Article Text

Abstract
Background: Ethics support services are growing in Europe to help doctors in dealing with ethical difficulties. Currently, insufficient attention has been focused on the experiences of doctors who have faced ethical difficulties in these countries to provide an evidence base for the development of these services.
Methods: A survey instrument was adapted to explore the types of ethical dilemma faced by European doctors, how they ranked the difficulty of these dilemmas, their satisfaction with the resolution of a recent ethically difficult case and the types of help they would consider useful. The questionnaire was translated and given to general internists in Norway, Switzerland, Italy and the UK.
Results: Survey respondents (n = 656, response rate 43%) ranged in age from 28 to 82 years, and averaged 25 years in practice. Only a minority (17.6%) reported having access to ethics consultation in individual cases. The ethical difficulties most often reported as being encountered were uncertain or impaired decision-making capacity (94.8%), disagreement among caregivers (81.2%) and limitation of treatment at the end of life (79.3%). The frequency of most ethical difficulties varied among countries, as did the type of issue considered most difficult. The types of help most often identified as potentially useful were professional reassurance about the decision being correct (47.5%), someone capable of providing specific advice (41.1%), help in weighing outcomes (36%) and clarification of the issues (35.9%). Few of the types of help expected to be useful varied among countries.
Conclusion: Cultural differences may indeed influence how doctors perceive ethical difficulties. The type of help needed, however, did not vary markedly. The general structure of ethics support services would not have to be radically altered to suit cultural variations among the surveyed countries.
Statistics from Altmetric.com
Ethical difficulties often arise in clinical care,1 and the number of ethics support services, committees or consultants is currently growing in many European countries.2–5 Growing evidence suggests the usefulness of these services,6,7,8,9,10,11 but evaluation has centred on the US. Although the experience of ethical difficulty itself is certainly expected in clinical practice everywhere, the types of difficulties encountered, how difficult they are considered to be and the perception that ethics support services can be of help may vary in different countries.12,13 Three reasons for this are as follows.
-
When faced by an ethical difficulty, reaching a decision that is ethically justified and acceptable to all concerned may be a complex process. This makes variation likely both within and between countries.
-
Differences in cultural constructs of health, disease, death or how medicine ought to be practised may affect the experience of ethical difficulties and of the usefulness of help in different countries.14–17 Although, clearly, nationality does not subsume culture, it is usually considered to be one of the circles within which some degree of culturally shared elements is contained.
-
Healthcare services themselves vary to such a degree that the European Commission recently renounced the project of centralised regulation.18
Differences in the perception of ethical difficulties, and of the usefulness of ethics support services, can be compounded by these variations. Thus, there is a need for comparative data on experiences with ethical difficulties faced by doctors, both in different cultural environments and in different healthcare systems. In Europe, there has been no comparative exploration of the experience of doctors facing ethical difficulties, including which situations they find the most difficult to resolve, how satisfied they are with current resolution of ethical difficulties and the types of help they would consider useful.
To deal with these three questions, we conducted an international survey of doctors in Italy, Norway, Switzerland and the UK. We chose these four countries for the diversity of their healthcare systems and cultural traditions within Europe. All of them offer universal access to healthcare.
PARTICIPANTS AND METHODS
Participants
Doctors were identified through the 2002 official list of the Norwegian Medical Association, the Swiss Medical Association, published listings of UK general practitioners and general physicians, and regional listings of Italian general practitioners and members of the Italian Society of Internal Medicine. A random sample of 400 doctors was drawn in each country, in proportions of general physicians, general practitioners and general internists, reflecting that of each country’s population of doctors. This choice was based on a concern to capture similar populations of doctors, who carry out the same kind of work in general internal medicine, in both inpatient and outpatient care.
Survey methods
We used items from the survey instrument developed by DuVal et al19 to explore similar issues among US internists. We developed the Ethics Experience Scale (Cronbach’s α = 0.72) and the Perceived Usefulness of Help Scale (Cronbach’s α = 0.87) from individual items in the original questionnaire. These were not intended as scales by their authors, but showed good internal consistency in our study. We also used items that dealt with what respondents considered to be the most difficult kind of dilemma and their satisfaction with the resolution of a recent case. We gathered demographic information and explored how much prior training in ethics was reported by our respondents.
The Ethics Experience Scale was worded as follows: “In the last two years, how often have you been in the following situations?” The situations listed included treatment of patients with impaired or uncertain decision-making capacity, disagreement among care givers, limiting life-sustaining treatment, and also issues such as requests for assisted suicide or euthanasia and scarcity of resources (fig 1). Response options were never (0), rarely (1), sometimes (2) and often (3). The summed scale score range was 0–36. Respondents were then asked to identify the type of ethical dilemma or problem they found the most difficult to resolve.

Experience of ethical difficulties. Percentages shown in valid per cent. *Kruskal–Wallis, p<0.01.
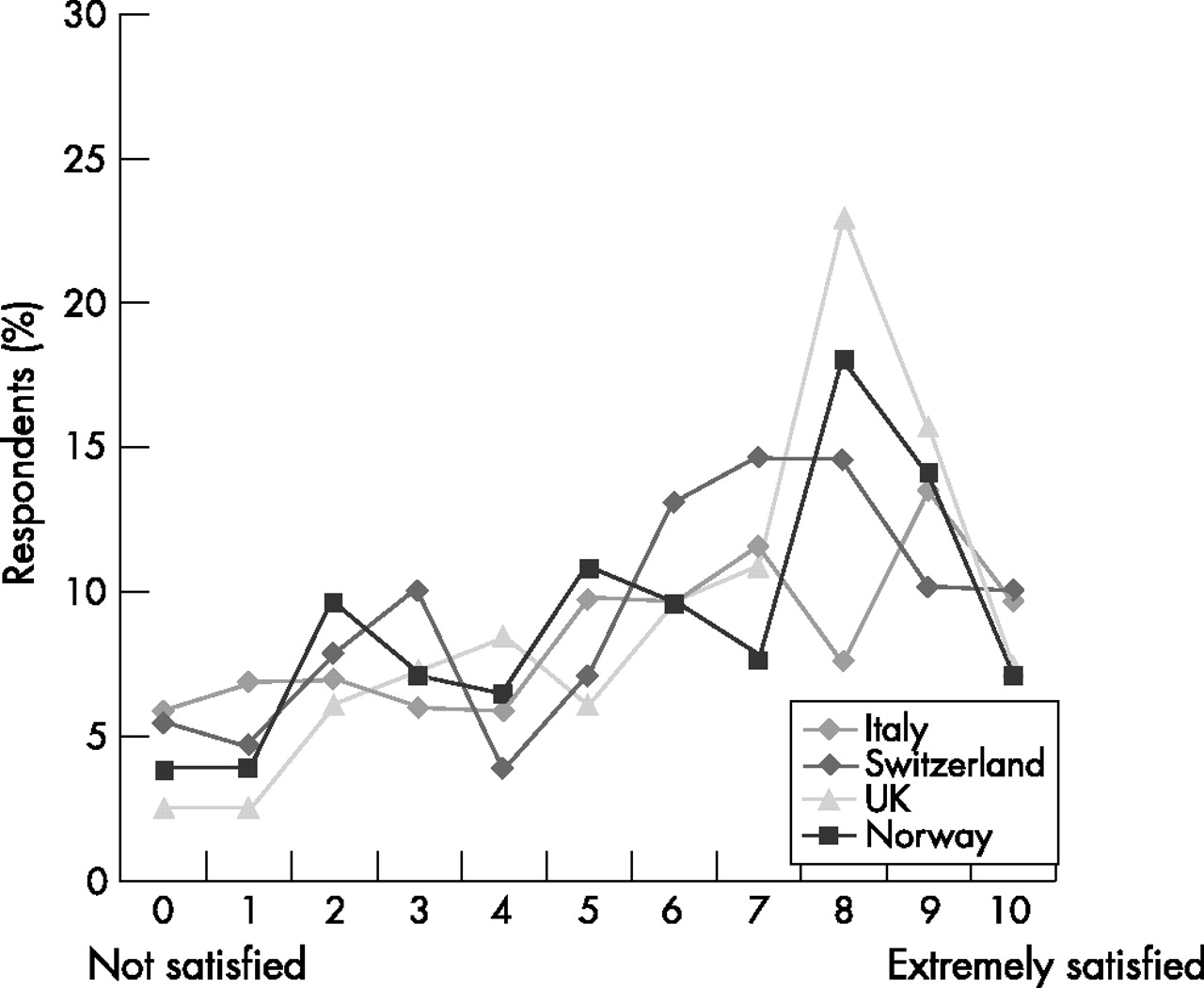
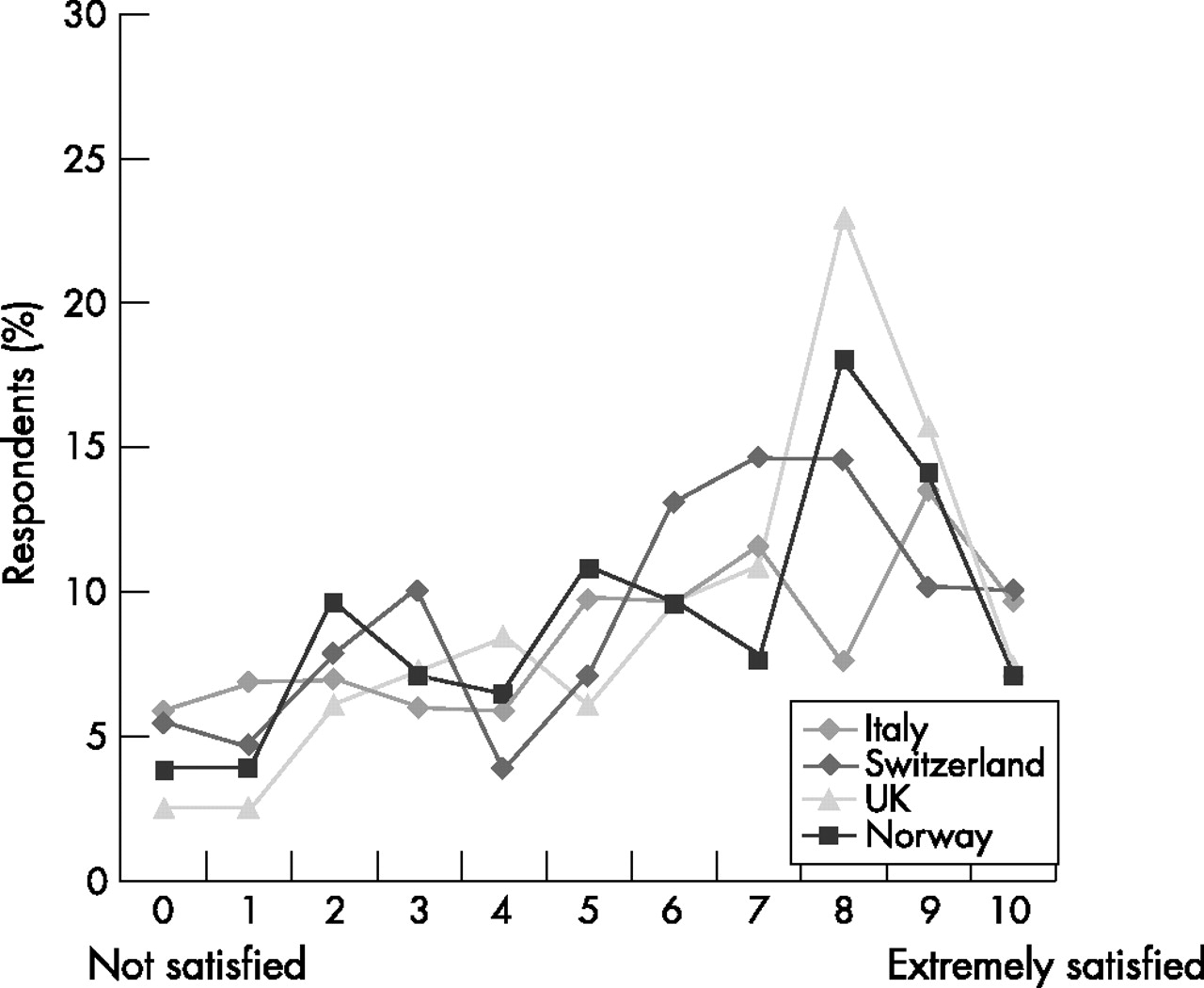
After asking for an example of an ethically difficult situation, respondents were questioned about their satisfaction with the resolution of this case in the following way: “How satisfied are you with the decisions that got made in this situation?” Responses were on a 11-point visual analogue scale ranging from not satisfied (0) to extremely satisfied (10).
The Usefulness of Help Scale, which was administered after the question soliciting an example of an ethically difficult situation, was worded as follows: “In reflecting back on the case, could you have used: …”. The forms of help listed included clarification of the issue, help in reviewing standard of ethics, help in weighing possible outcomes, alternative suggestions and the provision of ethics literature, and also professional reassurance that the decision was correct (fig 2). Response options were no (0), I don’t know (1) and yes (2). The summed scale score range was 0–28.

Types of help considered useful. Percentages shown in valid per cent. *Kruskal–Wallis, p<0.01.
The complete questionnaire was piloted on a convenience sample of doctors. Scales were tested for internal consistency after the pilot, and again on the full sample. The survey instrument is available on request.
The questionnaire was translated into Norwegian, French, German and Italian, back translated to assess accuracy and checked by bilingual doctors. Participants were contacted by mail and told about the aims of the study in a cover letter. Questionnaires were self-administered by the respondents. A repeat mailing was sent, with an incentive of €10 or the closest equivalent in local currency that could be enclosed as a single bill. Data were collected from February 2003 to June 2004.
Protection of human participants
Participation was voluntary and responses were made anonymous before analysis to ensure confidentiality. The institutional review board of the National Institute of Child Health and Development at the US National Institutes of Health, and the Trent Multi-Centre Research Ethics Committee in the UK approved the study. This study was examined and designated as exempt from ethics committee review by the institutional review boards in Norway, Italy and Switzerland.
Statistical analysis
Data were analysed using descriptive statistics, and bivariate correlations were analysed using Pearson’s χ2, Spearman’s rank correlation, Mann–Whitney U or Kruskall–Wallis tests as appropriate. We selected a significance level of 0.01 (two tailed). A multinomial logistic regression was used to identify variables associated with the perception that help would be useful in resolving ethical difficulties, as reported on the Usefulness of Help Scale. The model was built by using the variables that were found to be associated with the perception that help would be useful in bivariate analysis—namely, doctors’ age and number of years in practice since graduation, degree of experience with ethical dilemmas, satisfaction with the resolution of a recent case, confidence about knowledge in ethics, as well as the number of hours a week spent in inpatient or outpatient care, and having a hospital as a primary practice site.
The funding sources were not involved in the study design, collection, analysis or interpretation of data, in the writing of the report or in the decision to submit the paper for publication.
All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
RESULTS
Respondents
Respondents (n = 656, 43% of eligible sample) ranged in age from 28 to 82 years, they had been in practice for an average of 25 years, and 38.4% were at least partly hospital based (table 1). Respondents were predominantly men (85%), with the proportion of women ranging from 42.1% under the age of 30 to 7.8% from 61 to 70 years. A third of respondents (35.6%) reported having ethics courses in medical school. Just over half (53.8%) were somewhat confident of their knowledge of ethics. Only a minority (17.6%) reported having access to ethics consultation in individual cases and only 13.6% had ever used such services (table 1).
Respondent characteristics
Experience with ethical difficulties
The mean score on the Ethics Experience Scale was 10.12, with a range of 0–25 for a maximum of 36. For example, a score of 10 may mean that the respondent experienced three types of ethical difficulties often and one type rarely, or experienced five types of ethical difficulties sometimes, or 10 types rarely. Virtually all (99.4%) respondents reported experiences with at least one of the proposed types of ethical difficulties (fig 1). The difficulties most often reported were uncertain or impaired decision-making capacity (94.8%), disagreement among caregivers (81.2%) and limitation of treatment at the end of life (79.3%). The types of difficulties most frequently described as the most difficult were requests for euthanasia or doctor-assisted suicide, disagreement among caregivers, impaired or uncertain decision-making capacity and uncertainty about whether to disclose the diagnosis to the patient (table 2).
Issues most frequently described as the most difficult
Doctors reported encountering more ethical difficulties if they had specialty training in internal or general medicine, were hospital based or worked more hours a week in inpatient care. Doctors who worked in hospitals were more likely to report difficulties with end-of-life decisions, treating adults with impaired decision-making capacity, disagreement with caregivers, scarcity of resources or patient disagreement on cultural or religious grounds. Doctors in outpatient practice were more likely to report situations where their preferred course of treatment was in conflict with rules for payments of services. Respondents from the UK or Switzerland reported more experience with ethical difficulties than did doctors from Norway or Italy. Respondents reported fewer ethical difficulties if they were older, had worked longer since graduation or worked more hours a week in outpatient care (table 3).
Variables associated with experience of ethics, satisfaction with the resolution of an ethical difficulty and perception of help as useful in bivariate analysis
Satisfaction with the resolution of a recent case
When asked to describe a recent ethical difficulty and to rate their satisfaction with the resolution of this situation, a little under half (47.2%) of the respondents reported a satisfaction level of at least 7 on a visual analogue scale of 10 (fig 3). A quarter (25.7%) expressed dissatisfaction (score ⩽3). Doctors who had more experience with ethical cases were considerably less satisfied with the resolution of the recent case they described (table 3).
{kind=link}
{kind=link}
{kind=link}
Satisfaction with the resolution of a recent case. Percentages shown in valid per cent.
Perception that help would be useful
The mean score on the Usefulness of Help Scale was 10.59, with a range of 0–28. Most (81%) respondents thought that at least one type of help would be useful in the case they had described (fig 2). The types of help most often identified as potentially useful were professional reassurance that the decision was correct (47.5%), someone capable of providing specific advice (41.1%), help in weighing outcomes (36%) and clarification of the issues (35.9%). The types of help least often identified as useful were provision of relevant ethics literature (20.9%), help in talking things through with the patient (24.3%) and mediation of conflict (29.4%).
Doctors were more likely to agree that help would be useful if they were women, hospital based, worked more hours a week in inpatient care and encountered more ethical difficulties. They were less likely to agree that help would be useful if they were older, worked more hours in outpatient care, were more confident about their knowledge in ethics or more satisfied with the resolution of the recent case they described.
In multinomial logistic regression, doctors were more likely to report that they would welcome help if they reported greater experience with ethical difficulties (odds ratio (OR) 1.14, 95% confidence interval (CI) 1.04 to 1.24) and were less likely to report a perception that help would be useful if they felt more confident about their own knowledge of ethics (OR 0.32, 95% CI 0.18 to 0.58). Doctors’ age, sex, number of hours a week spent in inpatient or outpatient care, having a hospital as a primary practice site and satisfaction with the resolution of a recent case were no longer independently correlated with the perception of help as useful in the logistic regression model.
Country variations
We found significant differences among the four surveyed countries regarding the reported frequency with which doctors experience most ethical difficulties (fig 1). The most striking were uncertainty about whether to disclose the diagnosis to the patient, scarcity of resources, conflict with rules for payment of services, requests for euthanasia and assisted suicide, and conflict with the patient’s insurance status. In contrast, we found fewer differences regarding the perceived usefulness of help (fig 2). Clarification of the issues and mediation of conflict were perceived as less useful in Switzerland, help in talking things through with the patient was perceived as helpful more often in Italy, as was provision of relevant ethics literature in Italy and the UK. A discussion in advance was perceived as less useful in Norway.
DISCUSSION
In all the surveyed countries doctors experience ethical difficulties. The types of ethical difficulties most often encountered, as well as those considered most difficult, varied considerably across borders. Despite this, the types of help considered useful by doctors were remarkably stable across the four countries. Despite high satisfaction with the resolution of a recent case, most doctors believed that some kinds of help would have been useful in this case.
Our study has several limitations. Firstly, ethical difficulties are not always easy to identify and using self-reports may thus have led to under-reporting of ethical difficulties. Self-reports, however, allow insight into those cases that trouble doctors. Secondly, asking doctors what kind of help would have been useful in a recent case may have led to under-reporting of the kinds of help considered useful, as most cases are amenable to only certain kinds of help and may not reflect the overall experience of the respondent. This, however, also grounds reflection about the usefulness of help in a real-life case from the respondent’s experience. As we surveyed only general physicians, generalisations to other medical specialties should be cautious, as should generalisations to different countries. Although the four countries we surveyed do represent a reasonable reflection of variation in Western Europe, results from countries with different histories or healthcare systems, such as Central and Eastern European countries, may differ substantially. The response rates of doctors to mailed surveys are generally modest,20 but we would have liked to have a higher response rate. Non-respondent bias is most likely to be associated either with lack of time or with lack of interest in the topic. In the first instance, we would expect an under-reporting of experience with ethical difficulties in inpatient care, where this variable was associated with increased working hours. In the second instance, we may have to expect an over-reporting of ethical difficulties and of the perceived usefulness of help. By extrapolating our results to a response rate of 100% and considering all non-respondents to report no experience of ethical difficulties and no perception that help would be useful, however, the proportion of doctors reporting each would still be 41% and 36%, respectively. Finally, other healthcare professionals, as well as patients and their relatives, may also have a different perception of the kind of ethical difficulties encountered in clinical practice.21 Indeed, patients’ own experiences with ethical difficulties in facing disease and their difficulties with aspects of healthcare systems that they consider to be ethically problematic are two distinct and inter-related areas where further research is needed.
This study has several implications. Firstly, although the experience of ethical difficulties was seen in all the surveyed countries, the frequency of ethical difficulties encountered, and those perceived as most difficult, varied among countries. Among the striking differences was a much lower prevalence of patient disagreement for non-religious or cultural reasons in Italy, along with a higher prevalence of uncertainty about whether to disclose diagnosis among Italian respondents (fig 1). This suggests a more paternalistic model of medicine, in which the doctor is entrusted with decisions and patient participation may be viewed as more problematic. Difficulties related to requests for euthanasia and assisted suicide were much more prevalent in Switzerland, reflecting the legal situation of assisted suicide in this country. More intriguingly, difficulties with rules for payments of services were reported more often in Switzerland and in Norway, as were insurance status conflicts in Switzerland, suggesting that the structure of the healthcare system in these countries may confront doctors with ethical difficulties more often. These differences should indeed suggest caution against generalisation across cultural boundaries regarding the kinds of ethical dilemmas encountered in clinical practice. Such generalisations may lead to impoverished accounts of the kinds of ethical difficulties encountered by doctors in various cultural settings and to unwarranted inferences from one culture to another. Indeed, the experience of European doctors and other healthcare providers with ethical difficulties is a topic for further empirical research. Comparative data from countries with different histories or healthcare systems, such as the Central and Eastern European countries, would be especially interesting. As difficulties associated with euthanasia or assisted suicide were ranked high on difficulty by respondents from all four countries, data from Belgium or The Netherlands would bring a richer perspective to the four countries we surveyed.
The preferred types of help—namely, professional reassurance that the decision was correct, someone capable of providing specific advice, help in weighing outcomes and clarification of the issues—seem to have an underlying model in common: that of calling on an expert to solve a puzzle. The types of help that imply a stronger component of self-engagement in the process of solving an ethical difficulty are less often preferred. This may suggest that doctors view ethics consultation as a last resort, when they believe that their own efforts are no longer sufficient.22 Furthermore, despite the diversity in the types of difficulties encountered, the kinds of help perceived as useful were strikingly similar. Interestingly, then, although different sensitivities to ethical problems are evident in the four countries we surveyed, doctors have a common perception of the help they need. Although sensitivity to local cultural elements is likely to be an indispensable component of ethics consultation, our findings suggest that the general structure of ethics support services would not have to be radically changed to suit cultural variations, at least among the surveyed countries. And indeed, despite concerns about importing models for ethics consultation, such services are reporting positive experiences in many Western European countries.2–5,18,23,24 This disconnect between important differences on the kinds of difficulties encountered and lesser differences on the kinds of help considered useful is noteworthy. One possible interpretation is that this is because of a shared structure of ethical difficulties across different contents. Indeed, ethical difficulties with contents ranging from limitation of life-sustaining treatment to difficulties in facing scarcity do share structural elements, such as uncertainty among doctors on how to approach value-laden decisions, tension between values as understood by the professionals or dissent about the ethical judgement among the people concerned.25 The inference that different experiences must result in different kinds of help may not hold as widely as we sometimes assume. This finding suggests that similar ethics consultation processes can apply to difficulties of different content.26 Processes developed for ethics consultation, including those developed within Europe,27 may thus be useful across national boundaries to a wider extent than was initially thought.
Increased experience with ethical difficulties was associated with greater perception that help would be useful. Two interpretations come to mind. Firstly, doctors who are less able to resolve ethically problematic cases on their own may perceive more of them as difficult, at the same time perceiving help as more useful. Alternatively, increased experience with ethical difficulties may be an expression of greater moral sensitivity. Sensitivity to ethical difficulties, including the ability to identify them, is not a straightforward matter.28 The finding that respondents with more training in ethics tended to be less satisfied with the resolution of the case they described suggests that the second interpretation may be correct. And indeed, ethics consultation does not necessarily deal with theoretical knowledge but with the process of making space to discuss a problem from several angles.21,29
Finally, our findings highlight the prevalence of ethical difficulties and the perceived usefulness of help in outpatient medicine. Currently, clinical ethics committees and consultants tend to be centred in hospitals, and access to the help they provide is even more scantly distributed to doctors in outpatient practice than it is in hospitals. Further development of these services should take this element into account.
CONCLUSION
Ethical difficulties exist in clinical practice in all surveyed countries, with important differences among countries regarding both the frequency of different kinds of dilemma and their perceived difficulty. The kinds of help that doctors would consider useful, however, varied much less across countries. This suggests that, although ethics support services will necessarily have to function in culturally sensitive ways, they may not require fundamental changes in their basic structure to meet the perceived needs of doctors in these countries. It also suggests that ethical difficulties, different as they may be in content, share common features regarding the structure of the perceived problem. If that is so, it should not be surprising that responses considered helpful are not as diverse as the problems they intend to deal with.
Acknowledgments
We thank Gary Gensler and Dr Gordon DuVal for allowing us to use their questionnaire, the National Institutes of Health Clinical Center Library for its outstanding translation service, MEDTAP International for its excellent data collection work, and Dr Vardit Ravitsky for invaluable criticism of the manuscript. We also thank all the doctors who took the time to complete the questionnaire.
This work was funded by the Department of Clinical Bioethics at the National Institutes of Health, and was conducted while SAH was a fellow at this department. SAH was funded in part by the University Hospitals of Geneva, the Oltramare Foundation and the Centre Lémanique d’Ethique.
REFERENCES
Footnotes
-
Competing interests: None.
-
The views expressed here are the authors’ own and do not reflect the position of the National Institutes of Health, the Public Health Service, the Department of Health and Human Services, the University Hospitals of Geneva, the Oltramare Foundation or the Centre Lémanique d’Ethique.
Other content recommended for you
- Should ethics consultants help clinicians face scarcity in their practice?
- Croatian physicians’ and nurses’ experience with ethical issues in clinical practice
- How physicians face ethical difficulties: a qualitative analysis
- Euthanasia and other end of life decisions and care provided in final three months of life: nationwide retrospective study in Belgium
- Extent and determinants of error in doctors' prognoses in terminally ill patients: prospective cohort study
- Combating junior doctors’ “4am logic”: a challenge for medical ethics education
- Withdrawal of ventilation at the patient's request in MND: a retrospective exploration of the ethical and legal issues that have arisen for doctors in the UK
- Limitation of treatment at the end of life: an empirical-ethical analysis regarding the practices of physician members of the German Society for Palliative Medicine
- Late decisions about treatment limitation in patients with cancer: empirical analysis of end-of-life practices in a haematology and oncology unit at a German university hospital
- Role of non-governmental organisations in physician assisted suicide