Article Text

Abstract
Objective To find predictors of cognitive decline and quality of life 1 year after bilateral subthalamic nucleus deep brain stimulation (STN DBS) in Parkinson's disease (PD).
Methods A total of 105 patients were evaluated with a comprehensive neuropsychological assessment before and 12 months after surgery. A control group of 40 PD patients was included to control for effects of repeated testing and disease progression. The authors determined individual changes in cognition, mood and quality of life using a statistical method that controls for multiple comparisons, and performed logistic regression analyses to assess predictors of cognitive changes and quality of life.
Results 12 months after surgery, the improvement in motor function was 41% (Unified Parkinson's Disease Rating Scale Part 3 score in off). The STN group showed a large improvement in quality of life compared with the control group (Cohen d=0.9). At the individual level, 32% (95% CI 22 to 40) of the STN group showed a substantial improvement in quality of life. 36% (95% CI 27 to 46) of the STN patients showed a profile of cognitive decline compared with the control group. Mood improved in 16 STN patients and declined in 16 subjects. Impaired attention, advanced age and a low l-dopa response at baseline predicted cognitive decline, whereas a high l-dopa response at baseline predicted an improvement in quality of life. Postoperative decrease in dopaminergic medication was not related to cognitive decline.
Conclusions STN DBS improves quality of life. However, a profile of cognitive decline can be found in a significant number of patients. l-dopa response, age and attention at baseline are predictors of cognitive and psychosocial outcome.
- Parkinson's disease
- deep brain stimulation
- subthalamic nucleus
- cognition
- behaviour
- quality of life
- cognition
- neuropsychology
- stereotaxic surgery
Statistics from Altmetric.com
- Parkinson's disease
- deep brain stimulation
- subthalamic nucleus
- cognition
- behaviour
- quality of life
- cognition
- neuropsychology
- stereotaxic surgery
Introduction
Bilateral deep brain stimulation of the subthalamic nucleus (STN DBS) is an effective surgical treatment to reduce motor symptoms in patients with advanced Parkinson's disease (PD).1–4 The effects of STN DBS on cognition and behaviour, however, are still the subject of controversy.5 6 Meta-analysis of 28 reports on cognitive outcome revealed small declines in executive functions and memory, and moderate declines in verbal fluency.6 However, most of the included studies lacked control groups. This is an important omission because cognitive decline can be expected as a result of disease progression itself, while conversely decline may be masked by retest effects. Another issue is that a statistically significant difference between groups on a cognitive test is of limited interest to understanding changes in the individual patient. Subtle changes in several cognitive domains may have more implications for daily life than a large significant deviation on a single test. Suppose, for example, that a patient shows declines in memory, attention and executive functioning, while each of his score decrements on the corresponding tests is too small to reach statistical significance. This patient and his relatives may very well note his change in mental functioning in daily life. Finally, it is uncertain which factors increase the risk of cognitive decline after STN DBS, although cognitive impairment prior to surgery and advancing age have been suggested.7
In this paper, we report the 12-month follow-up of the cognitive and behavioural effects of STN DBS. We determined groupwise and individual cognitive changes in STN patients compared with a nonsurgical control group.8 Likewise, we assessed individual changes in mood and quality of life after STN DBS. Finally, we analysed possible baseline predictors of cognitive outcome and quality of life, including age, l-dopa response, medication, preoperative mental status and prior stereotactic surgery.
Methods
Patients
Included were consecutive PD patients who underwent STN DBS. Twenty patients have been previously described.9 The remaining patients were recruited between June 2001 and June 2006 in three Dutch hospitals experienced in STN stimulation for PD. Eligible patients had idiopathic PD with an unequivocal reduction in off phase symptoms on l-dopa, and at least one of the following symptoms despite optimal pharmacological treatment: severe response fluctuations, dyskinesias, dystonia, tremor or bradykinesia. Exclusion criteria were predominantly unilateral symptoms without severe response fluctuations, severe brain atrophy on CT or MRI scans, Hoehn and Yahr stage 4 or 5 in the best on phase,10 dementia (Mattis' DRS <120),11 psychosis or depression at inclusion, or surgical contraindications.
Alongside the STN group, we formed a control group of patients recruited from two university hospitals and a teaching hospital in the Amsterdam region. They were patients who had idiopathic PD for at least 5 years and who did not (yet) want surgery or for whom the treating neurologist considered STN DBS not (yet) indicated. They were invited to participate as controls. Exclusion criteria were identical to those of the STN group (controls were not analysed for surgical contraindications). Inclusion and prospective evaluation of the controls occurred parallel in time to the STN group. The 6-month follow-up of this cohort has been reported before.12
The medical ethics committees of the participating hospitals approved the study.
Surgical procedure
The STN group underwent stereotactic surgery as previously described,2 using ventriculography, MRI or CT scan to determine the coordinates of the target structure. Surgical techniques were identical in the participating centres. Microelectrode recording was used in 43 patients. After macroelectrode test stimulation, a four-contact electrode (model DBS-3389, Medtronic, Minneapolis) was implanted. The electrodes were connected to implantable pulse generators (Itrel II, Soletra or Kinetra, Medtronic, Minneapolis) in a staged procedure under general anaesthesia. We did not systematically perform MRI postoperatively, because of restrictions of the Dutch radiological departments. The location of the leads was checked at the end of surgery by bidirectional skull x-ray in the stereotactic frame.
The efficacy of DBS was assessed by its effect on motor symptoms and the lack of adverse events. If possible, the medication was reduced, especially the dopamine agonists. Significant side effects were not tolerated.
Neuropsychological tests
The selection of tests was based on suggestions from the literature13: Mattis Dementia Rating Scale (DRS)11 14; category fluency (animals and occupations for 1 min each)15; Controlled Oral Word Association Test16; alternating fluency (body parts/cities or pieces of clothing/countries)17; Dutch Adult Reading Test18; Paced Auditory Serial Addition Task (PASAT), speed 3.2 s per digit19; Rey Auditory Verbal Learning Test (AVLT)20; Groningen Intelligence Test subtest Visuospatial reasoning15; Stroop Colour Word Test21; Odd Man Out Test (OMO)22; Trail Making Test parts A and B23; and Boston Naming test.24
To minimise practise effects, we used alternate forms where available in a balanced order across patients.
Mood and behaviour rating scales
The Dysexecutive Syndrome Questionnaire (DEX) of the behavioural assessment of the dysexecutive syndrome25 and the memory assessment clinic ratings26 27 were completed by the patient and a proxy. The CES-Depression28 and the Parkinson's Disease quality of life (PDQL)29 scale were filled out by the patient. We assessed neuropsychiatric changes with a Dutch translation of the Neuropsychiatric Inventory (NPI).30 31 The NPI consists of 12 items: delusions, hallucinations, agitation/aggression, dysphoria, euphoria, anxiety, apathy, disinhibition, irritability/lability, aberrant motor behaviour, night-time behaviour, eating behaviour. We constructed four more items based on the Frontal Behavioral Inventory.32 These items are: disgust and negligence, sexual interest, language and speech, and cognitive changes.12
During the test session, a combination of the abbreviated Profile of Mood States (POMS)33 and the Positive Negative Affect Scale (PANAS)34 was completed by the patient. The Montgomery & Åsberg Depression scale (MADRS)35 was filled out by the examiner.
Assessments
At baseline, motor function was scored using the Unified Parkinson's Disease Rating Scale part 3 (UPDRS3) and Hoehn and Yahr staging in standardised on and off phase.4 l-dopa response was calculated as follows: UPDRS3 score in off minus UPDRS3 score in on divided by the UPDRS3 score in off.
Follow-up assessment was done in the on phase 12 months after surgery for the STN group and 12 months after baseline for the control group. Standardised on/off evaluations of motor functioning at 12 months were available only for the second half of the STN series.
Statistical analyses
We compared baseline group differences in demographic and disease characteristics with the Mann–Whitney U test, because of skewed distribution of many of these variables. Change over time was analysed in the conventional way by subtracting the test and questionnaire scores at baseline from the follow-up scores to form change scores. The distributions of change scores were first examined for deviation from normality. Next, the change scores were compared at the group level by analysis of covariance and at the individual level in a new way that compared each STN patient with the control group (see below).
Group differences
To compare the change in both groups, we analysed the change scores with ANOVAs covarying for baseline differences (if any) between the groups in demographic or disease characteristics. Furthermore, we computed effect sizes of change (Cohen d: difference between the means of change scores of both groups divided by the pooled standard deviations of the change scores). An effect size of 0.2 reflects a small effect, 0.5 a medium and 0.8 a large effect.36 p Values of less than 0.05 (one-tailed) were accepted as statistically significant. We did not correct the level of significance for multiple comparisons to reduce the probability of type I error because we were mainly interested in detecting adverse effects of the surgical intervention. Under these circumstances, type II error (failure to detect an effect when it actually exists) is more serious than type I error (considering an effect to be real when it is actually not).37
Individual changes
We applied a new multivariate method of normative comparison to determine individual outcome.8 Usually, when we consider cognitive impairments in an individual patient, we compare each test score with its normative data to decide whether or not it is abnormal. If multiple tests are administered, as we did in the present study, the risk of finding at least one significant deviation when in reality there is none (the familywise false-positive rate) becomes very large. Moreover, the usual univariate approach is insensitive to specific patterns in deviations from the norm. Therefore, we used the multivariate normative comparison method (MNC), which tests whether a patient deviates from a control group on several characteristics simultaneously. The MNC is based on Hotelling's T2 statistic. It is appropriate in small samples and allows testing of one-tailed hypotheses, while the familywise false-positive rate is adequately controlled at 5%. We performed MNC on cognitive decline and on mood changes. Included in the analysis of cognitive decline were the change scores of the Mattis' DRS, category fluency, letter fluency, alternating fluency, PASAT, AVLT immediate and delayed recall, the Stroop subtests, Trailmaking A and B, Boston naming test and GIT visuospatial subtest. Because we were mainly interested in individual decline, we tested one-tailed (α=0.05). If the one-tailed MNC test is significant, then the individual shows a cognitive profile that deviates in a negative sense form the control group.
In the analyses of mood, we used scores on positive affect, negative affect, POMS subscales and CES-D. Because mood changes can be in the direction of depression as well as in the direction of improvement, we tested multivariate mood changes two-tailed (α=0.05). Individual outcome of quality of life was tested univariately with the change scores of the PDQL. Because similar studies in this field generally find an improvement in quality of life after surgery, we tested one-tailed (α=0.05), arbitrarily defining an improvement of more than 1.65 SD of the change scores in controls as substantial.
Predictors of outcome
Finally, we conducted logistic regression analyses to find characteristics that predict outcome in cognition and quality of life. To increase the power of the analysis, we computed cognitive composite variables. Raw test scores were converted into z-scores corrected for age and education based on the published norms of each test. The variable ‘verbal fluency’ consisted of the mean z-score on category fluency and on letter fluency; ‘memory’ combined the immediate recall and the delayed recall of the AVLT; and ‘mental speed’ combined Trailmaking A, Stroop Word and Stroop Colour Card. The composite of Trailmaking part B and the Stroop Colour Word Card was named ‘attention’ (short for divided and selective attention). Because of a lack of appropriate norms, we could not integrate the PASAT, the OMO test and the alternating fluency into these composites.
The dependent variable in the first logistic regression model was cognitive decline (yes/no) as determined with the multivariate normative comparison method. From the possible predictors (age, education, Mattis' DRS, verbal fluency, attention, memory, mental speed, l-dopa response, disease duration, prior stereotactic surgery, mood, dosage of dopaminergic medication at baseline, and application of microrecording during surgery) we chose the variables that had an association of p<0.20 with the dependent variable. A stepwise forward approach was used. In the logistic regression model for outcome in quality of life, the dependent variable was improvement of quality of life (yes/no) determined by univariate comparison. The independent variables were chosen from the same set of possible predictors according to the same procedure as described above. The predictor variables were not dichotomised.
Finally, we looked at the correlations of cognitive decline with postoperative decrease in dopaminergic medication and with postoperative increase in depressive symptoms, because these factors are often suggested to be associated with cognitive decline.
Results
Group characteristics
One hundred and eleven patients were included in the STN group. The control group consisted of 42 patients with PD. After 12 months, six patients from the STN group were lost to follow-up (two had an infection of the stimulator; one was imprisoned; three refused). Two patients from the control group were lost to follow-up (one deceased; one contracted an unrelated disease). Data from 105 patients of the STN group and 40 of the control group were analysed. One STN patient had a pallidotomy during the follow-up interval, two patients had a dislocated electrode, and two patients suffered a postoperative haemorrhage. These patients were not excluded. Group characteristics are shown in table 1. The STN group was significantly younger than the control group, had fewer years of education, had longer disease duration and used more dopaminergic medication. There were no differences in score on UPDRS part 3 or in Hoehn and Yahr score in ‘on’ phase.
Demographic and disease characteristics at baseline
Motor functioning and medication
STN stimulation had a clear positive effect on motor functions. The UPDRS-3 score in off phase improved 34% after 6 months compared with baseline.12 After 12 months, this score was 26.4 (SD 11.9; n=52); improvement was 41% compared with baseline. After 12 months, there was a large reduction in LEU in the STN group, whereas the medication dose in the control group hardly changed (median change in LEU in STN group: –150 (25th and 75th centile: –400, 40); median change in LEU in control group: 0 (25th, 75th: 0, 200), the difference in median change was significant (p<0.001 Mann–Whitney U test)).
Cognitive tests
The cognitive test scores of the groups are shown in table 2. At baseline, the STN and control groups did not differ significantly in cognition except for a lower score at the delayed verbal recall in the control group and a worse score for the STN group on the OMO test.12
Cognitive test scores at baseline and change scores (mean, SD) at 12 months' follow-up for the subthalamic nucleus and control groups
We conducted ANOVAs with change scores as the dependent variables and dopaminergic medication at baseline, and age, disease duration and years of education as covariates. The change scores were not skewed (skewness varied between −1.26 and 0.60) except for the Mattis DRS (skewness −2.33), while the correlations between the change scores were typically low (median r=0.25; 25th, 75th 0.18, 0.35). Twelve months after surgery, the STN group showed a significant decline compared with the control group on all verbal fluency measures, Mattis DRS, delayed recall of the AVLT, Stroop Colour Card and Stroop Colour–Word Card. These results were comparable with those of the 6-month follow-up.12 In addition, at 12 months' follow-up, the STN group showed a greater decline on immediate recall of the AVLT, Stroop Word Card, and visuospatial reasoning. Non-parametric testing of the group difference in Mattis DRS change score was also significant (p=0.003, one-tailed Mann–Whitney U test).
Mood and behaviour questionnaires
The results for mood and behaviour are presented in table 3. At baseline, the STN group showed significantly more symptoms of tension and fatigue on the POMS, more negative affect on the PANAS and a lower quality of life compared with the control group.12 Again, the change scores were not skewed (skewness varied from −0.62 to 0.39), while the correlations between the change scores were low (median r=0.15; 25th and 75th centile: 0.08 and 0.30). However, the distribution of change scores was not normal for many of the NPI items.
Scores on questionnaires at baseline and change scores (mean, SD) at 12 months' follow-up for the subthalamic nucleus and control groups
When we covaried for group differences at baseline in dopaminergic medication, age, disease duration and years of education, we found that 12 months after surgery, the STN group showed a greater improvement in quality of life on the PDQL compared with baseline than the control group (Cohen d=0.9). Relatives of the STN patients reported a larger increase in dysexecutive symptoms on the DEX at 12 months than the control group. Non-parametric testing of the NPI and additional items showed no group differences (the result of the hallucinations item, although significant, is negligible).
Individual outcome
The multivariate normative comparisons method revealed that 38 out of the 105 STN patients (36%; 95% CI 27 to 46) showed cognitive decline, that is a pattern of test results that deviated significantly and in a negative direction from the control group (one-tailed test). Furthermore, 16 patients (15%; 95% CI 8 to 22) reported a pattern of mood changes that deviated in a positive sense from controls, and 16 patients reported a pattern of mood changes that deviated in a negative sense from controls (two-tailed multivariate normative comparisons). Seventy-nine per cent of the patients had a positive PDQL change score after surgery. Univariate comparison showed a substantial improvement in quality of life in 34 of the 105 STN patients (32%; 95% CI 22 to 40). Nine patients reported improved quality of life despite showing cognitive decline. Change in cognition was not related to a change in quality of life (χ2=1.66, df=1, p=0.20).
Predictors of cognitive decline
In the logistic regression model with cognitive decline determined by the multivariate normative comparisons method as dependent variable, we entered (stepwise forward) the following independent variables: l-dopa response, age and composite scores of speed, attention and verbal fluency. Cognitive decline after surgery was significantly associated with attention at baseline (OR 0.41 (90% CI 0.28 to 0.62)), as well as with age (OR 1.07 (90% CI 1.01 to 1.13)) and l-dopa response (OR 0.97 (90% CI 0.94 to 0.99)). The correlations between the predictors were low (r<|0.13|), and multicollinearity was not a problem (variance inflation factors<1.03). The results indicate that patients with impaired attention at baseline, advanced age or with a low l-dopa response at baseline had a higher risk of cognitive decline after surgery. The expected chances of cognitive decline for the ages of 55 and 65 years, given the z-scores on attention and given l-dopa responses of 30%, 50% and 70%, are depicted in figure 1.

Predicted chances of cognitive decline 1 year after deep brain stimulation of the subthalamic nucleus as a function of preoperative attention functioning for relatively young patients (55 years, upper panel) and relatively old patients (65 years, lower panel), and for three levels of preoperative l-dopa challenge test result (30%, 50% and 70% improvement in Unified Parkinson's Disease Rating Scale part 3 score from off to on phase). Attention is expressed as the mean z-score of the Trailmaking test part B and the Stroop Colour–Word test interference condition, after correction for age and education. Cognitive decline is established by neuropsychological evaluation and multivariate normative comparison (see text; p<0.05 compared with PD control patients).
Predictors of quality of life
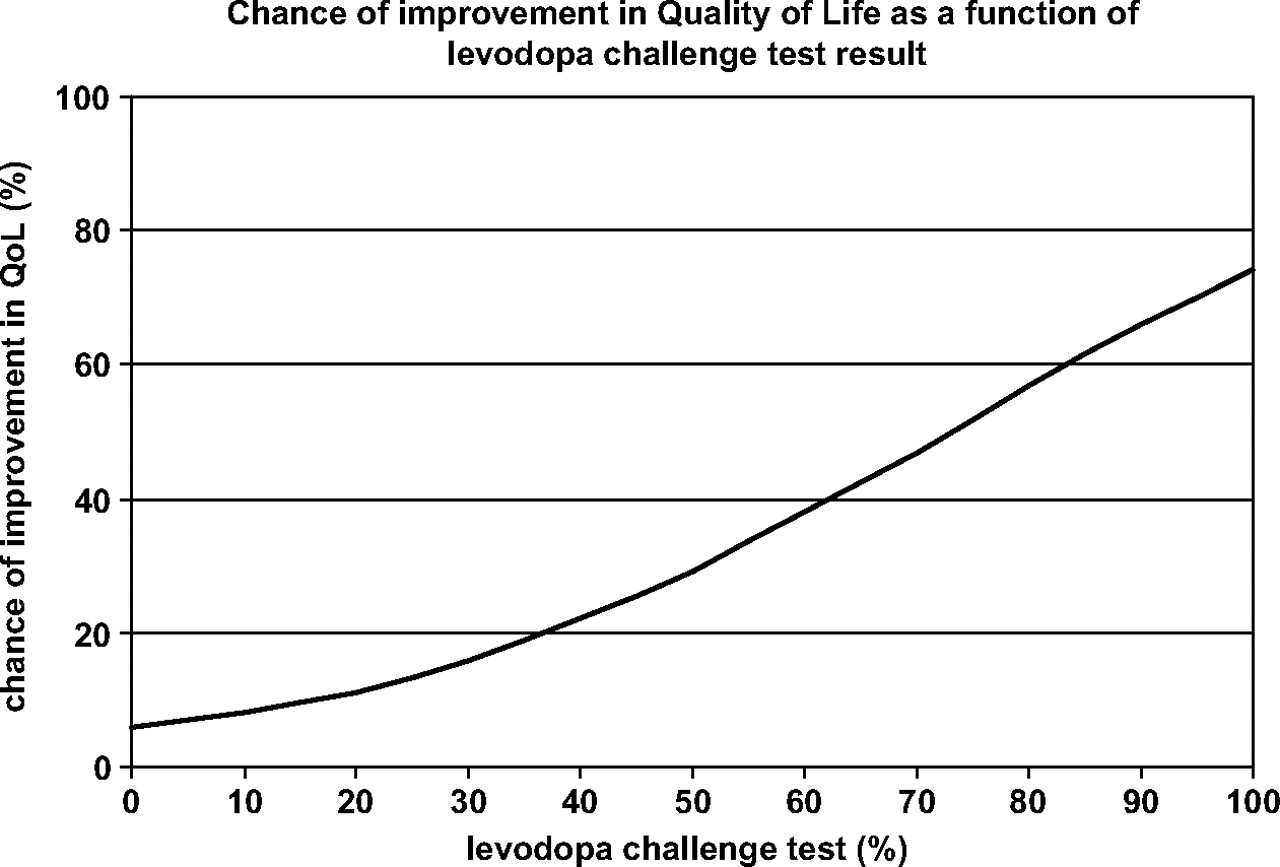
We entered l-dopa response, prior stereotactic surgery and Mattis DRS score into the regression analysis as independent variables and significant improvement in quality of life as the dependent variable. The OR of l-dopa response associated with improvement of quality of life was 1.04 (90% CI 1.02 to 1.06). The chances of improvement of quality of life as a function of l-dopa response are depicted in figure 2.

{kind=link}
{kind=link}
Predicted chances of substantial improvement in quality of life (Parkinson's Disease quality of life, p<0.05 compared with Parkinson's Disease control patients) as a function of preoperative l-dopa challenge test result (percentage improvement in Unified Parkinson's Disease Rating Scale Part 3 score from off to on phase).
Correlations with medication and depression
Cognitive decline in the STN group did not correlate with postoperative decrease in medication (r=0.01) and correlated slightly with postoperative increase in depressive symptoms on the MADRS (r=0.19). Cognitive decline correlated slightly with an increase in dysexecutive symptoms on the DEX (r=0.19).
Discussion
One year after STN DBS, we found a large improvement in quality of life. At the individual level, 79% of the patients reported at least some improvement, while quality of life improved substantially in at least one-third of the patients. Cognitive decline was found in a similar proportion of patients (36%). Some patients (9%) reported improved quality of life despite cognitive decline. Worsening of mood and improvement of mood were seen in comparable proportions (both 15%). l-dopa response at baseline predicted an improvement in quality of life. Attention at baseline, age and also l-dopa response predicted cognitive decline after surgery. Cognitive decline after STN DBS does not seem to be a temporary effect from which patients recover in the long term, because 12 months after surgery the effect sizes of most cognitive changes have become even larger (median −0.5) compared with the 6-month follow-up (median −0.3).12
The severity of cognitive decline ranged from a slight decline that was not even noticed by the patients themselves to severe decline. For advanced PD patients who often have borderline cognitive impairments, however, even a slight cognitive decline may imply a transition into evident impairments.
From reviews in the literature,5 the picture may arise that patients decline after STN DBS on some neuropsychological tests and improve on others. In almost all studies, these changes are based on group comparisons. When individual outcome is evaluated, it is often defined as the percentage of patients who improved or declined more than a SD on single tests. However, this approach suffers from a very high number of false positives.8 The multivariate normative comparisons method is more reliable, since it controls the number of false positives at 5%. With this method, we examined the profile of test performances of each of the STN patients compared with the controls. In this way, slight declines on several tests can be just as important as a large decline on a single test, because score decrements that are not significant at univariate statistical testing contribute to the overall result of the multivariate test. Probably, because of the statistical method we used, and because of the comprehensive way in which we assessed our patients, the percentage of cognitive decline in our study is higher than previously described.6 In essence, the application of this new statistical method, in combination with the use of a control group and the large sample size, is what distinguishes ours from previous studies. An advantage of this approach is that it facilitates the search for predictors because it detects more patients who have declined. A recent study that applied the usual univariate method in a similar cohort could not find predictors because it detected an insufficient number of patients as declined.38
Our findings are basically in agreement with what others have found. This can be seen, for example, in the decline of verbal fluency, which is the most consistent finding in this field. According to a recent meta-analysis,6 the mean decline of verbal fluency after STN DBS is 0.64 SD (95% CI 0.32 to 0.96). In our STN patients, category fluency declined 4.6 words, which equals an effect size of 0.46 (ie, 4.6/9.9; see table 2). The effect size of phonemic fluency in our patients is even smaller (4.1 words; ES=0.32). Also, as in almost all other studies, the decline in other cognitive domains than verbal fluency was small in our patients. With respect to demographic and disease characteristics, our patients were very comparable with, for example, the patients who were included in a large clinical trial by Deuschl et al.4 Also, the amount of motor improvement, the percentage of major adverse events and the neuropsychological findings in our study are comparable with those in the Deuschl study.4 39
The major limitation of our study is that it is not a randomised trial. Differences between STN patients and control patients in cognitive decline could be due to differences in demographic or disease characteristics. The STN group had a disease duration 3 years longer than the control group and used more l-dopa medication at baseline (table 1), implying more severe PD symptoms, which led to their recruitment in the surgical group. However, there were no differences in motor symptoms in the on phase. Moreover, the baseline differences did not explain a significant portion of variance in neuropsychological change scores. A second limitation is the fact that standardised on/off evaluation at 12 months was only performed in a subsample. Another limitation is that it is hard to decide when exactly a patient's quality of life has improved. Any cut-off value must be arbitrary, because there is no gold standard. A final but important limitation is the sample size of our study. Although it had the largest number of patients compared with other studies on neuropsychological aspects of DBS until now, this number is still quite small for establishing stable predictive models. Moreover, the models implicitly assume linear relations between predictors and outcome, but they may as well have a different form. The models as illustrated in the figures should be considered only crude approximations. Future studies should include more patients to find stable predictors of outcome and to assess their precise characteristics. However, it remains of importance that a comprehensive set of neuropsychological variables are studied, because subtle but clinically relevant changes will not be detected with coarse measures. Moreover, cognitive change was not restricted to verbal fluency or psychomotor speed but was also seen on several other measures, that is tests of memory and attention.
It has been suggested that cognitive decline after STN DBS might be associated with apathy resulting from postoperative decrease in dopaminergic medication.7 40 Apathy might result in an appearance of cognitive decline which is not actually there. However, this mechanism cannot explain our results, because the postoperative decrease in dopaminergic medication was not related to cognitive decline. Another hypothesis is that STN DBS stimulates the limbic area leading to an increase in depression, and subsequently to slight cognitive decline. We found a weak relationship between cognitive decline and postoperative increase in depressive symptoms, but even if depressed mood were a causative influence, it would only account for 4% of the variance in cognitive outcome. Finally, the idea that microrecording is related to cognitive decline because of the multiple tracks entering the brain leading to microlesioning,5 was not supported by our results (microrecording was not a significant predictor of decline).
We conclude that cognitive decline is fairly common after STN DBS, despite the improvement in quality of life. Our study indicates that best candidates for STN DBS are relatively young patients without impairments in attention, and with a high l-dopa response. However, further replication studies in other samples are needed to validate our prognostic findings. Our results should be taken as an ingredient that doctors and patients may use when they are balancing the pros and cons of the intervention.
Acknowledgments
We thank M Hoogman, R ten Dijke, A Rienstra and E Wijnalda (psychologists) for the neuropsychological testing of several patients; M Postma, L Daeter (Parkinson's nurses AMC), RMA de Bie, RAJ Esselink (neurologist UMC Nijmegen), B Post (neurologists AMC) and A Portman (neurologist UMC Groningen) for the scoring of motor functioning of the patients; J Kuster (neurologist from Kennemer Gasthuis Haarlem) and J Zijlmans (neurologist Ignatius ziekenhuis Breda) for recruitment of Parkinson's patients for the control group. WA van Gool and RJ de Haan made valuable comments on an earlier version of the paper.
References
Footnotes
Funding The study was supported by a grant from the Prinses Beatrix Fonds and the Parkinson Patiëntenvereniging.
Competing interests JDS acts as an independent consultant for Medtronic Ltd (Minneapolis). The movement disorders group of the AMC has received an unrestricted research grant from Medtronic Ltd.
Ethics approval Ethics approval was provided by the Medisch Ethische Toetsingscommissie, Academisch Medisch Centrum, Amsterdam.
Provenance and peer review Not commissioned; externally peer reviewed.