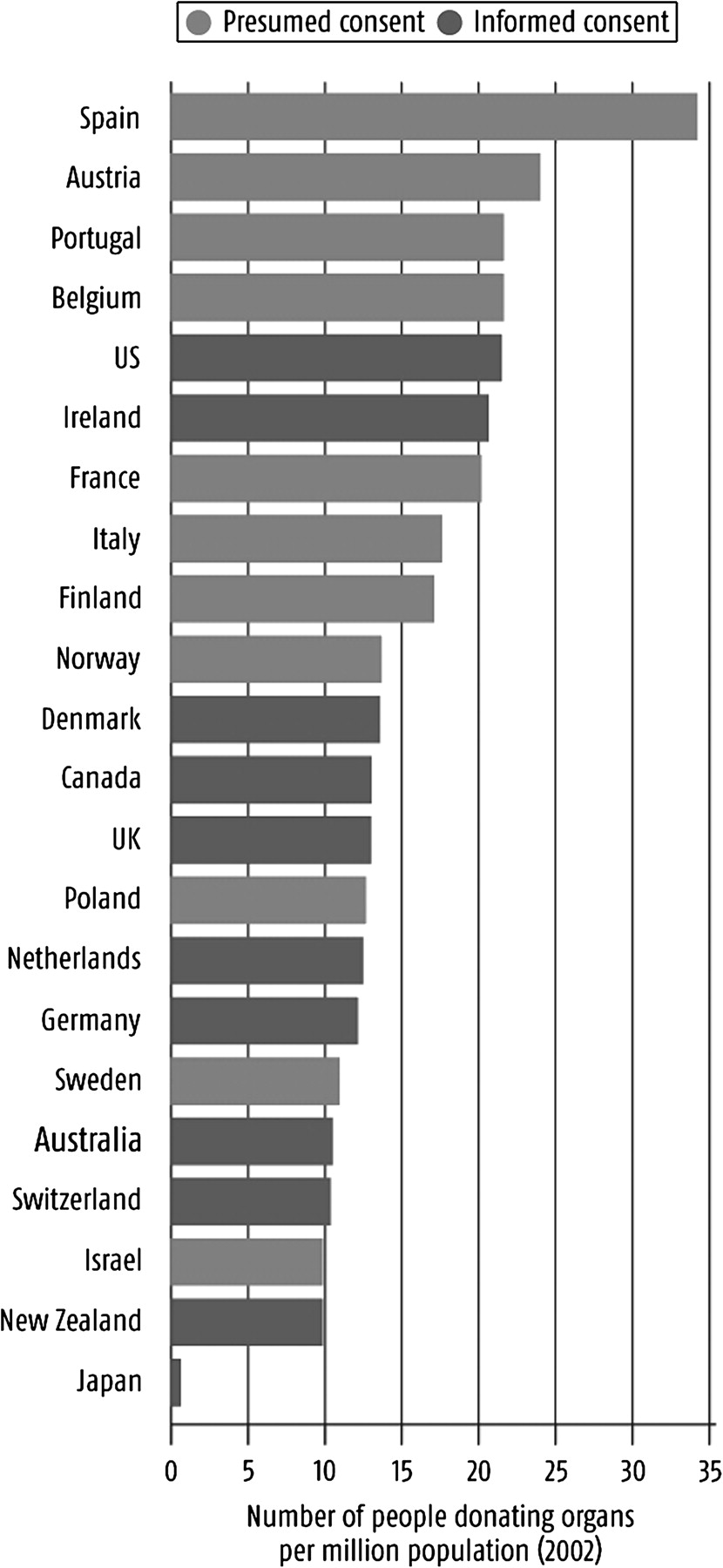
An opt-out system is one where adults are considered to be willing to donate unless they opt out by joining a national register, shifting the default position to presumed willingness to donate. There are two types of opt-out. In ‘hard’ systems the family's wishes are not considered when deciding whether or not to donate. In ‘soft’ policies, as proposed, families can volunteer dissent for any reason, retaining their veto, but in an environment of anticipated donation. Numerous European countries have successfully implemented opt-out systems to increase donation rates (figure 1).
Ethical principles relevant to the taskforce conclusions
The family veto
Family input is viewed as a safeguard. If the deceased has not registered an official position on organ donation but the family know his/her views, these can then be acted on. Paradoxically, this means families can dispute the deceased's wishes. While the families have no ‘rights’ afforded by the law, in practice it is often their wishes that are respected. In principle, the family's wishes are sought in both systems. However, one might predict that under an opt-out system fewer families would override the deceased's wishes. In Belgium, which has an opt-out system, the family refusal rate is 13%, compared with 40% in the UK.4
The default position
Various opinion polls have reported that approximately 70–90% of the public feel positively about donating their organs.3 Why is this not reflected in the default position? Under the current opt-in system the default position of presumed unwillingness to donate has arguably limited both the numbers of donors and the autonomy of potential donors (figure 2, table 1). Under an opt-out system the public, including families of the recently deceased, would be primed to donate unless the deceased had opted out. This would support the overall aim to facilitate potential donors who do not oppose organ donation to donate and, in doing so, save lives. This is echoed by support for a change in policy. The most recent government opinion poll in 2007 showed 64% of the public support a change to an opt-out system.5

A mathematical model to predict autonomy in the two organ donation systems. The model predicts the number of donors in each system; by comparing these numbers to the percentage we would expect to want, or not want, to donate, we can predict autonomy. Numbers used in the model include: 28% of the public are on the ODR; 80% of individuals would like to donate (a conservative estimate from the figure of 86% in the Taskforce's opinion poll below); Number opting out in the proposed system is 14% (the proportion opposing organ donation in the Taskforce report)—the comparable number in other countries can be very small: 2% in Belgium; family refusal in an opt-out system was predicted as 0% when individuals had registered, and 20% if not registered (20% is a conservative estimate given lower rates in similar situation in foreign counties, and the fact that we would expect it to decrease from the current family refusal rate of 40%).
A table to show the results of the mathematical model shown above (figure 2). It shows the number of potential donors, and the percentage of people who achieve or loose autonomy. To achieve autonomy the individual would have wanted to donate and done so, or not wanted and not done so. A loss of autonomy is counted when an individual who did not want to donate does, or when an individual who does want to donate doesn't.
Balancing possible outcomes: loss of autonomy, gain of life
The report emphasises the potential loss of personal choice with an opt-out system but seems not to explore the similar loss in the current opt-in system. This emphasis suggests that the Taskforce think it is worse for an individual who does not want to donate their organs to then donate, than for an individual who was happy to donate not to. Is one type of loss of autonomy better than the other? In the latter position, an individual's organs are not donated despite their wish for this, resulting in the death or suffering of someone on the waiting list. In the former position, an individual's organs are used against their will, benefiting someone on the list.
Furthermore, some individuals who oppose organ donation will become donors under either system, ie, currently some families allow donation when the deceased would not have wanted it, and in an opt-out system an individual may not register despite not wanting to donate. Using data in the report, we can produce a mathematical model to predict the extent of autonomy under the two systems, (figure 2, table 1). This suggests that an opt-out system will greatly increase autonomy. If we consider the Taskforce's position that it is worse to donate when you do not want to, our model suggests that an individual is more than twice as likely to lose autonomy by donating in an opt-in system than in an opt-out system (11% cf. 4.8%). There is presently no way of ensuring one's organs are not donated. For those who oppose donation, an opt-out system would provide a register in which to record their wishes, which may otherwise be unknown. If coupled with our assumption that fewer families will override such wishes, levels of autonomy will be higher (79.2% cf. 62.8%).
The relationship between the patient and state/doctors
The Taskforce highlighted concerns that an opt-out policy would threaten individual rights; that is, there will be a conflict of interest between care of the dying and those waiting for organs, and that the state will gain unwarranted control and ‘exploit’ donors. However, these concerns apply to all systems, and the best solution is to have enough donors.
The gift element
A major argument put forward is that the concept that organ donation as a gift will be lost by moving away from an opt-in system. However, the primary object is not to make people feel good about giving organs but to prolong lives; and anyway, changing to an opt-out system would increase the possibility for people to donate and hence feel good about it.
Assessment of public opinion
The Taskforce concluded that the evidence from the eight reviews they commissioned into public attitudes to opt-out systems was ‘limited and incomplete’. Similarly, discussions with ‘key stakeholders’ revealed practical concerns on the potential change in donor numbers but little on public opinion, except support for an opt-out system alongside efforts to increase awareness of organ donation. This was echoed in letters from individual members of the public, charities and other organisations. The taskforce largely drew its conclusions on public opinion from the surveys discussed below.
Assessment of public attitudes towards organ donation and the influence of education
The Taskforce performed a small survey of 350 members of the public, asking them before and again after ‘deliberative sessions’ whether they were willing to donate their organs. Before the sessions 50% definitely and 36% possibly wanted to donate (a total of 86%), while after the deliberative sessions 61% definitely and 26% possibly wanted to donate (a total of 87%). Thus the overall percentage of people who thought positively, or negatively, towards organ donation did not change significantly after increasing awareness via the sessions. This suggests that future awareness campaigns will have little effect on the number of people willing to donate.
The key finding is that that the majority of the public support organ donation and are willing to donate their organs. This conclusion is supported by previous opinion polls. This highlights the ethical question of whether the organ donation policy should reflect public opinion.
Interpretation of support for change in policy
Subsequently the same 350 members of the public were asked ‘To what extent would you support the law of organ donation in the UK changing from an ‘opt-in’ to an ‘opt-out’ system?’ Figure 3 is taken directly from the Taskforce report.2 It clearly shows that after ‘the events’ (other deliberative sessions) 72% of the public either supported or strongly supported a change in policy.

{kind=link}
{kind=link}
{kind=link}
Evidence for support for a change in the law. Reprinted with full permission from the Organ Donation Taskforce.2
The members of the Taskforce misinterpret these results by stating that, ‘The evidence shows that most people would accept a move to an opt-out system on the basis that they assume this would lead to an increase in organ donation rates’. A more honest statement would comment not merely on acceptance, but support by the majority for an opt-out policy. That the public believes a new system would increase donation, and hence would allow it to save lives, should be better appreciated by the Taskforce.
Instead the Taskforce seemingly overvalue the smaller percentage that oppose the change in the law; ‘However, there is a sizeable minority who are strongly opposed to a system of opt-out, and even those who support it in theory have reservations around about certain issues’. Why, having previously described the 14% of the public who do not want to donate as a small minority, do they now describe the 12% who oppose the change in law as a sizeable minority? It would be more reasonable to emphasise the 43% who strongly support a policy change, or the overall 72% who would support it.
Analysis of faith and belief groups
The taskforce aimed to analyse ‘prevailing attitudes to organ donation and consent in the many and varied cultural and faith groups within the UK’.6 There are two aspects of this: to learn about the official position of faith groups on organ donation, and of the prevailing attitudes of individuals within different groups. The Taskforce's methodology for this involved interviewing only 17 religious ‘leaders’ on the views of their respective religions.
By interviewing leaders one can reasonably analyse the official position of different faith groups. This revealed that ‘While the majority of faith and belief groups permit organ donation, and some even have core beliefs which support it, religion was not described as a key influence for people opting in’. If the majority of faith and belief groups feel positively towards organ donation, it follows that the most appropriate donation policy would have a default towards donating organs, that is, opt-out.
If the aim was to assess the majority opinion of individuals within the groups, the method was inappropriate. A large opinion poll of the individuals whose opinion they wanted would be a valid technique. In effect, the Taskforce have ended up with an opinion poll of only 17 ‘leaders’. Furthermore, as ‘leaders’ of the groups, the background on which they form an opinion is different from those of the ‘grass roots level’ on which they were specifically asked to comment. Indeed, some leaders sensibly suggested that their views and opinions were not necessarily representative of the group they head.
A good example of incongruities between opinions of the leaders compared to those of individuals following a religion is presented in the report. A 2007 study in Birmingham reported that 60% of Muslims, from a wide variety of ethnic backgrounds, thought that organ donation was contrary to their faith. However, discussion with Muslim leaders revealed only that organ donation is an individual choice and not specified by religious guidance.
Moreover, some of the questions provided by the Taskforce in a discussion aid for the interviewers were misleading. One question asked was the ‘faith's position of the current ‘opt in’ system, whereby members of the public need to opt-in, or volunteer, to become a donor?’ It is not clear if the leaders were aware that only 20% of donations come from people on the ODR and hence are voluntary gifts. The consequent conclusion that, regarding the current system, ‘Its key advantage was considered to be that it allowed for free choice, and ensures that organs have been donated under conditions of informed consent’, is a reflection of the misleading question and a lack of understanding.
Another question was, ‘What is your faith's position on the idea of an ‘opt-out’ or ‘presumed consent’ system, whereby members of the public are assumed to be donors unless they have formally opted out whilst alive’. As commented by the Taskforce, ‘presumed consent’ is a misnomer. Consent refers to a well-informed, balanced, decision by the individual, which by definition, can never be presumed. Indeed, even in the current opt-in system, it is hard to argue that registration is equivalent to consent; without interviewing someone it is impossible to know if the decision is informed. By referring to opt-out as ‘presumed consent’, it suggests that an opt-in system would, rather than presuming consent, preserve personal choice by leaving it up to the individual. This is reflected in the interviewees' answers: ‘The opt-out system would not allow for personal choice’. However, people can effectively register their choice in both systems. In terms of people ultimately getting what they want our model (figure 2) suggests greater autonomy is achieved in an opt-out system.
The Taskforce, despite concluding that all religions support organ donation, and that no religious beliefs favour one system of organ donation over the other, draws strong conclusions from the personal opinions of only 17 individuals. Their conclusions are then used as some of the main arguments against a change in organ donation policy.
Impact of opt-out systems
Analysing the potential impact of an opt-out system involved reviewing studies, including an independent systematic review,7 of organ donation in European countries. The review was set out in three parts: the first examined ‘before and after’ studies, the second scrutinised ‘between country’ studies and the last involved surveys of public and professional attitudes to opt-out.
‘Before and after studies’ reveal positive correlation
The Taskforce analysed five studies on the impact of introducing opt-out systems on organ donation in Austria, Belgium and Singapore. All revealed positive associations between policy change and organ donation. In Austria, where legislation changed in 1982, donation rates more than doubled from 4.6 per million people per year (pmp/yr) to 10.1 pmp/yr in 1985. In Belgium, the policy change resulted in the number of kidney retrievals increasing from 18.9pmp/yr to 41.3pmp/yr after 3 yrs, and in Singapore, after opt-out was introduced in 1987, donor numbers increased from 4.7pmp/yr to 31.3pmp/yr.
The Taskforce rejected the significance of the correlation due to confounding influences. Changes in legislation are inevitably linked to contextual changes in a country, including awareness and educational campaigns, as well as improvements in transplantation infrastructure. Effects of this consolidation cannot easily be disentangled from the effects of policy change and hence it remains uncertain which aspects are directly responsible for increasing donors. Nevertheless, given the methodology, the optimum positive result towards policy change was reported; a positive association. Further exploration into the issue of causation, although not done by the Taskforce, is possible.
Two methods of exploring causation
One method is to minimise the influence of external confounders such as publicity, road-traffic accidents and culture etc by performing ‘between region’ studies. A well-cited study of this sort compared two Belgium cities, Antwerp and Leuven.8 The cities had equivalent opt-in systems until a change in policy was made in 1986. At this point Leuven introduced an opt-out policy, while the main hospital in Antwerp refused to adopt the new policy and continued practising opt-in donation. Donation rates rose only in Leuven, where the law was implemented. This strongly suggests changing the law and shifting the default position is instrumental in increasing organ donation.
The second method is to see if the increases in organ donation are sustained after confounding influences such as increased publicity and awareness have ceased. Relevant data available to the Taskforce, and mentioned in the report, came from a 2002 study of 22 countries with different consent systems and donation rates shows the four countries with the highest donation rates have a system of ‘presumed consent’ including Austria, which, even after 20 years, continues to boast an impressive donation rate (figure 1).
Therefore the confounding factors cited by the Taskforce are arguably insufficient to deem the positive correlation between the opt-out systems and increase in donor number irrelevant.
‘Between country studies’
The systematic review considered four robust ‘between country studies’. These compared organ donation rates between (mainly) European countries with different consent systems. Using regression models the studies attempted to identify the effect of policy change separately from other variables. A range of 3–7 variables were chosen, including GDP/health expenditure per capita, mortality rates, incidence of road traffic accidents, transplant capacity, religion and education. Three studies demonstrate a significant association between ‘presumed consent’ and increased organ donation rate (at the 5% level); the last was not significant but nevertheless reported a positive association.
The Taskforce agree that these four studies have no major flaws and applaud their methodology. Having then acknowledged that ‘…overall the evidence suggests that presumed consent law is associated with increased organ donation…’ they eventually refute the conclusions on the grounds of statistical short-comings. In the three sentences devoted to this section in the final report there is no mention that any positive correlation was found, and the last sentence, centrally placed, and in bold italics, reads: ‘The evidence identified and appraised is not robust enough to provide clear guidance for policy’.
Spain, an example
The taskforce over-values the importance of this example, which is of little statistical weight, and makes inferences from contentious data. Strong emphasis is given to the personal opinion of Dr Rafael Matesanz, president of the Spanish National Transplant organisation, who questioned the importance of an opt-out policy for increasing donation rates when compared to infrastructure changes he implemented.
Spain has had an opt-out policy since 1979, and has the highest rate of organ donation in Europe. Increases in donation rates were only seen 10 years after the legislation change, in 1989, seemingly coinciding with new government infrastructure initiatives. One suggestion, argued by the Taskforce, is that increased donation rates are attributable to infrastructure improvements rather than the opt-out policy. However, it could be that an immediate increase in donation was not seen because the infrastructure was, or became, a limiting factor. Despite opt-out unleashing more potential organ donors these could only be realised once systems had improved to accommodate them. While architects of the new infrastructure may claim full responsibility, the opt-out policy may be a necessary pre-condition.
Conclusions
The Taskforce concludes that an opt-out system should not be introduced at the current time because ‘such a system has the potential to undermine the concept of donation as a gift, to erode trust in NHS professionals and the Government and impact negatively on organ donation numbers’. However, concerns about ‘donation as a gift’ and erosion of trust seem to be emotive but unsubstantiated concerns. Furthermore, the evidence they present from foreign countries and UK opinion polls supports the contrary conclusion that organ donations would increase with an opt-out system.
The Taskforce continue by saying that policy change would distract from ‘essential improvements’ to systems, infrastructure and urgently needed increases in public awareness and understanding. These refer to improvements they themselves recommended in a previous report.1 Without taking away from the importance of infrastructure, public attitude towards organ donation is critical. Hence, an opt-out system of organ donation, in which the default position reflects the majority opinion, should be adopted. Furthermore, given the current failure of the ODR and the lack of effect of ‘deliberative sessions’ on changing public opinion, simply promoting the current system would be futile.
I believe both the ethical position and assessment of evidence by the Taskforce is wrong, and the debate into the impact of an opt-out system in the UK should be reopened.
Acknowledgments
Thanks to the Journal of Health Economics, the New Scientist and the Organ Donation Taskforce for their co-operation and the use of their figures. Thanks also to the statistics department at UK Transplant for their help.
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
↵i This information was made available by personal request to the UK-transplant statistical office as data from the National Donor Database. For the latest published data please visit http://www.uktransplant.org.uk, or ring them on 0117 975 7575 and ask.
Other content recommended for you
- Taskforce rejects system of presumed consent for organ donation in UK
- Healthcare students support opt-out organ donation for practical and moral reasons
- Opt-out organ donation without presumptions
- Short-term impact of introducing a soft opt-out organ donation system in Wales: before and after study
- A public opinion survey: is presumed consent the answer to kidney shortage in Hong Kong?
- Elective ventilation and the politics of death
- Normative consent and opt-out organ donation
- Is an opt-out system likely to increase organ donation?
- Presumed consent: a distraction in the quest for increasing rates of organ donation
- Authorisation, altruism and compulsion in the organ donation debate