Article Text

Abstract
Background: Abortion policy varies significantly between Northern Ireland and Norway. This is the first study to compare medical students’ attitudes towards abortion in two different countries.
Objective: To assess medical students’ attitudes to abortion at the University of Oslo (UiO) and Queen’s University Belfast (QUB).
Design: An anonymous questionnaire completed by 59 medical students at UiO and 86 medical students at QUB.
Participants: Students who had completed their obstetrics and gynaecology placements during 2006/2007.
Results: The students’ responses (UiO versus QUB) were as follows: response rate, 95.2% vs 92.5%; stated no religious affiliation, 48.0% vs 4.7%; pro-abortion, 78.2% vs 14.3% (χ2 = 58.160, p<0.001); had seen an abortion while studying medicine, 74.6% vs 9.4% (χ2 = 73.183, p<0.001); in favour of abortion when there was a threat to the mother’s life, 100% vs 93.3% (χ2 = 6.143, p = 0.150); in favour of providing abortion on the mother’s request, 86.4% vs 9.3% (χ2 = 42.067, p<0.001); in agreement that women should have access to free abortion services (mean value on a 5-point Likert scale 1.69 out of 5), versus in disagreement (mean 3.76, p<0.001).
Conclusion: There were significant differences in students’ attitudes to abortion, reflecting differences in religious, legal and educational experiences.
Statistics from Altmetric.com
Abortion has elicited strong but divided feelings from society in general, and decisions to abort raise many complex and important issues. Social challenges to abortion are increasing due to the advances in prenatal diagnostics, including “4D” imaging techniques1 and the improved survival of premature babies.
Abortion policy differs greatly between Northern Ireland and Norway. The UK Abortion Act 1967 does not extend to Northern Ireland and therefore the grounds for permitting abortion in Northern Ireland are more restrictive than in the rest of the UK. In an attempt to clarify the legal situation in Northern Ireland, there has been a recent publication (2007) of draft guidance for health professionals on the termination of pregnancy in Northern Ireland.2
The law governing the termination of pregnancy in Northern Ireland at present can be found in Sections 58 and 59 of the Offences Against the Person Act 1861 and in Section 25 (1) of the Criminal Justice Act (Northern Ireland) 1945. There must be either (a) a threat to the life of the mother or (b) a risk of real and serious adverse harm to the mother’s long-term health.2 The British Medical Association has called for the Abortion Act 1967 to be extended to Northern Ireland to ensure equality of services.1 However, a survey in 2003 among general practitioners and consultants in obstetrics, gynaecology and psychiatry showed that 71% opposed an extension of the Abortion Act to the province.3
By contrast, abortion law in Norway is more liberal and allows abortion on request during the first 12 weeks of gestation. After this stage, a pregnancy may be terminated (a) if the pregnancy, childbirth or care of the child may result in unreasonable strain on the health of the mother or place her in difficult circumstances; (b) if there is a major risk that the child may have a serious disease; (c) if the pregnancy resulted from a criminal act or (d) if the woman has severe mental illness or mental retardation.4 The abortion rate for Norway in 2005 was 12.2/1000 women aged 13–50 years.5
A literature review on healthcare professionals’ attitudes towards abortion showed that attitudes varied depending on nationality, professional background, experience in abortion care, personal attitudes such as religious beliefs and the reasons for women undergoing abortion.6 One study showed the most important personal factors influencing a physician’s decision not to perform abortions included lack of proper training and the person’s ethical and religious beliefs.7
Very little data exists on medical students’ attitudes towards abortion. Any studies that have been carried out have been in the USA,8 9 Mexico,10 South Africa11 and, most recently, the UK.12 This is the first study to compare medical students’ attitudes towards abortion in two different countries.
METHODS
Overview of study design
An anonymous questionnaire was completed by medical students at Queen’s University Belfast (QUB) and the University of Oslo (Universitetet i Oslo; UiO). Data was collected during May and June 2007 from students who had completed their obstetrics and gynaecology placements during the academic year 2006–7. This design was approved by the Research Ethics Committee of the Schools of Medicine, Dentistry and Biomedical Sciences, QUB.
Study population and sampling
On the basis of a pilot study, it was estimated that 80% of the UiO students and 50% of the QUB students would be in favour of abortion. Calculation using a standardised difference formula showed that 45 students were needed in each group to meet conditions specified for the study (power 0.85, p<0.05).
Study instrument
The questionnaire was designed taking into consideration previously published surveys on attitudes to abortion.8–11 The study was reviewed by medical faculty members of QUB and UiO. The questionnaire contained mainly closed questions, with one open-ended question at the end. The first section contained six questions about place of study, age, sex, religion, current year of study and current career intention.
The second section, consisting of 10 questions, evaluated participants’ attitudes to abortion. Students were given the definition of abortion as used by the British Medical Association: “induced termination of an established pregnancy (ie after implantation). It does not include the use of emergency hormonal contraception.”1 This was deemed semantically important, as in Norway the term abortion is ambiguous and is often used to describe a miscarriage.
Statistical analyses
The data was analysed with the Statistical Package for Social Sciences (SPSS) software program (version 15). Independent samples t test was used to compare responses involving the 5-point Likert scale. These included questions relating to conditions affecting the fetus, scenarios relating to the mother and access to free abortion services. This resulted in a mean value ranging from 1, indicating strong agreement with the statement, to 5, indicating strong disagreement. Ordinal scales do not necessarily adhere to rules of addition—for example, two neutral responses (each coded 3) do not necessarily equal one response of agree (coded 2) and one response of disagree (coded 4). Consequently, inferences about differences in population means arising from p values that are close to the significance level of 0.05 should be treated with caution. Standard χ2 tests were used to compare categorical variables.
RESULTS
The responses (UiO and QUB, respectively) were as follows: rate of response from eligible students, 95.2% (59 of 62) vs 92.5% (86 of 93); proportion of eligible students who were women, 71.2% vs 66.3%; respondents stating that they had no religious affiliation, 48.0% vs 4.7%; those who were pro-abortion, 78.2% vs 14.3% (χ2 = 58.160, p<0.001); those who had seen an abortion while studying medicine, 74.6% vs 9.4% (χ2 = 73.183, p<0.001); those who would be unwilling to watch an abortion, 50.6% vs 5.1% (χ2 = 62.398, p<0.001). The UiO students believed their medical school teaching had adequately covered abortion (mean value 2.10), whereas the QUB students thought it had not (mean value 3.84) (p<0.001). Both groups disagreed with the statement “I am more comfortable with medical than surgical abortion” (mean value 3.28 UiO, 3.26 QUB, p = 0.902).
Attitudes to abortion given scenarios in relation to the mother
All the respondents at UiO would permit abortion where continuing with the pregnancy posed a risk to the mother’s life, vs 93.3% at QUB (χ2 = 6.143, p = 0.150). Amost all the UiO students (98.2%) believed abortion should be allowed when continuing with the pregnancy posed a threat to the mother’s health, vs 74.4% at QUB (χ2 = 9.912, p<0.001). The majority of the UiO students believed abortion should be allowed on the mother’s request (86.4%), vs only 9.3% of the QUB students (χ2 = 42.067, p<0.001). Responses to these and other scenarios relating to the mother are represented in fig 1.

Percentages of students at two universities—the University of Oslo and Queen’s University Belfast—who believe abortion should be allowed, according to various scenarios relating to the mother. Life, threat to life; Health, threat to health; Rape, women who have been raped; Disabled, mentally handicapped; <16, less than 16 years old; Married, married, wants no more children; Socioecon, economic or social reasons; No marriage, does not want to marry partner; On request, on woman’s request.
Attitudes to abortion given scenarios in relation to the fetus
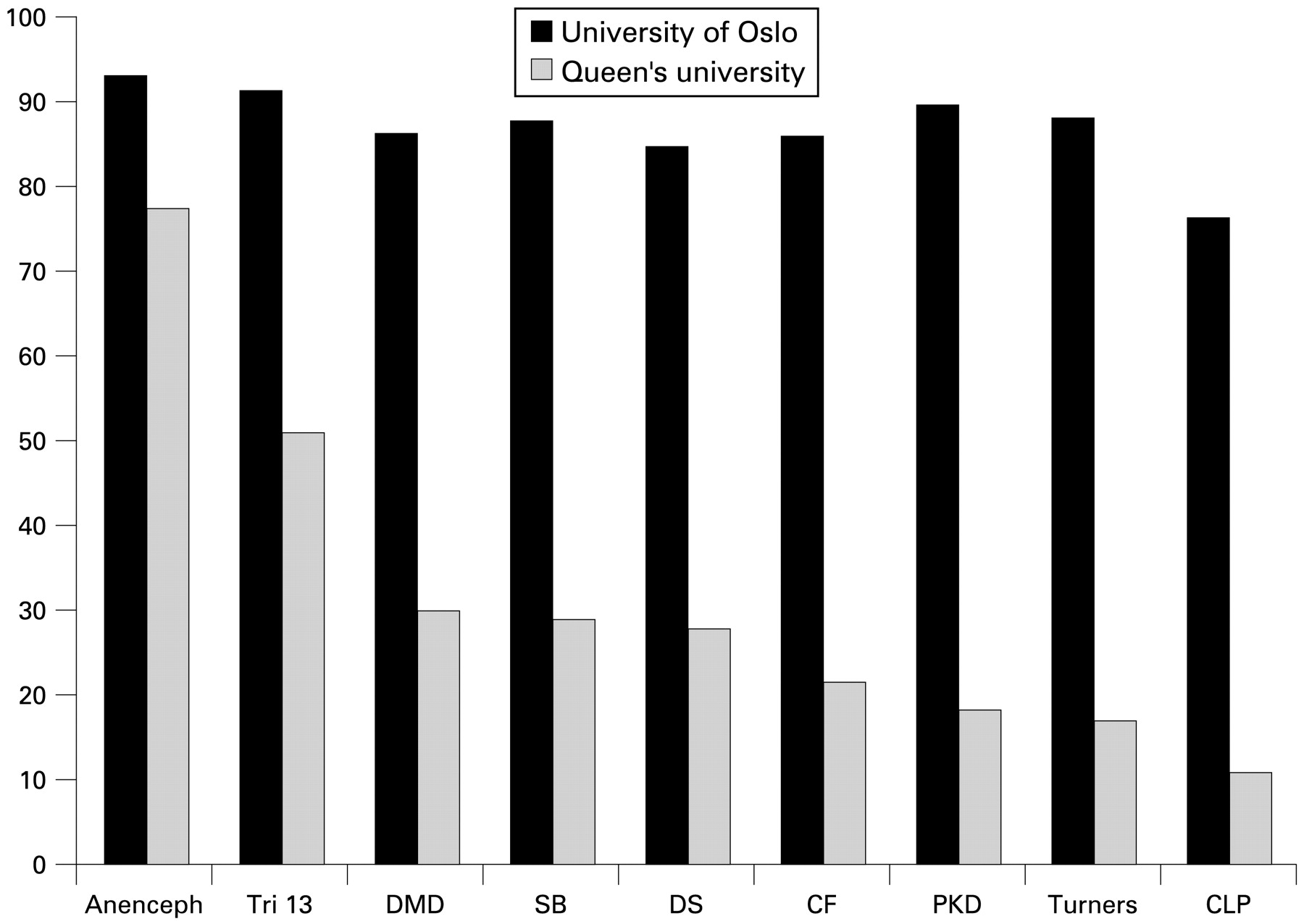
Considering the fetus, the proportions of students who believed abortion should be allowed (UiO versus QUB) were 84.7% vs 27.4% (χ2 = 29.552, p<0.001) if a fetus had Down syndrome and 76.3% vs 10.7% (χ2 = 33.829, p<0.001) if it had a cleft lip and palate. Responses to these and other scenarios relating to the fetus are represented in fig 2.

{kind=link}
{kind=link}
Percentages of students at two universities—the University of Oslo and Queen’s University Belfast—who believe abortion should be allowed, according to various scenarios relating to the fetus. Anenceph, anencephaly; Tri 13, trisomy 13; DMD, Duchenne muscular dystrophy; SB, spina bifida; DS, Down syndrome; CF, cystic fibrosis; PKD, polycystic kidney disease; Turners, Turner syndrome; CLP, cleft lip and palate.
Access to free abortion services
Regarding the statement “all women should have access to free abortion services”, the students at UiO agreed (mean value 1.69) whereas the QUB students disagreed (mean value 3.76, p<0.001).
DISCUSSION
This is the first time that medical students’ attitudes to abortion between two different countries have been studied. The main finding from this study was the strong difference in abortion stance between the two groups, with the UiO students largely pro-abortion and the QUB students largely anti-abortion.
Age and sex of participants
This study found that the attitude towards abortion (pro- or anti-abortion) did not differ in relation to the age or sex of the participant. Therefore, the greater age of medical students at UiO does not explain the difference in results between the two groups. This finding is in contrast to that of a study in Mexico10 involving medical students and physicians, where men and physicians more than 30 years old were increasingly in favour of abortion.
Religion
A Scandinavian study13 of nurses and gynaecologists showed a strong association between degree of religious belief and attitude to abortion. This is consistent with several research studies that show a relationship between religious belief and attitude to abortion.14 15 A recent study of medical students in the UK found that students who practised their faith were more pro-life than non-religious students.12 The students with no religious affiliation comprised the largest group at UiO and were mostly pro-abortion. Only four of the students at QUB stated they had no religious affiliation. This may help to explain the discrepancy in attitudes to abortion between the UiO and the QUB students.
Educational experience
The students at UiO were much more likely to have seen an abortion during their training than those at QUB. Clinical exposure may have affected the Norwegian students’ attitudes to abortion. Espey and colleagues found that of students who had participated in an optional half-day clinical experience in abortion care, 38% reported a change in their attitudes to abortion; 94% of these because more supportive of access to abortion services.16 A recent study in the USA found that early clinical experiences with abortion and family planning can affect medical students’ knowledge, attitudes and intentions to provide abortions.17 Students' overall knowledge and support of abortion services increased following the externships.
Half of the students at QUB would be unwilling to watch an abortion. However, the QUB students stated that abortion had not been adequately covered during their medical school teaching. Even though abortion is limited by law in Northern Ireland, it is important that students are educated about abortion and that their autonomy is respected if they feel they cannot observe the procedure. The most important aspect is that students are taught not to impose their beliefs on patients and that it is their duty to refer the patient to another doctor if they cannot provide aspects of care. A literature review found differences in attitudes between professions, with past and current diversity of education programmes contributing to different formulation of attitudes.6 There are educational opportunities for student-selected components and interprofessional education in this area.
Scenarios relating to the mother
A South African study11 assessed medical students’ attitudes to abortion when there was a threat to the mother’s life and when she had been raped. In comparison with students at UiO and QUB, South African students were less in favour of abortion when there was a threat to the mother’s life or if she had been raped.
The UiO students’ support of abortion for a mentally handicapped mother reflect practice in Norway, where the law states that a woman is allowed an abortion after the 12th gestational week if she is mentally retarded. By contrast, the law in Northern Ireland does not stipulate a learning disability as grounds for an abortion.
The students at QUB were least in favour of allowing an abortion for women in difficult social circumstances, whereas the UiO students were more likely to allow one. In Norway this is a common reason for an abortion: in 2005, 38.1% of abortions performed there after the 12th gestational week were performed for social reasons.5
Abortion on the mother’s request was strongly supported by the students at UiO. These results reflect abortion policy in Norway, which permits a woman to end an unwanted pregnancy on request up until the 12th gestational week. In 2005, 96% of abortions performed in Norway were on the request of women, with no justification required.5 Similarly, in a Swedish study of midwives and gynaecologists, the vast majority supported the Swedish legislation that allows women to have an abortion before the 18th gestational week without giving any grounds.18
Scenarios relating to the fetus
Attitudes to abortion among the QUB students varied significantly depending on the condition affecting the fetus. A majority supported abortion when the fetus had anencephaly or trisomy 13. A minority supported an abortion when the fetus had the other conditions asked about. Similarly to the QUB group, there was a high emphasis placed on the circumstances surrounding the abortion in a study of nurses.19 This showed that 95% of nurses would care for a woman undergoing abortion because of fetal demise in the first trimester, 77% for fetal anomalies incompatible with life and 37% for non-lethal anomalies.19 The QUB students’ attitudes appear to reflect clinical practice in Northern Ireland, where a woman usually continues with her pregnancy when a fetus is diagnosed as having an abnormality.
Anencephaly was the condition affecting the fetus that received most support for abortion from both groups. This may be because the resulting expectation of life is very short.20 In Norway, a fetus whose condition is considered incompatible with life when born may be terminated after the normal cut-off point of 18 gestational weeks. The average life expectancy for infants born with trisomy 13 is 2½ days, with one in 25 surviving to 6 months.21 This may explain the favourable attitudes of medical students to abortion for this condition. For conditions where life expectancy is greater, the students at QUB appeared to be less in favour of allowing an abortion. For a fetus with a cleft lip and palate, which most students are likely to perceive as having less serious consequences, only a small proportion of the students at QUB believed abortion should be allowed, compared with a majority of those at UiO. A study of obstetric and gynaecology residents in the USA found that their willingness to be involved in abortion decreased with decreasing fetal anomaly.22 By contrast, the attitudes of the UiO students are consistent with the findings of a literature review on attitudes towards abortion6 that showed Scandinavian countries to have a more liberal view of abortion. In a Danish study, abortion was acceptable without reservation to 95.1% of gynaecologists, 84.9% of midwives and 77.8% of nurses.13
Medical versus surgical abortion
Both groups disagreed with the statement “I am more comfortable with medical than surgical abortion.” These findings were also reported in a study of medical students’ attitudes to abortion in Washington.8 The authors of that study believed this might be because “medical abortion is a newer and less familiar option. Alternatively students may not differentiate between types of procedures.”
Access to free abortion services
The students at UiO were in agreement that access to free abortion services for all women should be provided. This reflects practice in Norway, where women obtain abortions in public hospitals. By contrast, the QUB students believed that women should not have access to free abortion services. This corresponds with the anti-abortion stance held by the majority of the students and the current situation in Northern Ireland, where women who want an abortion travel to England and have to cover all the costs.
Further research
Further research might investigate attitudes of medical students studying in other countries. Attitudes of students of subjects other than medicine should also be sought.
CONCLUSIONS
This study demonstrates considerable differences in attitudes between medical students at UiO and QUB, with 78.2% of the UiO students being pro-abortion versus only 14.3% of the QUB students. The majority of participants from UiO were in favour of abortion for all scenarios relating to the mother and fetus. Students at QUB seemed to agree more readily with abortion when they did not perceive the situation to be the woman’s responsibility—for example, when there is a threat to her life or health or she has been a raped. For less serious conditions relating to mother and fetus, the QUB students were less likely to be in favour of abortion. These differences probably reflect the differing religious, legal and educational experiences of the two groups of students.
Acknowledgments
The author acknowledges the help of Dr AEW Gilliland (Senior Lecturer, Department of General Practice, Queen’s University Belfast) in supervising the study and Mr M Stevenson for his statistical advice.
REFERENCES
Footnotes
Funding: A medical student elective bursary was provided by the Institute of Medical Ethics.
Competing interests: None declared.
Ethics approval: Ethics approval was obtained from the research ethics committee of School of Medicine, Dentistry and Biomedical Sciences, Queens University Belfast (reference number 07/01).
Provenance and Peer review: Not commissioned; externally peer reviewed.
Linked Articles
- The concise argument
Other content recommended for you
- Patients, not criminals: Northern Ireland grapples with how to provide legal abortion
- Attitudes towards abortion in graduate and non-graduate entrants to medical school in Ireland
- Secular trends in heart rate in young adults, 1949 to 2004: analyses of cross sectional studies
- Cross-sectional study of Australian medical student attitudes towards older people confirms a four-factor structure and psychometric properties of the Australian Ageing Semantic Differential
- Abortion provision in Northern Ireland: the views of health professionals working in obstetrics and gynaecology units
- Attitudes of pharmacy students towards patient safety: a cross-sectional study from six developing countries
- Abortion in Northern Ireland: is change on the cards?
- W George Irwin
- ‘Sorry doctor….I didn’t hear that….’: phenomenological analysis of medical students’ experiences of simulated hearing impairment through virtual reality
- Impact of clinical posting in psychiatry on the attitudes towards psychiatry and mental illness in undergraduate medical students