Article Text

Abstract
Aim or objective To examine the effectiveness of concussion prevention strategies in reducing concussion risk in sport.
Design Systematic review according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines.
Data sources Eleven electronic databases searched and hand-search of references from selected studies.
Eligibility criteria for selecting studies The following were the study inclusion criteria: (1) contained original human research data; (2) investigated an outcome of concussion or head impact; (3) evaluated a concussion prevention intervention; (4) included sport participants; (5) analytical study designand (6) peer-reviewed. The following were the exclusion criteria: (1) review articles, case series or case studies and (2) not in English.
Results The studies selected (n=48) provided evidence related to protective gear (helmets, headgear, mouthguards) (n=25), policy and rule changes (n=13) and other interventions (training, education, facilities) (n=10). Meta-analyses demonstrate a combined effect of a 70% reduction (incidence rate ratio (IRR)=0.3 (95% CI: 0.22 to 0.41)) in concussion risk in youth ice hockey leagues where policy disallows body checking, and the point estimate (IRR=0.8 (95% CI: 0.6 to 1.1)) suggests a protective effect of mouthguards in contact and collision sport (basketball, ice hockey, rugby).
Summary/conclusions Highlights include a protective effect of helmets in skiing/snowboarding and the effectiveness of policy eliminating body checking in youth ice hockey. Future research should examine mouthguards in contact sport, football helmet padding, helmet fit in collision sport, policy limiting contact practice in youth football, rule enforcement to reduce head contact in ice hockey and soccer, ice surface size and board/glass flexibility in ice hockey and training strategies targeting intrinsic risk factors (eg, visual training).
Systematic review registration PROSPERO 2016:CRD42016039162
- concussion
- prevention
- sport Injury
Statistics from Altmetric.com
What is already known about this subject?
The burden of concussion in youth, amateur and professional sport is high.
Primary prevention strategies in sport can reduce the burden of injury; however, there are limited rigorous cohort and randomised controlled trails evaluating concussion prevention strategies in sport.
What are the new findings?
Helmets in skiing/snowboarding reduce the risk of traumatic brain injury, including concussion.
Policy that eliminates body checking in youth ice hockey leads to a 67% reduced risk of concussion in 11-year-old and 12-year-old hockey players.
There is evidence to support future research examining mouthguards in contact sport where meta-analysis suggests that there may be a 19% reduced risk of concussion (although not statistically significant) when combining evidence from basketball, ice hockey and rugby.
Introduction
The Consensus Statement on Concussion in Sport (Fourth International Conference on Concussion) defined concussion as ‘a subset of mild traumatic brain injury (mTBI) which is a complex pathophysiological process affecting the brain, induced by biomechanical forces’.1 Biomechanical forces may include a direct impact to the head, neck or face, or an impact to another part the body with a mechanical force transmitted to the head.1 Signs and symptoms of concussion (eg, headache, dizziness, neck pain, nausea, confusion, irritability, sleep disturbance) are believed to be the results from altered brain function, and they do not indicate structural damage to the brain.1 Despite the widespread adoption of the Consensus concussion group definition,2 definition and terms remain controversial.
More than 160 000 Canadians experience an acquired brain injury annually, with mTBI accounting for the largest proportion of traumatic brain injuries (TBIs).3 Statistics Canada reported that in 1 year, 94 000 Canadians aged 12 and over experienced an ‘activity limiting concussion’.4 Annually, over 700 000 youth ages 0–19 seek hospital-based medical care for TBI in the United States, and 80%–90% of these injuries are mTBI.5 The leading cause of concussion in young adults and youth is sport, resulting in a significant public health burden.4
The risk of concussion is highest in individuals participating in collision sport, particularly in youth rugby, ice hockey and American football (concussion rates ranging from 0.5 to 4.2 concussions per 1000 athlete exposures), affecting more than 10% of players in one season.6–9 Other risk factors for sport-related concussion include previous concussion history, competition (vs training), rules of the game (eg, body checking in youth ice hockey), age, sex and level of play.10
Concussion is among the most common injury type in youth sport, accounting for over 15% of the overall injury burden.11 12 Concussion may reduce future participation in physical activity, adversely affecting future health, and may also lead to post-concussion syndrome, reduced participation in physical activity and overweight/obesity.13–16 Reduction of concussion risk would have a major impact on quality of life. A logical approach to reducing this burden is primary prevention and rigorous scientific evaluation is key to informing best practice and policy in injury prevention.17 18
While it is impossible to eliminate all concussion in sport, concussion prevention strategies can reduce the number and severity of concussions in many sports. Until the past decade, there has been a relative paucity of scientifically rigorous evaluation studies examining the efficacy of concussion prevention strategies in sport, particularly youth sport.19 20 Historically, epidemiological research focused on the evaluation of concussion prevention strategies in elite adult athlete populations where injury surveillance practice is established more commonly, including medical staff within the sport structure.19 20 As a result, previous recommendations for concussion prevention practice in youth sport have relied heavily on studies on adult elite sport populations.19 20
Our primary objective was to examine the effectiveness of concussion prevention strategies in reducing concussion risk in sport. We systematically reviewed the extrinsic and intrinsic concussion prevention strategies in sport and assessed the effectiveness of prevention strategies for reducing head impacts in sport.
Methods
Data sources and search strategy
This review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines.21 The protocol for this systematic review was registered on PROSPERO and can be accessed at http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016039162
Relevant studies were identified through 11 electronic databases:
Ovid MEDLINE (R) In-Process & Other Non-Indexed Citations (1946 to present)
CINAHL (1982 to present)
PsycINFO (1967 to present)
Cochrane Databases for Systematic and Complete Review (1975 to present)
Cochrane Controlled Trials Registry (1975 to present)
Cochrane Injuries Group Trials Register
SPORTDiscus (1980 to present)
EMBASE (1974 to present)
ERIC (1966 to present)
Conference Proceedings Citation Index (via Web of Science)
ProQuest Dissertation & Theses Global Database
A search involving a combination of medical subject headings, keywords and related synonyms in three main concepts was performed in May 2016 and updated in September 2016. Databases were searched for terms related to: (1) mTBI or concussion or head impact AND (2) prevention strategy (eg, policy, equipment, neck strengthening) AND (3) sport. For the MEDLINE search used, see online supplementary material. Duplicates were removed and then study titles and abstracts were reviewed to identify potentially relevant studies (AMB, AK, CAE, GM). If a study title of interest was found but no abstract available, the full article was retrieved to ensure that no relevant studies would be missed. Reference lists of selected studies were also hand-searched to identify relevant articles not found by the search strategies. Only peer-reviewed literature (manuscripts and published abstracts) and dissertations (if relevant details were not available in manuscript or abstract) were included in this search.
Selection of studies
The titles and abstracts of returned records from each search strategy, after accounting for duplication, were reviewed by two of four reviewers to identify potentially relevant studies (AMB, AK, CAE, GM). The full text of all potentially relevant studies was then independently reviewed by two authors to determine final study selection (AMB, AK, CAE, GM). The following were the study inclusion criteria: (1) contained original data human research studies only (full-text paper or abstract published); (2) investigated an outcome of concussion or head impacts; (3) evaluated a concussion prevention intervention (eg, rules and regulations, protective equipment, education, training); (4) included sport participants (eg, male and/or female, all ages, all levels of performance); (5) analytical study design (including randomised controlled trial (RCT), quasi-experimental, cohort (prospective or historical), case-control, cross-sectional, pre-experimental, ecological) and (6) peer-reviewed. The following were the exclusion criteria: (1) review articles, case series or case studies and (2) not written in English.
Data extraction and risk of bias assessment
Data extracted from each study included authors, study design, study duration, country, participants (ie, sport, level, sex, age and sample size for intervention and control groups), concussion definition, intervention and control description, concussion incidence rate or incidence proportion reported for each of the intervention and control groups, and effect estimate (ie, incidence rate ratio (IRR), risk ratio, OR). Effect estimates are reported based on describing a protective effect. Data were extracted by two authors and consensus was made on final extraction by four authors (AMB, AK, CAE, GM).
Two authors (AMB, AK, CAE, GM, KJ, LE, JK, DM, CT) independently assessed the risk of bias for each study based on the Downs and Black (DB) checklist for methodological quality.22 This checklist comprises 27 criteria (maximum score of 33 points) assessing study reporting, external validity, internal validity (eg, bias and confounding) and power. Discrepancies in DB scoring were resolved by consensus between two authors and if required a third author was consulted to obtain consensus. The level of evidence represented by each study was categorised by consensus of two authors (CAE, AMB) based on the Oxford Centre of Evidence Based Medicine 2009 model.23
Data synthesis and meta-analyses
We synthesised data qualitatively based on the categories of injury prevention intervention established following data extraction. If an effect estimate was not provided, risk ratios were calculated if the data (number of concussions by study group and number of individuals and/or exposure totals in each study group) were available. Meta-analyses were conducted using the R project software for statistical computing (package ‘metaphor’) based on available outcomes and homogeneity where combined estimates of effect measure were produced using IRR based on a random effects model for studies examining overall concussion outcomes in sport. Two more known and important measures of heterogeneity, I2 and Q (the latter with its associated p-value), were also examined.
Results
The initial search yielded 13 008 studies (figure 1). After removal of duplicates and studies not meeting inclusion criteria, this was narrowed to 74 (AMB, AK, CAE, GM). Updating the search strategy yielded three additional references for full-text review. Further, 29 were excluded based on manuscript evaluation by two independent reviewers (AMB, AK, CE, GM). In total, 48 studies were identified and categorised by prevention strategy and sport (figure 1 and table 1; see online supplementary tables 1 and 2).24–71 The majority of studies evaluated protective equipment (n=25) or rules and regulations (n=13), and the remainder examined other concussion prevention strategies (eg, training, education, facilities) (n=10). In total, only 5 of 48 (10.4%) studies are RCTs, with the remaining being cohort (n=20, 41.7%), historical cohort (n=12, 25.0%), case-control (n=3, 6.3%), cross-sectional (n=5, 10.4%), pre-experimental (n=2, 4.2%) and ecological (n=1, 2.1%) studies. The sports included are ice hockey (n=19, 39.6%), American football (n=15, 31.3%), rugby (n=7, 14.6%), soccer (n=3, 6.3%), basketball (n=1, 2.1%), skiing/snowboarding (n=1, 2.1%) and multi-sport (n=2, 4.2%). One study (2.1%) included female sport participants only,38 41 (85.4%) included male sport participants only and 6 (12.5%) included both. Youth sport participants were targeted in 26 of 48 (54.2%) studies.
Search strategy and results of the systematic literature search, with total number of unique articles per database
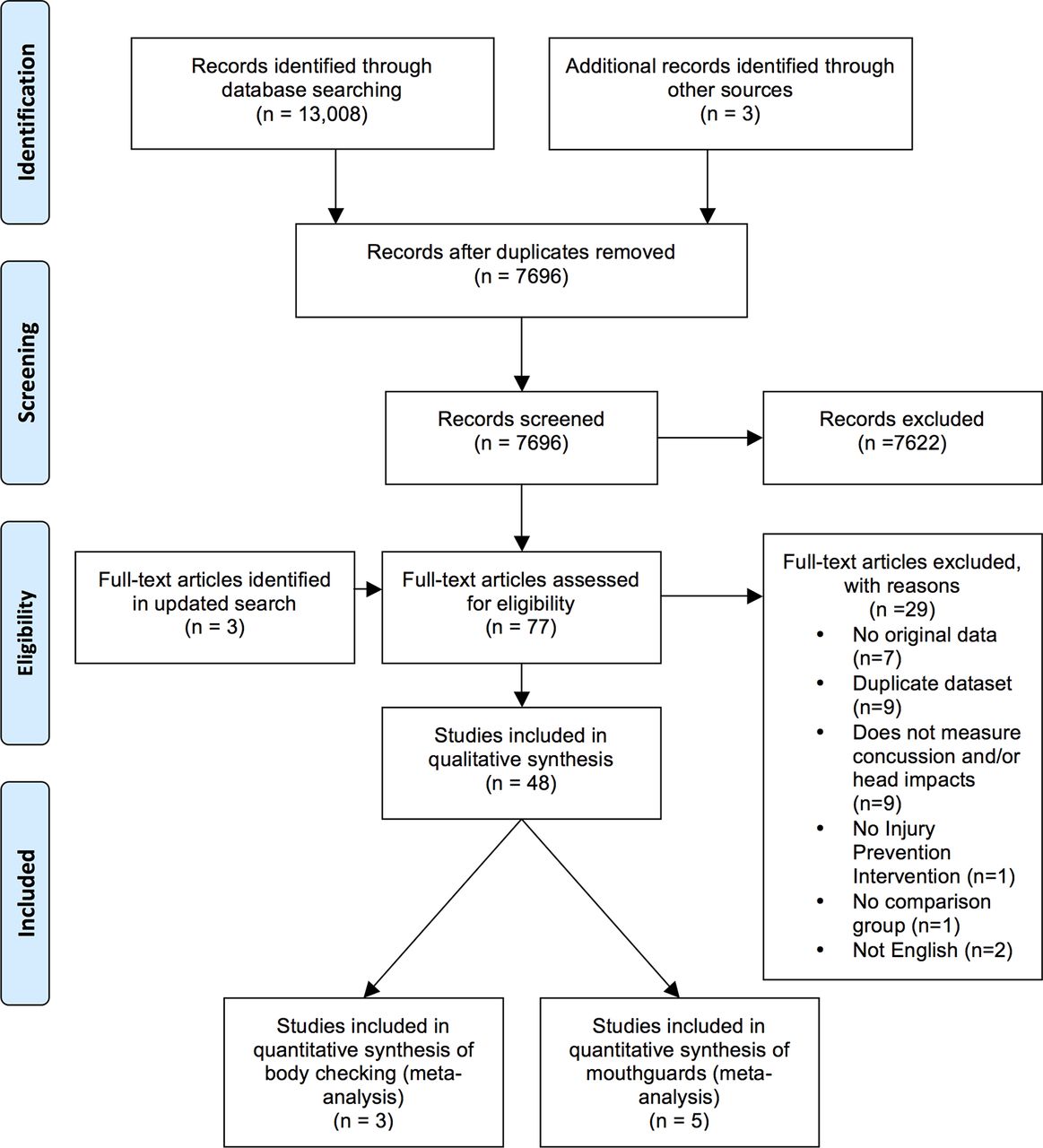
Study identification PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Risk of bias assessment
The median assessment of risk of bias for all 48 studies, based on the DB checklist, was 14.5/33 (range: 6–24). The median methodological quality for the five RCTs was 15/33 (range: 11–24). Common limitations included the lack of reporting of adverse events, incomplete description of how the participating sample was representative of the population of interest, limited description of the characteristics of those lost to follow-up, inadequate sample size or lack of reporting of a-priori sample size, and lack of adjustment for potential confounding.
Meta-analyses conducted based on available outcomes of cohort studies to produce combined estimates of measure of effect using IRR for five studies examining mouthguards in reducing the risk of concussion in sport and for three studies examining policy eliminating body checking in youth ice hockey are summarised in figures 2 and 3, respectively. Missing data from one abstract evaluating mouthguards were supplemented by data available in the published dissertation.72 The size of the box in these figures represents the relative weights given to each study in calculating the overall summary measure. The weights depend on the standard errors of the IRR. The combined estimate for studies examining the preventative effect of wearing a mouthguard in collision or contact sport (eg, basketball, rugby, ice hockey) suggests a protective effect (based on the point estimate and the proximity of the right confidence limit to 1) in reducing the risk of concussion by 19%, but this finding is not statistically significant (IRR=0.81 (95% CI: 0.6 to 1.1) I2=0.00%, Q(4df)=2.7985, with associated p=0.5921). The combined estimate for cohort studies demonstrate a preventative effect in reducing the risk of concussion by 67% when body checking is eliminated in youth ice hockey (IRR=0.33 (95% CI: 0.25 to 0.45), I2=0.12%, Q(2df)=1.50693, with associated p=0.47073) (figure 2).

Forest plot based on meta-analysis evaluating mouthguard use compared with no mouthguards. IRR, incidence rate ratio.

{kind=link}
{kind=link}
{kind=link}
Forest plot based on meta-analysis evaluating body checking policy change in youth ice hockey. IRR, incidence rate ratios.
Protective equipment: helmets
Of the 48 studies identified in the review, 9 examined the effectiveness of helmets, helmet fit or helmets with face protection for concussion prevention.24–32 A physician, therapist or ski patrol medically identified the outcome measures, including concussion in all studies. Protective effects of wearing a helmet when compared with not wearing helmet were observed in one study in skiing/snowboarding32 and one comparing collegiate football (helmets worn) with rugby29 (helmets not worn). There is some evidence supporting the importance of appropriate helmet fit in youth football,26 with reduced symptom severity and duration reported with proper helmet fit. The use of full compared with half face shields in collegiate ice hockey did not reduce the risk of concussion and there was no risk compensation found (eg, increased risk of non-head injury in players with full face shields that might be expected if players increase their ‘risky’ on-ice behaviour when the ‘protection’ is greater).1 30
Three of the four studies examining helmet type in football suggest that different helmet types may influence concussion risk. Collins et al 25 reported a 40% reduction in concussion risk when a helmet with thicker padding over zygoma and mandible area was compared with standard helmets, and Rowson et al 28 reported a 54% reduction when the same helmet was compared with a standard helmet. Conversely, a later study by Collins et al 24 reported a higher proportion of concussed players who wore the helmet with thicker padding relative to players wearing other brands. It should be noted, however, that this study relied on proportions and did not estimate concussion incidence rates for each helmet type. Greenhill et al 26 did not find a difference in concussion risk when comparing three helmet brands.
Protective equipment: headgear
Seven studies were identified in sports where helmets are not worn that examined another form of headgear in rugby and soccer and the evidence is inconsistent.33–39 Hollis et al 33 (IRR=0.57) and Kemp et al 34 (IRR=0.43) reported a significant protective effect of headgear in professional rugby players. The remaining three rugby studies demonstrated no effect of headgear on concussion risk.35–37 In soccer, Delaney et al 39 demonstrated a protective effect of headgear in youth soccer (RR=0.38), consistent with Achar et al 38 in collegiate soccer (RR=0.42); however, this finding was not statistically significant.
Protective equipment: mouthguards
The protective effect of wearing a mouthguard in comparison with no mouthguard was examined in eight studies (basketball,1 hockey3 and rugby4) with mixed findings.33 34 37 40–43 48 Six of the eight studies suggest a protective effect on concussion risk33 34 40–42 48 across three sports; however, none of these findings were statistically significant. Five other studies27 44–47 comparing a custom mouthguard with a standard mouthguard primarily in football players failed to demonstrate a protective effect, with the exception of Singh et al 44 and Winters and DeMont45 where a reduced risk of concussion is reported in high school football players wearing a custom mouthguard. Based on combining five studies (basketball, ice hockey, rugby) that provided data to consider IRRs, the point estimate (IRR=0.8 (95% CI: 0.6 to 1.1)) suggests a protective effect of mouthguards in contact sports (figure 2).
Policy and rule changes
Twelve studies examined the effectiveness of policy or rule changes in reducing the risk of concussion.49–53 The majority of these studies7 examined the protective effect of disallowing body checking in youth ice hockey, demonstrating an overall effectiveness (20%–90% reduced concussion risk where policy disallowed body checking),50 51 in all but two studies that were based on hospital injury surveillance outcomes alone.57 58 A meta-analysis including only cohort studies that used individual-level exposure data and validated team-based injury surveillance methodology demonstrates a combined unadjusted effect of a 67% reduction (IRR=0.33 (95% CI: 0.25 to 0.45)) in concussion risk in leagues where policy disallows body checking53 54 (figure 3). Two studies examined the effect of zero tolerance to the head contact rule change52 56 with conflicting results. In the NHL, a reduction in concussion risk of 36% was observed following a rule change instituting greater enforcement of head contact penalties.52 In youth ice hockey, however, a protective effect was not found.56 One study examined stricter enforcement of red cards in soccer for high elbows in heading duels, demonstrating a 19% reduced risk of concussion.49 In professional football, Ruestow et al 61 examined the effect of the free kick rule change on concussion risk with inconclusive results. High school football policy restricting to no more than two collision practices a week led to a 42% reduction in head contacts in games and a 53% reduction of head contacts in practices.59 In youth football (ages 9–12), limiting contact practice to no more than one of three weekly practices (≤40 min) may have led to a reduced frequency of head impacts.60
Other strategies to reduce concussion risk
Clark et al 62 demonstrate an 85% reduction in concussion risk in collegiate football in an RCT examining the effectiveness of vision training preseason. Kerr et al 64 examined the combined effectiveness of a Heads Up First Education Program and limiting contact in practices in youth football and found no protective effect in reducing concussion risk combined or individually in games or practices. However, in a later study, Kerr et al 63 demonstrate a protective effect of introducing a player safety coach in reducing the risk of concussion in practices. Tackle training without helmets and shoulder pads in youth football did not lead to a reduction in head impacts in games.65 Following technical training in professional rugby, the overall technical proficiency did not differ in injurious compared with non-injurious tackles on video analysis; however, proficiency scores for head and shoulder placement were higher in non-injurious tackles.66
Fair play rules (where teams get additional tournament points for low penalty minutes) have been evaluated in youth ice hockey. Roberts et al 67 and Smith et al 68 demonstrated no difference in concussion risk with or without fair play rules in tournament play. However, Smith et al 68 demonstrated fewer non-injurious head contacts with ‘intensified’ fair play compared with ‘non-intensified’ fair play rules.
In elite levels of ice hockey, there is evidence to support a lower incidence of head contacts in games played on a large international ice surface (204 feet long × 100 feet wide) compared with a smaller standard North American rink ice surface (200 feet long × 85 feet wide) or intermediate size surface (94 feet wide).70 71 Furthermore, a 57% reduction in concussion risk (IRR=0.43, 95% CI: 0.18 to 1.01) was reported when player game exposure was in rinks with flexible boards and glass compared with traditional boards and glass, but this difference was not significant.69
Discussion
Protective equipment
Helmets contribute to preventing focal head injuries in sport, but their effectiveness in preventing concussions is less clear. This review identified two studies demonstrating a protective effect of helmet use in skiing/snowboarding and in a comparison between football and rugby.29 32 This evidence is limited based on a lack of distinction of concussion in skiing/snowboarding within the injury definition including all head injuries.32 In the other study, a comparison was made between two different sports without consideration of other important covariables (eg, rules of the game, previous concussion history) that may have influenced these findings.
Further research evaluating the effectiveness of helmets in team collision sports (eg, ice hockey) is difficult as a control condition is not ethical where helmet use policy is in place. Three systematic reviews73–75 support the effectiveness of helmets in skiing and snowboarding in reducing the risk of head injuries in adults and youth. In the studies including children, the associated OR was 0.41 (95% CI: 0.27 to 0.59).73 These studies include all head injury and not specifically concussion risk.
There is cohort study evidence that thicker padding over the zygoma and mandible area may contribute to a reduced risk of concussion in American football.25 28 Ensuring appropriate helmet fit is also supported as a strategy to reduce concussion symptom severity and duration in youth football.26 Further biomechanical studies with appropriate controls are needed to support rigorous helmet standards for manufacturing and establishing appropriate sport-specific helmet fit criteria.
Whether headgear protected against concussion in rugby is unclear.33–36 Based on two cross-sectional studies, the evidence is more consistent for headgear to protect against concussion in soccer.38 39 However, further evidence based on a more rigorous study design is required as these findings may have been influenced by biases inherent to cross-sectional studies (eg, selection bias) and lack of control for potentially confounding variables. No studies in boxing met the inclusion criteria; however, the use of headgear in boxing remains controversial and gained much media attention in 2016. No effect of headguards on concussion was reported in Olympic boxing, which led to the removal of head guards in male boxing prior to the 2016 Rio Olympics.76
Studies examining the protective effect of mouthguards in reducing the risk of concussion in basketball, hockey and rugby suggest a protective effect.33 34 40–42 48 Mouthguards have consistently decreased the risk of orofacial injury across numerous adult sports (eg, ice hockey, rugby, basketball, football), with a pooled 86% increased risk in non-users through meta-analysis.77 Studies examining mouthguards specifically related to the prevention of concussion were limited by study design, small sample size, lack of control for confounding and self-report measurement bias.
Meta-analysis combining studies suggest a protective effect of mouthguard use (based on the point estimate and the proximity of the right confidence limit to 1) in collision sport (IRR=0.81 (95% CI: 0.6 to 1.1)), but this finding was not statistically significant. Although it may not be ethical in some collision sports where mouthguard use is mandated to do an RCT, it may be possible to consider case-control approaches to evaluate risk with consideration of potential confounding and more rigorous injury surveillance methodologies.
Policy and rule changes
Body checking policy in youth ice hockey was considered in seven of the twelve studies examining the effectiveness of rule changes50 51 53–55 57 58 in reducing the risk of concussion. A previous meta-analysis reported a combined effect estimate suggesting a protective effect in reducing the risk of concussion (OR=0.58 (95% CI: 0.41 to 0.83)), including studies that did not consider validated injury surveillance, individual level participation exposure data, control for clustering by team and confounding variables.78
In our meta-analysis, only cohort studies using validated injury surveillance methodology and individual-level participation exposure data were included in the combined estimate, which demonstrates a 67% reduction in concussion risk in players ages 11–12. Further consideration of body checking policy in older age groups and various levels of play will inform policy change in leagues where players are 13 years and older. Video analysis to examine injury mechanisms and player performance associated with such policy change is important to inform governing bodies regarding the effects of policy change on contact mechanisms and performance.
In contrast, a rule change that was not evidence-informed was the zero tolerance for head contact enforcement. This rule change reduced the risk of concussion in professional ice hockey,52 but no protective effect was reported in youth ice hockey.56 This inconsistency may be related to differences across leagues in concussion referral patterns, referee behaviours and injury surveillance methodologies. During the period of the youth hockey cohort study, increased media attention and awareness of concussion may have informed a greater identification of concussions after this rule change.56 In professional soccer, a similar rule change where stricter enforcement of red cards for high elbows in heading also led to a reduced risk of concussion.49
In youth football (high school age and ages 9–12), limiting contact practice led to a reduced frequency of head impacts in younger players.60 The translation of reduced head impacts to concussion risk reduction requires further investigation.
Other strategies to reduce concussion risk
Fair Play programs that reward teams for not committing fouls reduce the number and severity of penalties in youth ice hockey.67 79–82 However, two studies examined the effect of fair play on injuries, and the ability to detect the effects of this intervention on concussion was limited due to sample size.67 68
There is little evidence to support education programs alone as a strategy to reduce concussion risk in youth collision sport. However, educational strategies may increase concussion identification and management knowledge in players, parents and coaches.83 84 Thus, such strategies may be beneficial in the secondary prevention of subsequent concussions and consequences of concussion (eg, post-concussion syndrome), but this has not yet been examined. The combination of coach education and reducing collision drills in practice in youth football may reduce head contacts.60 63 64 The translation of reduced head contacts to concussion risk reduction requires further investigation. Tackle training in practice sessions without helmets in football does not reduce head contacts in games.65 In addition, technical tackle training in professional rugby may improve tackle proficiency; however, further research is necessary to evaluate the effect on concussion risk.66
Although not primary prevention strategies, secondary prevention strategies may include baseline testing (eg, Sport Concussion Assessment Tool)85 to identify players at high risk for concussion and legislation ensuring assessment and clearance to return to play by a medical professional. The evaluation of such secondary prevention strategies should be targeted in future research. Considering the predisposition to concussion risk based on genetic susceptibility, such as Kristman et al 86 who examined apolipoprotein allele in concussed athletes, may be a future research direction.
Targeting intrinsic risk factors through individualised primary concussion prevention strategies may be important given the evidence supporting history of concussion as a significant risk factor for concussion.78 There is a greater risk of concussion in youth ice hockey when players report preseason symptoms (eg, headache, dizziness, neck pain).85 Abnormal dynamic visual acuity is greater in youth ice hockey players with a history of sport concussion.87 There is limited evidence evaluating the effectiveness of individualised primary prevention strategies targeting intrinsic risk factors. Clark et al 62 demonstrated an 85% reduction in concussion risk on collegiate football in an RCT examining the effectiveness of vision training preseason. Further research evaluating multifaceted primary prevention strategies targeting intrinsic risk factors is required.
A recently published systematic review examining concussion prevention strategies included only studies that used a prospective study design to evaluate the preventative effect of1 equipment,2 training or3 educational programs on the risk of concussions.88 This study was limited by a restricted search strategy (three terms and two electronic databases (PubMed and EBSCO)). It included only 15 studies, and meta-analyses were completed with extremely heterogeneous criteria (eg, outcome definitions). Schneider et al 88 did not examine the potential strategies that aim to reduce head impacts and did not capture potential environmental factors that could contribute to concussion prevention (eg, hockey rink size, board composition). In contrast, our systematic review captured 48 studies using 11 electronic databases and less restrictive inclusion criteria. The meta-analyses included in our systematic review considered more homogeneity in participants, sport, research design and outcomes.
Strengths and limitations
This is the most comprehensive systematic review and meta-analysis examining all published studies evaluating prevention strategies for sport concussion. Selecting only English-language papers may have introduced language bias. Measurement bias, including self-report bias, is an extremely prevalent bias in the selected studies. The measurement bias with regard to concussion definition would likely be non-differential in nature as the probability of a concussed player being classified as non-injured or a non-injured player being classified as concussed would likely be the same across study groups. This would bias the effect estimates toward the null. The use of convenience samples may have also affected the ability to show an age or sex effect. Although confounding was not considered in all studies, the cohort studies examining the risk of body checking did consider the potential effects of age, previous concussion and level of play. Publication bias may have affected our results. It is acknowledged that some industry-funded studies evaluating protective equipment may also introduce bias. Although some of these studies were summarised in systematic review, their results were not included in any meta-analysis. Finally, effect estimates and variability in the context of team sports require control for clustering by team in the analyses and this was rare in included studies. The evidence is limited based on exclusion of studies that considered TBI as an outcome broadly without distinction of mTBI or concussion. For example, the literature evaluating cycling helmets did not consider specifically the protective effect of helmets on reducing the risk of concussion specifically. Some studies that primarily considered all injury outcome may have been missed based on search terms aligning with TBI. In addition, inclusion of studies based on head impacts cannot translate to mTBI or concussion outcomes and further research is necessary.
Finally, there were nine authors that contributed to independently assessing the risk of bias in each study (two for each study), with a third author assessment when consensus was not met between two authors. The participation of nine authors may have led to some bias in the risk of bias assessment.
Conclusion
The strongest and most consistent sport concussion prevention evidence evaluates body checking policy disallowing body checking in youth ice hockey, demonstrating a significant protective effect in reducing the risk of concussion. This evidence has subsequently informed policy change in non-elite levels in older age groups and this requires further investigation. Further research is required to examine such rule changes in other collision sports, and alignment with biomechanical research to examine injury mechanisms is important. Regarding equipment, there is sufficient evidence in skiing/snowboarding to support strong recommendations and policy to mandate helmet use. The evidence for mouthguard use in preventing concussion is mixed, but meta-analysis suggests that there may be an overall protective effect in collision sports that cannot be ignored and rigorous case-control designs are required. Future research should focus on evaluating evidence-informed concussion prevention strategies targeting sport-specific extrinsic (eg, rules of the game) and intrinsic (eg, previous concussion history) risk factors. Prospective evaluation study designs (eg, cohort studies, RCTs), valid injury surveillance systems, consideration of potential confounders (eg, concussion history) and common concussion outcome definitions are needed. Concussion definitions consistent with international consensus guidelines and consideration exposure data (ie, player participation) to accurately measure injury rates are essential. Psychological and sociocultural factors in sport play a role in the uptake and maintenance of any injury prevention strategy and require further consideration in evaluating concussion prevention strategies.
Supplementary file 1
Supplementary file 2
Acknowledgments
The authors thank and acknowledge Dr Alix Hayden, MLIS, MSc, PhD (Librarian Taylor Family Digital Library, University of Calgary, Alberta) for her assistance with reviewing the systematic review protocol, search strategies and terms. We also thank Tanya Childs and Tate Hubka for their administrative contributions.
References
Footnotes
Contributors CAE was responsible for the conception and design of the systematic review, analysis and interpretation, drafting of the article, provided final approval and is the guarantor of the work; AMB contributed to the design of the systematic review, analysis and interpretation. AN-A conducted the meta-analyses and contributed to the interpretation. AMB, AK, CAE, GM contributed to the article search and selection process. AMB, AK, CAE, GM, KJ, LE, JK, DM, CT contributed to the risk of bias assessment. All authors contributed to the final systematic review plan (PROSPERO) and reviewed the article critically and provided final approval.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.