Article Text

Abstract
Background: Ethical dilemmas are an integral part of medicine. Whether physicians actually feel that they have made ethically problematic treatment decisions or choices in their work is largely unknown. Identifying physicians with ethical problems, and the types of problems and underlying factors, might benefit organisational and educational efforts to help physicians solve ethical dilemmas in a constructive way. We investigated how the frequency and types of ethically difficult treatment decisions vary by specialty.
Method: A mail survey of all non-retired Finnish physicians (n = 17 172, response rate 75.6%) was conducted in 2004. Of those who had made any ethically problematic treatment decisions, the types of decisions and reasons given for these decisions were asked for. Factor analysis was used to investigate clustering of ethically problematic treatment decisions, and logistic regression to investigate the effect of specialty, adjusted for age and gender.
Results: Psychiatrists experienced ethically problematic treatment decisions most frequently, followed by pulmonologists, internists and neurologists. Problems were reported least often by pathologists, laboratory physicians and ophthalmologists. Overtreatment was more common than undertreatment in most specialties, with the exception of psychiatrists who emphasised undertreatment and patient rights issues.
Conclusion: Physicians of different specialties differ significantly regarding frequency and types of ethically problematic treatment decisions they have made. Psychiatrists differ from all other specialists in reporting more undertreatment and patient rights issues. Experiencing ethically problematic decisions might affect the quality of care and physician well-being in many ways. The findings could be useful for both under- and postgraduate ethics education.
- ethical dilemmas
- ethical problems
- medical specialties
- survey
- physicians
Statistics from Altmetric.com
As the technical and scientific complexity of medicine increases, specialisation within the profession also continues to develop. However, physicians are supposed to conform to similar principles of medical ethics and professionalism irrespective of specialty. After their common undergraduate education, the values of physicians are influenced by postgraduate training, peers and the clinical and ethical issues their work presents. Whether physicians of different specialties actually face similar ethical problems is largely unknown.
Experiencing an ethically problematic situation requires both an ethical problem and a sensitivity to recognise it as such. Ethical problems can be empirically investigated from several different points of view. Firstly, values, attitudes or styles of moral reasoning can be investigated. Secondly, ethical sensitivity, ethically problematic decisions and ethical distress can be studied. The frequency, causes and consequences of ethical problems vary accordingly. On the positive side, sensitivity in recognising ethical issues, capabilities of ethical reasoning and holding values conducive to good healthcare might be advantageous to patients. Professional self-control is often considered important for care quality, and there is also some evidence that advanced capabilities of ethical reasoning can improve quality.1–6 On the negative side, ethical problems may indicate an inability of physicians to act in the best interests of their patients and may be a source of work-related stress.7
We conducted a survey to estimate the prevalence of Finnish physicians who had made ethically problematic treatment decisions in their clinical work, the types of problematic decisions, the reasons given for these decisions and how these decisions varied by specialty.
MATERIALS AND METHODS
The survey
A questionnaire about ethics was mailed to all 17 172 Finnish physicians who were not retired in 2004.8 Of the 14 011 physicians (response rate 81.6%) who returned the questionnaire, 12 984 (75.6% of all subjects, 92.7% of respondents) completed the questions about ethics. All analyses were conducted on these subjects. Information about age, gender and specialty were asked for and, for non-respondents, collected from the Finnish Medical Association’s register.
The physicians were divided in five age-groups: under 30 years, 30–40, 40–50, 50–63 and over 63 years. Those aged over 63 years (n = 186) were analysed as one group, because 63 years was the official age for retirement in Finland and most physicians over this age were retired.
There are 49 medical specialties in Finland. As some specialties are very small and their categorisations vary between countries,9 we combined these to form 19 main specialties. Physicians in specialist training were classified according to their future specialty.
Ethical problems
Non-philosophers are likely to understand philosophical terms like “ethical problem” in heterogeneous ways and possibly differently than professional ethicists.10 11 To overcome this challenge of empirical approaches to ethics, we inquired about both general and specific ethical problems. Respondents were first asked whether they had made ethically problematic treatment decisions or choices in their clinical work (yes or no). Seven previously reported ethically problematic decisions were then asked about separately (yes or no): if the physician had made/ordered too few investigations, made/ordered too many investigations, given unnecessary treatments, withdrawn necessary treatments, withheld information from the patient, pressured the patient, or ignored the autonomy of the patient.12–16 In addition, respondents were asked reasons for the ethically problematic treatment decisions/choices with six alternatives: inadequate resources, rush, legislation, treatment guidelines/rules/pressure at the workplace, pressure from patient, or pressure from relatives.
Statistical methods
We calculated the frequency of physicians reporting having made any ethically problematic treatment decisions by specialty. Respondents, who answered yes to the general question about having made ethically problematic choices or yes to any of the alternative problems, were classified as reporting any ethical problems.
We used factor analysis to examine the relationships between different types of ethical dilemmas, and the relationship between different reasons for ethical dilemmas. The factor analysis was based on tetrachoric correlations, as it was reasonable to assume that the dichotomic response variables could be viewed as indicators of the latent structure defined by unobserved continuous scale variables.17 Polycor procedure of the R statistical package (v.2.5.1) was used for estimating a matrix of tetrachoric correlations. The factor loadings were estimated by Survo statistical program (v.2.4.2, Survo System Ltd).18 We grouped the ethical dilemmas and their causes based on this observed factor structure, and used these groups in all analyses. We estimated the statistical goodness of the factor model by assessing the reliability of the measurement scales and the proportion of the common variation of the original variables explained by the factors.19
We calculated the frequencies of different problematic treatment decisions and the reasons given. To explore the relationship between ethical dilemmas and the reasons given, we calculated the frequencies of different reasons given for each ethical dilemma for those physicians, who reported only one ethical dilemma. Logistic regression was used to estimate the association between ethically problematic decisions and medical specialty. Separate models were created with each different ethical dilemma as an explanatory variable, controlling for age and gender. General practitioners were used as a comparison group as they were the largest group. The frequencies and logistic regression analyses were estimated using Stata 8.2 statistical software (v.8.2, Statacorp LP).20
RESULTS
The sample
The socioeconomic characteristics of respondents and response rates are described in table 1. The non-respondents did not differ statistically significantly from respondents by age (mean age 44.9 years for non-respondents, 45.3 years for respondents), although the small group of physicians over 63 years of age had a lower response rate. The response rate was higher for female (78.4%) than for male physicians (72.5%). The response rate for different specialties varied between 71% and 89%.
More than half of Finnish physicians are women. Specialties such as surgery are still dominated by men, whereas women form the large majority of psychiatrists, paediatricians, oncologists and gynaecologists (table 1).
Factor structure of problematic decisions and reasons given
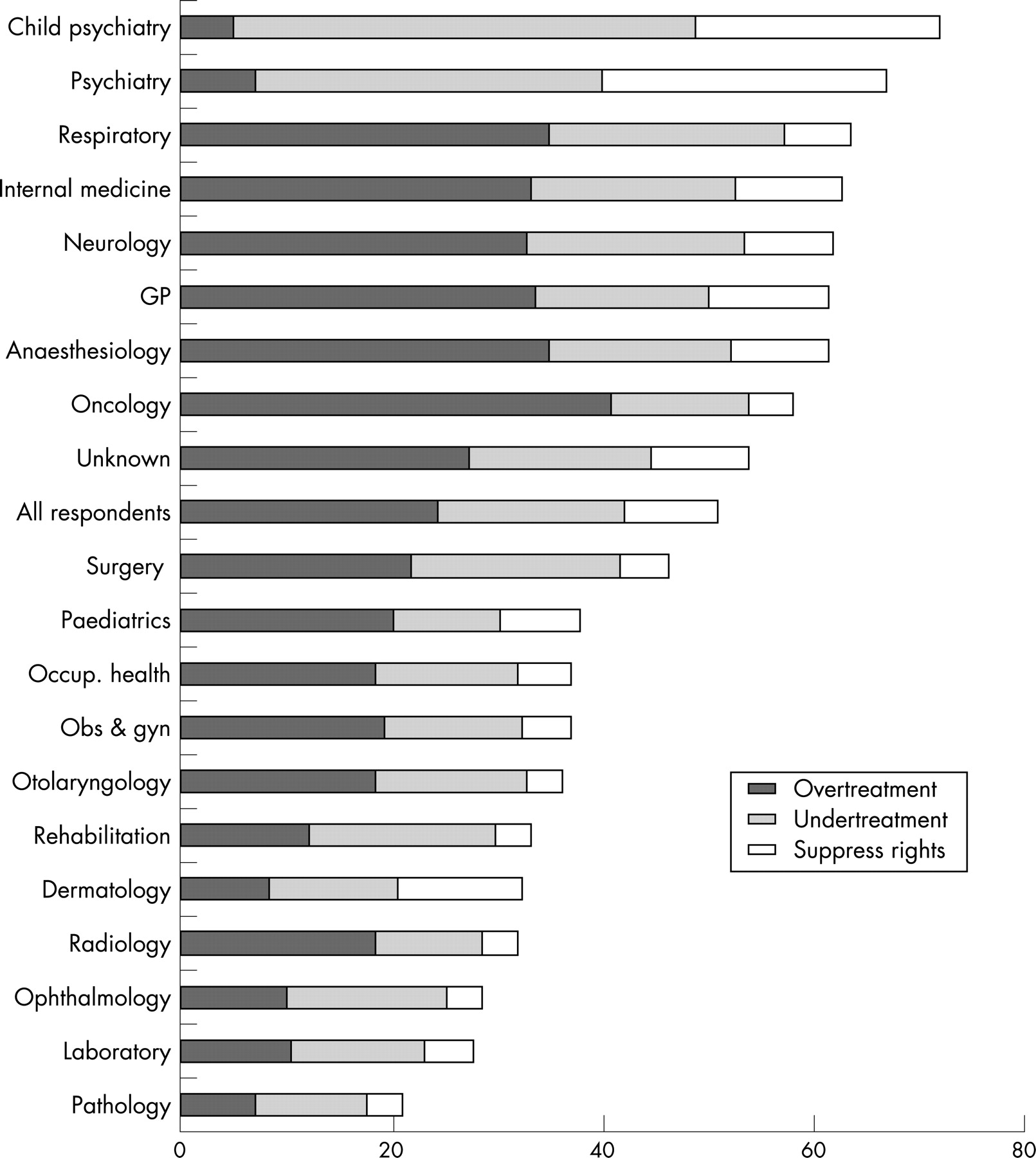
The factor analysis produced a three-factor solution for the ethically problematic treatment decisions: “overtreatment” loaded with having done too many investigations or given unnecessary treatments, “undertreatment” loaded with having done too few investigations or withdrawn necessary treatments, and “suppress rights” loaded with having withheld information from the patient, or pressured or ignored the autonomy of the patient. The reasons for the ethical dilemmas also produced a three-factor solution: “patient demand” loaded with pressure from patient or relatives, “resource constraints” loaded with inadequate resources and hurry, and “law and guidelines” loaded with law and local rules or guidelines. The fit of the factor model was good, with reliability scores of 0.89 for the problems and 0.90 for the reasons19 (Cronbach’s alphas 0.80 and 0.82, respectively), and the model representing 62% of the common variation of the problems and 49% of the reasons.
Frequency of problematic decisions and reasons given
The proportion of physicians who had made ethically problematic treatment decisions varied between 17% and 61% for different specialties (table 2). Ethically problematic decisions were most commonly reported by psychiatrists, oncologists, pulmonologists, anaesthesiologists and neurologists, and least often by pathologists, dermatologists, laboratory physicians and ophthalmologists. Female physicians reported more problematic decisions.
Overtreatment was the most common problem, with the exception of psychiatric specialties, rehabilitation medicine and ophthalmology, where undertreatment was more commonly reported (table 2, figure 1). Patient demand and inadequate resources were fairly equally reported as the most common reasons for problematic decisions, but the specialties emphasising undertreatment reported inadequate resources more often as a reason for the ethically problematic decisions.
{kind=link}
The reasons given by those physicians who report one ethical dilemma only are presented in table 3. Of physicians reporting only overtreatment, 82% explained this by patient demand; 81% explained undertreatment with inadequate resources and 56% explained suppressing rights with rules and guidelines.
Regression analyses
The age and gender adjusted odds ratios for having made ethically problematic treatment decisions are presented in table 4. Psychiatrists experienced ethically problematic treatment decisions most often, followed by oncologists, pulmonologists and general practitioners. Pathologists, laboratory physicians, ophthalmologists, radiologists and dermatologists presented with the least number of problem decisions. The problems that child, adolescent and adult psychiatrists reported were clearly different from other physicians: they reported overtreatment least frequently and undertreatment and suppressing patient rights most frequently, compared to all other specialties. The specialties emphasising overtreatment (relative to undertreatment) most were general practice, anaesthesiology, radiology and paediatrics.
DISCUSSION
We conducted a survey of all non-retired Finnish physicians to study how ethically problematic treatment decisions vary by medical specialty. We found that the proportion of physicians experiencing ethical problems varies widely (between 17% and 61%) by specialty. Psychiatrists experienced ethical problems most and pathologists and laboratory physicians least often. In general, reporting overtreatment was the most common ethical problem, with the clear exception of psychiatrists, who reported undertreatment and suppression of patient rights most often. Overtreatment was explained by pressure from patients and undertreatment by inadequate resources.
Strengths and weaknesses of the study
The most important strengths of our study were the large sample, which allowed a representative sample of even the smaller medical specialties, and the high response rate. To our knowledge, this is the first study comparing all major medical specialties in a representative population of physicians. However, as our study was cross-sectional, no conclusions about causality can be made.
Classification of medical specialties is difficult, as the number of medical specialties varies widely between countries. For example, the European Union recognises 52 medical specialties, of which 10 are not found in Finland. In addition, the actual work and responsibilities of physicians within the same specialty might vary between countries. To overcome these problems, we combined the smallest and least international specialties to form 19 common and internationally applicable categories of medical specialties.
Our results describe the situation in Finland, and international studies are needed to investigate whether the trends identified are observed elsewhere. In addition, as there were no established, well-validated and very short instruments for evaluating ethical problems,21 22 we had to use our own questionnaire. This limits direct comparison to other studies. As we inquired specifically about ethical problems related to clinical practice, ethical dilemmas of specialties with little patient contacts may have been under-reported. More generally, the true consequences of having made ethically problematic treatment decisions are difficult to investigate without burdensome methods, as this would also require knowledge of the personality, values and objective working conditions of the physicians. Thus we think that the relative differences between specialties are the main findings of our study, while the absolute proportions of physicians reporting ethical problems are difficult to interpret.
Comparison to previous studies
We are aware of no directly comparable study that has included all medical specialties. Most surveys have included only a few specialties,23–28 or investigated specific ethical issues (eg, attitudes to end-of-life decisions or patient autonomy.)29 30 An overwhelming majority of studies on ethical distress in healthcare concern nurses.21
Experiencing ethically problematic treatment decisions can reflect healthcare problems in many ways. First, they may reflect differences in real work conditions between specialties—for example, inadequate resources in psychiatry leading to undertreatment, and excessive pressure from patients in general practice leading to overtreatment. Second, they might indicate ethical distress experienced by physicians: psychiatrists with intensive patient contact report ethical problems most often, whereas specialties with few patient contacts report the least. Having to practise against one’s ethical convictions might threaten professional attitudes through distress and negative coping strategies. More theoretically, differences in reporting might also reflect different personalities or values held by physicians in different specialties.31 32
A Swiss study investigating the work satisfaction of paediatricians, internists, general practitioners, surgeons and psychiatrists found that that psychiatrists were least satisfied and paediatricians most satisfied with the care they provided.28 This was measured by asking, for example, about the quality of care provided, the possibility of referring patients to a specialist if needed and the possibility of treating patients in one’s own way. These results are in line with our findings, with psychiatrists five times more likely than paediatricians to report undertreatment. A study comparing psychiatrists’ and GPs’ loyalty between patients and society found little difference between these specialties.26 Thus it is likely that our results at least partly reflect true differences in working conditions and not just in attitudes.
A US study of ethical dilemmas faced by three specialties found that critical care specialists reported ethical dilemmas most often, followed by oncologists and internists24; this difference was not found in our study. Of those physicians reporting issues related to resource allocation, a slightly larger proportion reported using unnecessary resources than forgoing necessary resources,25 which is generally in line with our findings. In addition, the study found that general internists most often reported experiencing ethical problems related to justice, oncologists problems related to truth telling and critical care specialists problems related to end-of-life and decisional capacity issues.27 A previous Finnish study about attitudes of physicians found that oncologists were more ready to forgo life-sustaining treatment in terminal care than surgeons, general practitioners or internists. Oncologists were most and surgeons least influenced by family appeals.33 These findings could at least partly explain why, in our study, oncologists reported more overtreatment (explained by pressure from patients) and less suppressing of patient rights, whereas surgeons reported less overtreatment than internists and general practitioners.
A Norwegian study investigating physician attitudes on patient autonomy found psychiatrists had the least paternalistic attitudes, compared to surgeons, laboratory physicians and medical specialties, whereas general practitioners and specialists in social medicine had intermediate attitudes.29 This difference in attitudes could at least partly explain our finding that psychiatrists emphasise ethical dilemmas related to suppressing patient rights more, and surgeons less, than general practitioners. It is also possible that if psychiatrists value patient wishes more highly than other specialties, they also suffer more when these wishes can not be fulfilled due to lack of resources or other reasons outside the physicians and patients control.
CONCLUSIONS
The results of our study show that the ideal of common medical ethics education for all medical specialties might not optimally support contemporary practising physicians. Considering the ever-deepening sub-specialisation of medicine, this might not be surprising. Instead, ethics education and support systems could benefit from knowing how different specialties challenge physicians with different ethical problems. Our results could be used as a foundation for ethical discussions within different medical specialties. Further studies investigating the causes of the trends observed are warranted.
REFERENCES
Footnotes
Funding: The mailing of the questionnaire and statistical analyses were funded by the Finnish Medical Association.
Competing interests: None.
Other content recommended for you
- Ethical decision making in intensive care units: a burnout risk factor? Results from a multicentre study conducted with physicians and nurses
- Physicians' Ethics Forum: a web-based ethics consultation service
- Moral distress among Norwegian doctors
- Why doctors use or do not use ethics consultation
- Clinical ethics, information, and communication: review of 31 cases from a clinical ethics committee
- Military physicians’ ethical experience and professional identity: a Canadian perspective
- Dismembering the ethical physician
- Ethical aspects of time in intensive care decision making
- Ethical decision-making about older adults and moral intensity: an international study of physicians
- A review of tobacco smoking and smoking cessation practices among physicians in China: 1987–2010