Article Text

Abstract
Objectives: To explore how subjects in a placebo-controlled vitamin A supplementation trial among Ghanaian women aged 15–45 years perceive the trial and whether they know that not all trial capsules are the same, and to identify factors associated with this knowledge.
Methods: 60 semistructured interviews and 12 focus groups were conducted to explore subjects’ perceptions of the trial. Steps were taken to address areas of low comprehension, including retraining fieldworkers. 1971 trial subjects were randomly selected for a survey measuring their knowledge that not all trial capsules are the same. The subjects’ fieldworkers were also interviewed about their characteristics and trial knowledge. Factors associated with knowledge were explored using multi-level modeling.
Results: Although subjects knew they were taking part in research, most thought they were receiving an active and beneficial medication. Variables associated with knowledge were education and district of residence. Radio broadcasts benefited those with some schooling. Fieldworkers’ characteristics were not associated with subjects’ knowledge.
Conclusions: Research and debate on new or improved consent procedures are urgently required, particularly for subjects with little education.
Statistics from Altmetric.com
Genuine informed consent is considered critical for ethical research.1 2 Most ethical guidelines agree that for informed consent to occur, potential research subjects must make a voluntary choice about participation, based on sufficient knowledge and comprehension of the research design, the risks and benefits of participation, and their rights as participants.3 Despite the prominence of informed consent in ethical debates, guidelines and review procedures, empirical evidence suggests that subjects often have low knowledge of information that could influence their decision to enrol or continue in a study.4–7
Current consent procedures do not always ensure that subjects have sufficient knowledge to make an informed choice about participation, and limitations specific to developing countries have been identified.3 8–10 Procedural problems that hinder understanding, such as complex language and lengthy consent forms, may be exacerbated in populations with poor education or little exposure to research, where local beliefs about health and disease conflict with research theories and concepts or where there are large power differences between the researchers and the participants.3 8 10–13 The cultural context in many developing countries is characterised by a high level of trust in research institutes, a tradition of deferring to others in decision-making and a lack of alternative sources of healthcare.14 15 This context may result in minimal evaluation and processing by subjects of information provided during the process of gaining consent, and consequently in poor knowledge—even though subjects may consider individual consent important. The cultural context may also affect the amount of information provided to subjects by fieldworkers.16 17 For example, if fieldworkers consider consent procedures unnecessary or feel under pressure to limit refusals, they may provide less information than was intended. On the other hand, fieldworkers may enhance subjects’ understanding by modifying difficult wording or providing analogies. Despite the complexity of informed consent, the focus of many ethical review boards is on the research protocol and the content of the consent form, rather than on ensuring that the actual process of gaining consent is appropriate.18
Although several studies in developing countries have documented subjects’ knowledge of trial information,11 12 17 19–22 few have explored factors associated with knowledge of the trial.17 22 This paper reports the findings of a study to measure how subjects in a cluster-randomised placebo-controlled vitamin A supplementation (VAS) trial investigating the impact of VAS on maternal mortality in Ghana perceive the trial, and in particular whether they know that not all the capsules provided in the trial are the same. The study also identifies the factors associated with this knowledge and explores the importance of fieldworkers’ characteristics for understanding of the trial, as this potentially important factor has rarely been examined.
THE VAS TRIAL AND CONSENT PROCEDURE
The VAS ObaapaVitA trial started at the end of 2000 and is planned to end in late 2008. More than 100 000 women aged 15–45 years in the Brong Ahafo region in central Ghana are under active surveillance as part of the trial. Women in the trial have been cluster randomised to take weekly capsules containing 7000 μg of vitamin A in soya bean oil or a placebo containing soya bean oil only and are visited at home every month for capsule delivery and data collection. The VAS trial was preceded by formative research23 to identify concerns and questions that communities had about the planned trial and inform the consent procedure in terms of desired information and appropriate language.
The consent procedure consisted of gaining community consent from traditional leaders at the district and village level, followed by village level community meetings, where senior project staff introduced the aims and methods of the trial and answered questions. In urban areas, community meetings were replaced by radio broadcasts, as meetings often have low attendance in such settings. Individual consent was then sought from all eligible women in the trial area. Fieldworkers trained in communication skills used an information sheet in the local language (Twi) to describe the aim of the trial, the research design, what participation involves, confidentiality and the right to withdraw. Fieldworkers also gave women and others in the household an opportunity to ask questions about the study, which were answered using a “frequently asked questions” book developed from the findings of the formative research. Women were then invited to participate in the trial and asked to confirm their consent with a signature or thumb print.
METHODS
This study consisted of three stages. In stage one, qualitative research was conducted to explore subjects’ perceptions and knowledge of research and the trial. In June 2003, 12 focus groups (of 6–12 women) and 60 semistructured interviews were conducted with randomly selected trial women from 12 villages. The villages were purposively selected to reflect the differences in ethnicity, village size and access to healthcare in the trial area. The interviews were conducted by trained interviewers in Twi, interviewers took field notes during the interviews and the focus groups were tape-recorded. The interviews and focus groups were then converted to detailed English transcripts and were analysed through systematic identification and coding of themes.
In stage two, a number of activities were carried out to address the key areas of low comprehension identified in stage one. These included training of fieldworkers to re-explain the trial to each trial subject during their routine home visits. In addition, eight radio broadcasts and 40 school visits targeting girls eligible for enrolment in the trial were conducted. The aim of these activities was to re-introduce the trial and inform the trial subjects about the placebo and why the trial is being conducted. Placebo was explained as “Half of the women who take ObaapaVitA [the trial name for all of the capsules distributed] receive vitamin A and half receive a capsule which contains no vitamin A. By comparing the results of the women receiving the two different types of ObaapaVitA we can test whether vitamin A improves women’s health.”
In stage three, data on subjects’ knowledge that two types of weekly capsules are provided by the VAS trial and potential explanatory variables were collected. These data were collected by adding questions to a routine VAS trial data-collection instrument monitoring the women’s adherence to VAS. Women for the adherence survey are randomly selected from the VAS trial database using multi-stage sampling (one trial cluster is selected from each of the four trial districts each week and then 10 women are selected from each of the selected clusters). This corresponds to 1971 women being selected for interview from 217 clusters. Of these, 1661 women were successfully interviewed (total non-response rate of 16%, with non-response related to women being temporarily absent from their home despite a return visit for all absent women). The trial knowledge questions were added in January 2004 and the results presented here are based on data collected until December 2004. In December 2004, the 143 fieldworkers of the 1661 women interviewed were contacted and were asked to complete a self-administered fieldworker questionnaire that collected data about their characteristics and their knowledge of the trial.
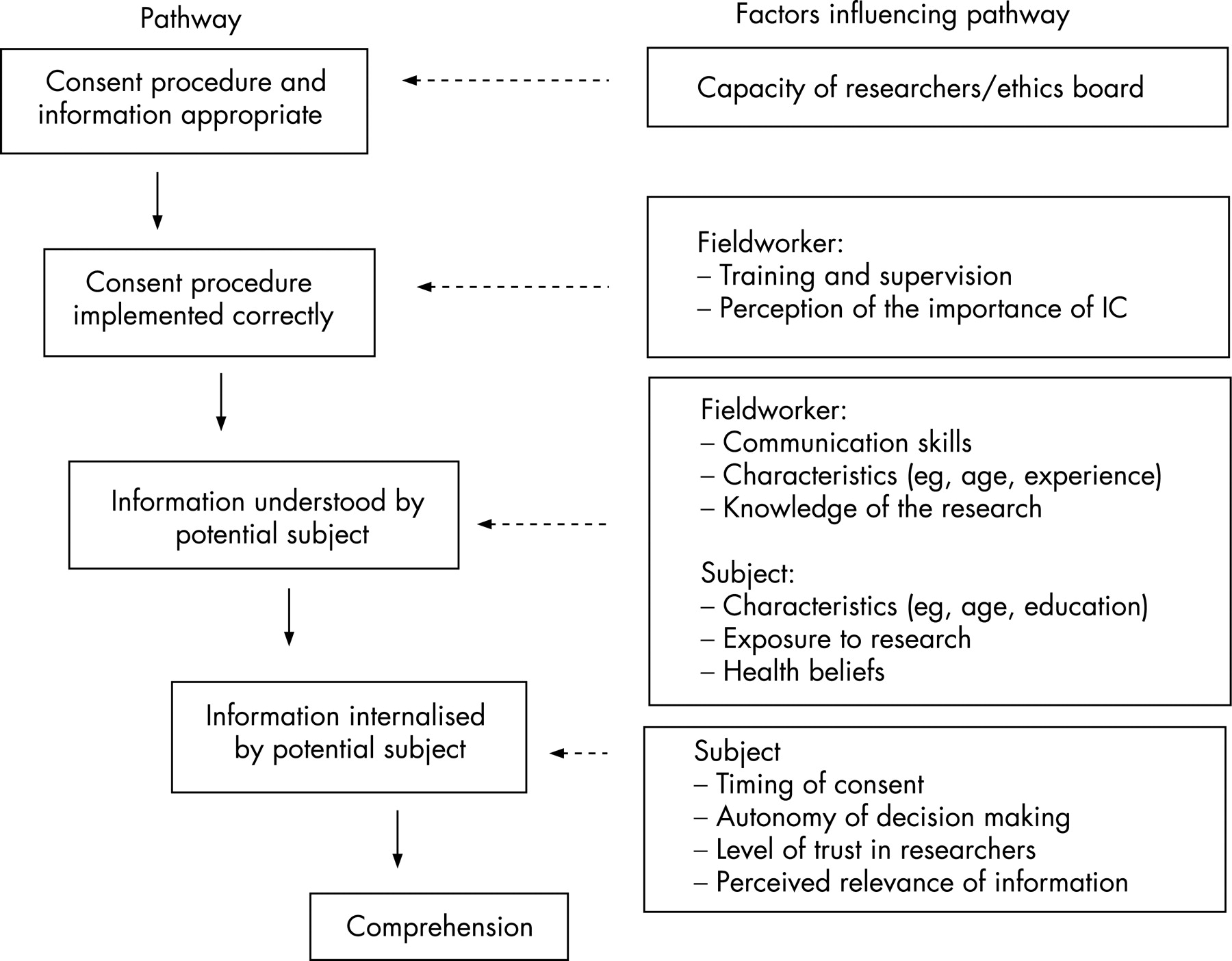
The data for the subjects and the fieldworkers were analysed using Stata 7.0 (Stata Corporation, College Station, Texas, USA). The outcome variable was women’s knowledge that not all capsules in the trial are the same. The explanatory variables were identified from a conceptual framework (fig 1) developed after a review of the literature. It should be noted that in this conceptual framework informed consent is viewed as a process occurring throughout the research rather than a single event that occurs at the start of a participant’s involvement in the research. Similarly, comprehension is viewed as dynamic, because information can be forgotten, reinterpreted or remembered as the research progresses.
{kind=link}
The explanatory variables identified for data collection were subject-related factors (age, education, household assets, place of residence), fieldworker-related factors (age, experience, sex, knowledge of the trial) and trial-related factors (trial district, exposure to radio messages about the trial). Fieldworkers’ education was not included, as all the trial fieldworkers were required to have a secondary education and all had a similar education level. Other factors such as fieldworkers’ communication skills were not measured because of logistical constraints.
Bivariate analysis was conducted for the outcome and each explanatory variable, standardised sample weights were applied, and the standard errors were adjusted for clustering. After checking for collinearity between the explanatory variables, a final, multilevel, population-averaged hierarchical model was fitted using the Xtlogit command in Stata with individuals’ characteristics as level one and fieldworkers’ characteristics as level two. Variables were included in this final model if they had p<0.2 in the bivariate analysis. Hypothesised interactions between the explanatory variables in the final model were then explored. The results presented exclude Nkoranza district, as few women in this district knew that not all the trial capsules were the same (see table 1). The lack of variation in Nkoranza district led to large standard errors and a potentially unstable model, and this district was therefore excluded from the analysis. Excluding Nkoranza district did not change the findings of the final model with regard to the significant variables. In total, 1245 women were included in the analysis.
RESULTS
Perceptions and knowledge of research and the trial
The results from the semistructured interviews show that the majority of women (93%) thought that the trial capsules were a medicine or vitamin. Women described capsules as good for strength, as protective against illness and as ensuring safe delivery. This finding was confirmed in the focus groups: “Ghanaian women suffer during pregnancy and delivery and ObaapaVitA will help reduce these health problems.” Thirteen per cent of the women in the semistructured interviews reported that not all the trial capsules were the same. This poor knowledge about placebo was also confirmed in the focus groups, where differences in capsules were rarely mentioned and a belief that all the trial capsules contain vitamin A was common: “ObaapaVitA is vitamin A which comes from things like paw paw, banana and oranges.” The focus groups also identified a small group of women who knew nothing at all about the trial or the capsules: “I am taking the medicine but I don’t know what it is.”
Most women in the focus groups and the semistructured interviews had good knowledge of trial eligibility criteria, of how to take the trial capsule, of vitamin A and its functions and of the length of the study.
Seventy five per cent of women in the semistructured interviews reported that they knew they were taking part in research, but the findings of the focus groups suggest that women interpret “research” in several ways. While the trial’s aim of testing the effectiveness of the capsules emerged in all the focus groups (“You want to find out if the medicine will help women or not”), other common interpretations of research included finding out if women are taking the capsules, whether the capsules have side effects and whether distribution can be extended to the rest of the country, and monitoring how well the fieldworkers are doing their job. Women most frequently described research as “the way you find out the truth about something … like an investigation for a murder case”. Several women reported that the reason they knew they were part of research was because the fieldworkers were always coming to ask them questions.
Factors associated with trial knowledge
The weighted distribution of the explanatory variables are presented in table 2, along with the distribution of the outcome variable by each category of the explanatory variables. Sixty-nine per cent of the sample were rural, 68% were under 35 years of age, and the majority had no or only primary education (52%), were classified as having low or medium household assets (60%) and were Akan (52%). In total, 45% of participants (38% if Nkoranza district is included) knew that not all the capsules in the VAS trial were the same. Knowledge of other aspects of the trial was high (how to take the capsules and who can take them), with 85% of women being classed as having high knowledge based on answering correctly at least 14 out of 15 questions about the capsules and how to take them.
Table 2 also shows the bivariate analysis and the adjusted odds ratios for each explanatory variable. In the bivariate analysis, subjects’ education, household assets, ethnicity, district, exposure to radio messages about the trial and fieldworker experience were all significantly and positively associated with knowledge that not all capsules in the VAS trial are the same (p<0.05). Place of residence was not significantly associated with knowledge but was eligible for inclusion in the final model (p<0.02).
In the multilevel analysis, only education level and district of residence remained significantly associated with knowledge about the capsules. Women in Wenchi and Techiman districts were three to four times more likely than women from Kintampo to know that not all capsules in the VAS trial were the same, and women with primary education were 1.5 times and those with secondary or higher education 2 times more likely than women with no education to know that the capsules were different. Hypothesised interactions were explored in the final model and a significant interaction between exposure to trial radio messages and education level was found. Hearing radio broadcasts benefited knowledge about the capsules only among those with some education (odds ratio 1.9; confidence interval 1.22–2.90).
DISCUSSION
The data from the semistructured interviews and focus groups suggest that most women in the trial (75%) knew that they were taking part in research but that their interpretations of the trial varied. Many women believed they were receiving an active medication that provided benefits such as strength, reduction of illness, and safe delivery. Only 13% knew that not all the trial capsules were the same, despite a lengthy consent procedure. Knowledge of how the capsules differ is likely to be even lower.
Other studies in developing countries have also found that subjects have low trial knowledge: in Gambia only 10% of participants understood the placebo-controlled design in a vaccine trial,11 and in Uganda only 19% of mothers knew that not all of the treatments in a malaria trial were the same.17 In Haiti only 20% of participants passed an assessment of their trial knowledge, which included whether they knew the purpose of the study, the risks and benefits of participation and that participation was voluntary.12 In Bangladesh only 48% of respondents knew they were free to withdraw after giving consent.20 Three South African studies also found low knowledge: in one, 28% of participants knew the study’s aim,21 in the second, 88% of women in a trial felt participation was compulsory;19 and in the third, only 21% of participants understood randomisation and 19% understood placebo.22 Low levels of knowledge have also been reported in developed countries, with a cross-sectional survey of patients in three cancer trials in America finding that only 26% of participants knew their treatment was not standard.7
Although the results from the semistructured interviews and focus groups suggest that many women believed they were receiving an active and beneficial medicine, knowledge of other trial information was high (eg, who can take the capsules, how to take the capsules and what to do if capsules were missed), suggesting that widespread dissemination of trial information is possible. This information was provided in a different manner from the placebo information—namely, in small segments over multiple visits and on an ongoing basis. This contrasts with the procedure for gaining consent, in which a large quantity of information was provided in a single visit. The possibility of providing information for informed consent in small segments and over multiple visits should be explored. The high knowledge of other trial information may also be related to the salience of the information, in that the information for which participants had high knowledge was identified by respondents in the formative research as important.23 Informed consent cannot be thought of only in terms of whether participants understand the information provided or not. Whether the information is relevant to their lives or is important to them should also be considered.
There is no consensus regarding the level of understanding required for research to be ethical or whether understanding is important throughout a trial or only at the time of consent. Some argue that only minimal understanding may be required, as the costs and benefits of participation have already been considered in the ethical review process24 or because subjects may not want to base their decision to participate or continue in a trial on all the information provided.25 During the formative research for the VAS trial, women expressed a desire for detailed information about the study,23 and we took the view that knowledge is important not just for deciding whether to enrol but also whether to continue in a trial. We therefore considered that the low knowledge discovered in the qualitative research warranted re-education activities.
Data from this study suggest that the re-education activities improved knowledge: the percentage of women who knew that not all the trial capsules were the same increased from 13% (as measured in the semistructured interviews) to 38% (as measured in the quantitative survey in all districts). This apparent difference must be interpreted with caution, as the sampling frames for the two surveys were not the same. In addition, the time interval between the consent procedure and data collection for the semistructured interviews was 2 years, whereas the data for the quantitative survey were collected within 12 months of the re-training activities. No evidence of recall bias was found, in that there was no association between time of interview and knowledge that not all the trial capsules were the same in the structured survey conducted after the re-education activities.
The analysis of the predictors of women’s knowledge of whether all the trial capsules are the same found that after adjustment for covariates, having attended school and district of residence were significantly associated with subjects’ knowledge of whether all capsules in the trial were the same. Education is one of the factors most consistently associated with trial knowledge,26 and current consent procedures appear to be inadequate for ensuring comprehension among less-well-educated subjects. Repeating current consent messages through different media is not enough, as we found exposure to messages through radio broadcasts benefited only subjects who had some education. Focusing on women with low education in the design of the consent procedure and the consent form and extensively pre-testing the consent procedure with this group may help develop procedures that are more appropriate.
Site differences in trial knowledge have been found in studies in other developing countries17 and are difficult to explain. In our study it is possible that there are unmeasured factors that account for the observed district differences, such as subject mobility. The capital of Techiman district, has a large market, which attracts people from all over the district and may result in residents being more mobile and thus more exposed to new concepts and ideas and more questioning about the research. Another possible explanation is that consent procedures and re-education activities were not implemented uniformly across districts. Exposure to previous research studies does not appear to explain district differences and does not appear to facilitate trial knowledge. Kintampo district (where comprehension was lowest) has been the site of community-based research for the past 10 years and most villages in the district have taken part in one or more research studies. A high level of interaction with research institutes has been found to result in a high level of trust14 15 and this trust may have resulted in women in Kintampo assuming the trial was beneficial and thus not evaluating or processing the information provided during consent or re-education.
None of the characteristics of the fieldworkers (age, sex, experience, knowledge that not all the trial capsules were the same) were associated with subjects’ knowledge that not all the trial capsules are the same. Potentially important characteristics of fieldworkers, however, such as their communication skills and whether they omitted information during consent, were not measured, because of logistical constraints. Studies are needed that focus on fieldworkers’ communication skills, as well as qualitative studies exploring fieldworkers’ views of consent and the role they are asked to fulfil.
Despite extensive training and provision of fieldwork manuals, 17% of the fieldworkers did not understand the concept of placebo and thought that all the trial capsules were the same. Fieldworkers’ knowledge of consent information needs to be increased and should be assessed as part of the post-fieldworker-training assessment currently used to aid in fieldworker selection for the VAS trial.
If the low level of subjects’ knowledge about placebo found in this and other developed and developing country studies is to be improved, changes in consent procedures and review processes are required. There have been many suggestions as to how to improve consent, such as building the capacity of local ethics boards, improving ethical guidelines, adapting consent forms and processes to local contexts, developing tools and metaphors to explain complex concepts, providing information in small portions and over multiple visits, using visual aids, improving fieldworkers’ communication skills, checking subjects’ understanding and allocating sufficient resources and training for the process of gaining informed consent.8 14 15 18 20 25 27 There is, however, little evidence for what is actually effective to improve knowledge, and an evidence base on how to ensure that informed consent is truly informed in developing countries is urgently needed. A recent review of interventions in developed countries found that extended discussion and interaction during the consent procedure showed the most promise for improving knowledge. Multi-media interventions rarely had an effect on knowledge, and evaluations of interventions that improved consent forms or tested subjects’ knowledge of key information were methodologically flawed.26 Despite debate on the appropriateness of current procedures for developing countries,12 21 28–30 only one intervention study in a developing country was located. This small-scale study, in Haiti, improved subjects’ knowledge though multiple meetings with consent counsellors and the use of visual aids.12 Research and debate on new or improved strategies for information delivery are urgently needed. Review boards also play an important role in ensuing that consent procedures are appropriate. Review boards in both developed and developing countries must ensure that their requirements do not result in complex and lengthy consent forms and need to focus more on process as well as content.
In summary, despite all the care in undertaking formative research, designing comprehensive consent procedures and training fieldworkers, only 13% of women knew that not all the trial capsules were the same 24 months after giving consent. Even after re-education, knowledge among those with no education was low. This raises questions about how informed consent should be approached. Potential reasons for the low level of knowledge was the salience or relevance of the information to the participants’ lives, the provision of a large quantity of information at once, the appropriateness of the consent procedure for women with low education and issues of trust between the community and the research centre. Qualitative research is needed to explore these reasons in depth and to collect recommendations from participants on ways to enhance their understanding of research. This research needs to be followed by intervention research to add to the limited evidence base on how to improve informed consent.
Acknowledgments
The authors would like to thank Dr Janet Rice, Professor Carl Kendall and Dr Thom Eisle for their help and guidance. We would also like to thank all the staff of the Kintampo Health Research Centre and all the community members who participated for their support during this research. This study was supported by the UK Department for International Development.
REFERENCES
Footnotes
Competing interests: None declared.
Other content recommended for you
- Understanding the language barriers to translating informed consent documents for maternal health trials in Zambia: a qualitative study
- Education versus screening: the use of capacity to consent tools in psychiatric genomics
- Making research ethics work for global health: towards a more agile and collaborative approach
- Discussing surgical innovation with patients: a qualitative study of surgeons’ and governance representatives’ views
- Double blind, cluster randomised trial of low dose supplementation with vitamin A or βcarotene on mortality related to pregnancy in Nepal
- Achieving new levels of recall in consent to research by combining remedial and motivational techniques
- Thrombolysis for acute ischaemic stroke: consumer involvement in design of new randomised controlled trial
- Building on relationships of trust in biobank research
- Randomised, double blind, placebo controlled clinical trial of efficacy of vitamin A treatment in non-measles childhood pneumonia
- Informing children and parents about research