Article Text

Abstract
Aim To examine the prevalence of smoker support for a ban on cigarette sales in 10 years time and increased regulation of the tobacco industry and to investigate the independent associations of support for these measures.
Methods The authors surveyed opinions among adult smokers in two survey waves (N=1376 and N=923) from the New Zealand arm of the International Tobacco Control Policy Evaluation Survey during 2007–2009. The authors report prevalence of support stratified by age, gender and ethnicity. The authors carried out multivariate analyses to identify significant associations among potential determinants (demographics, socioeconomic status, mental health and smoking-related beliefs and behaviours) of support.
Results Most New Zealand smokers supported greater regulation of the tobacco industry (65%) and more government action on tobacco (59%). Around half (46%) supported banning sales of cigarettes in 10 years time, provided effective nicotine substitutes were available. In a fully adjusted model, significant associations with support for greater tobacco company regulation included Māori ethnicity, experience of financial stress and greater awareness about the harms of smoking. Significant associations with support for a ban on tobacco sales in 10 years time included increasing area-based deprivation level, increasing intention to quit and greater concern about the health effects of smoking.
Conclusions The findings suggest that most smokers will support stronger government action to control the tobacco industry and that many support radical ‘endgame’ approaches. Greater support among Māori, more deprived and possibly Pacific smokers, is an important finding, which could inform the design and implementation of new policies given the very high smoking prevalence among these groups and hence high priority for targeted tobacco control interventions. Perceived difficulties in gaining public support should not impede the introduction of rigorous tobacco control measures needed to achieve a tobacco-free New Zealand.
- Primary healthcare
- tobacco control in Africa
- prevalence
- environmental tobacco smoke
- cessation
- advocacy
- smoking-caused disease
- taxation and price
- economics
- public policy
- endgame
- harm reduction
- packaging and labelling
- tobacco control policy
Statistics from Altmetric.com
- Primary healthcare
- tobacco control in Africa
- prevalence
- environmental tobacco smoke
- cessation
- advocacy
- smoking-caused disease
- taxation and price
- economics
- public policy
- endgame
- harm reduction
- packaging and labelling
- tobacco control policy
Introduction
The level of public support for proposed policy options is an important factor in determining the feasibility and desirability of introducing and implementing policy at a range of levels, including central and local government. It also often forms a component of the justification and advocacy case in support of policy options.1
This is particularly true for health issues like tobacco control where policy introduction and implementation is often highly contested, notably by groups with an economic self-interest.2 ,3 These include the tobacco industry (and associated commercial allies in the retail and marketing sectors) or other sectors who may fear being affected in the future by stronger regulatory policies to reduce harm to health (such as the alcohol and processed food sectors).4 Others who may contest polices include politicians, commentators and other opinion formers who may also object on ideological grounds.5 Such commentators often highlight issues around ‘freedom of choice’ and cite the need to respect the views of the public, including smokers.
Levels of support among smokers are therefore key indicators to assess and monitor. If a tobacco control policy measure is supported by a majority of smokers, who may be perceived as having the most to lose or gain from its introduction, it is difficult to oppose the policy measure on the grounds of preserving individual freedom and autonomy and because of the need to respect the views of smokers.
Recently, some tobacco control organisations and official bodies have advocated ambitious targets for tobacco control, such as reducing tobacco smoking prevalence to close to zero within the short to medium term. These targets represent a tobacco ‘endgame’ scenario. For example, in Finland, a Tobacco Act was passed in 2010 which aimed to ‘put an end to the use of tobacco products in Finland’6 and The Cancer Society of Finland argues that Finland should aim to be wholly smoke free by 2040.7 In New Zealand, the Tupeka Kore (tobacco-free) vision was launched by a range of concerned non-governmental organizations and advocacy groups in New Zealand in 2009. The vision proposed a target of close to zero tobacco smoking prevalence by 2020 and a series of interventions to achieve this.8 Subsequently, the New Zealand government adopted the goal of ‘reducing smoking prevalence and tobacco availability to minimal levels … [to make] New Zealand essentially a smoke-free nation by 2025’.9 Smokeless tobacco is already banned in New Zealand. One proposed mechanism to achieve such an ‘endgame’ is for governments to introduce a ‘sinking lid’ system for import quotas (say 10% reduction in absolute terms per year) for tobacco products,until importation and commercial sale of tobacco products ceased.10
There has been increasing documentation of levels of support for key tobacco control policies before and after their introduction. This is perhaps best demonstrated by smoke-free workplace and public places legislation. The general pattern has been for such legislation to have high levels of public support, including among smokers, which increases in the period before and after implementation.11
There is also international evidence of strong support by smokers for a general increase in tobacco regulation. For example, a study of attitudes to tobacco regulation based on the International Tobacco Control (ITC) four-country study (data from Australia, Canada, UK and USA) found high levels of support for greater tobacco product regulation and more government action to tackle the harm caused by tobacco smoking among smokers. Across the four countries, this ranged from 62% to 71% for agreement with the statement ‘tobacco products should be more tightly regulated’ and 50%–66% support for the statement that ‘the government should do more to tackle harm caused by tobacco smoking’.12 Recent evidence from the USA suggests high levels of support for a range of measures to regulate tobacco products and tobacco product marketing, including regulation of tobacco products as a drug by a government agency, such as the Food and Drug Administration.13
There has been little documentation of support for endgame solutions. Surveys in the USA and England indicate some support for governments ending tobacco sales within 10 years.14 ,15 Relevant New Zealand research is mentioned below. However, there has been little in-depth analysis of the degree to which support for tobacco control measures varies by demographic and other factors. Tobacco smoking in many countries, particularly those in the developed world, is increasingly concentrated among more disadvantaged groups. It is therefore pertinent to developing the case for tobacco control interventions to explore levels of support among smokers from these groups, where smoking is most entrenched, and who are likely to be most impacted by the policies. Māori (the indigenous people of New Zealand) and Pacific peoples have smoking prevalences of up to twice as high as other New Zealanders,16 and smoking is a major contributor to the substantial disparities in heath between Māori and non-Māori.17 ,18 We have previously published brief reports of levels of support for tobacco control measures, including an end to tobacco sales in 10 years time, among Māori and Pacific peoples smokers compared with other New Zealander smokers19 ,20 and among the general population, Māori and Pacific peoples, and smokers.21
The main aims of this paper are to explore the attitude of smokers in New Zealand to increased regulation of the tobacco industry and to ending tobacco sales in 10 years time across different demographic groups and to investigate the independent associations of support for these measures.
Methods
The ITC project
The International Tobacco Control Policy Evaluation Survey (the ITC Project) is a multicountry collaborative study on tobacco use epidemiology and tobacco control policy evaluation. It has involved data collection in over 20 countries. A full description of the ITC Project conceptual framework and methods has been published.22 ,23
The New Zealand arm of the ITC Project participants are smokers recruited among subjects in the 2006/2007 New Zealand Health Survey (NZHS). The NZHS survey methods are detailed more fully in an overview24 and methodology report.25 Respondents were selected by a multistage, stratified, probability-proportional-to-size sampling design, with systematic boosted sampling of the Māori, Pacific and Asian populations. Face-to-face interviews with 11 924 respondents aged 18 years and over were conducted in respondents' homes by trained interviewers. The response rate was 67.9%.
Participants
We derived a sample of adult smokers from subjects who stated that they were willing to participate in further research at the end of the NZHS interview (85.2% of adult smokers in the NZHS). Of 2438 eligible subjects, 1376 (56.4%) completed a telephone questionnaire giving an overall combined response rate of 32.6% in the final ITC Project sample (for details, see an online Methods Report).26 Between-wave attrition of 32.9% resulted in 923 respondents in wave 2.
Procedures
Data collection was carried out using computer-assisted telephone interviewing (subcontracted to Roy Morgan Research). The first wave of participants was interviewed between March 2007 and February 2008, usually 3–4 months after their NZHS interview. Wave 2 was conducted between March 2008 and February 2009. The study protocol was cleared by the Multi-Region Ethics Committee in NZ (MEC/06/07/071) and by the Office of Research Ethics, University of Waterloo, Canada (ORE #13547).
Measures
We used indices that were used elsewhere in our ITC Project analyses (eg, in Borland et al 27and Young et al 12). These are fully described in an online Methods Report.26 Where new indices were developed, we assessed internal consistency using Cronbach's α, and only used indices where Cronbach's α scores were at least 0.5.
The particular questions relating to the tobacco industry and regulation were largely derived from wave 4 of the four-country ITC survey. However, the New Zealand arm of the study added some additional questions in both waves 1 and 2.
Respondents were categorised into three age groups (<35, 35–49 and ≥50 years). Ethnicity was prioritised with all those with Māori or Māori and other ethnic affiliations classified as Māori and all those with Pacific or Pacific and other ethnic affiliations classified as Pacific (unless Māori affiliation was also reported). The ‘European/other’ grouping included all ‘other’ (non-Māori, non-Pacific and Asian) ethnic groups.
We had multiple measures of socioeconomic status (SES) and other socio-demographic measures from the NZHS. We used a small area-based SES score developed for New Zealand (NZDep2006) which measures the level of socioeconomic deprivation for each neighbourhood (meshblock) according to a combination of nine 2006 Census variables28 This index has been used in many published articles and reports, and the predecessors of NZDep2006 (NZDep91, NZDep96 and NZDep2001) have been extensively validated.29 We also used an individual-level deprivation score created for the New Zealand setting (NZiDep). Although NZDep2006 and NZiDep are weakly correlated in our sample (Pearson's correlation coefficient, r=0.26, p<0.001), these are conceptually quite different measures.30
We also had two measures of financial stress: unable to pay any important bills on time in the last month and spending money on cigarettes that would have been better spent on household essentials in the last 6 months. These are correlated with each other (and the other SES measures)26 but involve significant conceptual differences.31 ,32 Indeed, all these variables could be included in the multivariate model without destabilising the model with intercorrelation.
Other measures which were included in the multivariate analysis were measures of mental health and a range of smoking-related attitudes, behaviours and beliefs (see tables 1 and 2). Most of the smoking behaviour and smoking-related belief questions were from the wave 4 of the four-country ITC survey.
New Zealand smokers' attitudes to tobacco companies and to tobacco regulation by sex, ethnicity and age
Logistic regression analysis for agreement with the statement that ‘If effective nicotine substitutes that are not smoked became available, the government should then set a date to ban cigarette sales in 10 years time’ (all the results weighted and adjusted for the complex design)
Weighting and statistical analyses
All analyses included weighting to make the sample representative of all New Zealand smokers and to adjust for the complex sample design (ie, multistage sampling with boosted sampling of Māori, Pacific peoples and Asians in the NZHS) and non-response in the NZHS and ITC Project survey. This resulted in our final sample being somewhat dominated by women (61.6%) and older smokers (64.7% aged 35 years and over) and having disproportionally higher percentages of Māori (44.1%) and disproportionally lower percentages for Pacific (6.5%), Asian (4.3%) and European/other (45.1%). A two-phase calibrated weighting procedure was used. A full description of the weighting process is detailed in two online reports.33 ,34
We conducted univariate analysis of the key socioeconomic and smoking variables and multivariate logistic regression analyses for the two key regulation measures. The latter used a conceptual framework, which assumed hierarchical relationships between demographic and socio-demographic factors35 that would dominate over smoking-related attitudes, behaviours and beliefs. All models included age, gender and ethnicity, and models 2 and 3 included key socio-demographic variables (eg, SES and financial stress). Model 3 added in a range of variables concerning smoking-related beliefs and behaviours and indicators of mental health and well-being. We forced these variables into the model 3 on the theoretical grounds that they were likely to be key characteristics that acted as high-level determinants of support for regulation.
All analyses were conducted in STATA (V.10; Stata Corp.).
Results
Smoker attitudes to banning cigarettes in 10 years time
Table 1 and figure 1 show the results of the general analysis of smoker attitudes to the tobacco industry and tobacco control activities and policies. There were no large differences or consistent patterns in smoker attitudes by age group or gender, but there were variations by ethnicity.
{kind=link}
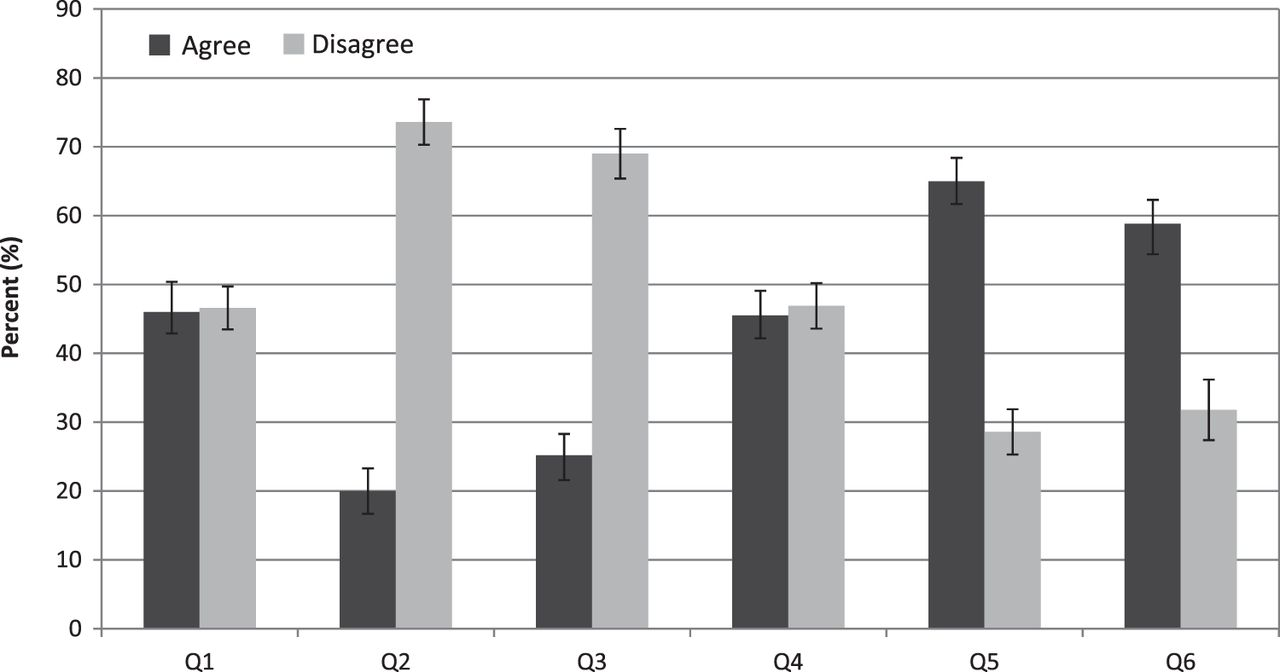
Degree of agreement and disagreement with statements about tobacco industry regulation, tobacco control and ending tobacco sales in 10 years.
Around half of smokers (46%) supported the banning of sales of cigarettes in 10 years, provided effective nicotine substitutes were available. Support was highest among Pacific (62%) smokers.
Around seven out of 10 smokers disagreed with the statements that the tobacco industry has done all they can to reduce the harm caused by smoking and that the industry should be allowed to advertise and promote cigarettes as they please (table 1). Only 20% and 25%, respectively, agreed with these two statements (figure 1). The level of disagreement varied little by gender, ethnicity or age group, except being lower among Pacific smokers (63% for both questions) and being higher (76%) among the youngest age group for the statement that the tobacco industry has done all it can to reduce harm caused by cigarettes.
There was majority (65%) support for greater regulation of tobacco companies. Only 29% disagreed with this statement. Support was strongest among women (69%), Pacific (74%) and Māori (71%) smokers. There was also majority (59%) support for more government action to tackle the harm done by smoking, with only 32% disagreeing. The level of support for this statement was highest among men (65%), Pacific (78%) and Māori (66%) smokers and lowest among smokers aged over 55 years (49%).
Agreement with the statement that the industry should take more responsibility for the harm caused by smoking was mixed—about half (46%) agreed and half (47%) disagreed. Agreement was strongest among men (50%), Pacific (60%) and Māori (50%) smokers.
Independent associations between smoker characteristics and support for banning cigarette sales in 10 years time
Table 2 shows the results of the logistic regression analyses to identify the determinants of support for a ban on the sale of smoked tobacco products in 10 years time, assuming that safer nicotine delivery products were available. The socio-demographic variables that were significantly associated with support were the small area deprivation measure (models 2 and 3, greater support with increasing deprivation) and one of the two measures of financial stress (model 2 only, greater support if financial stress present). There was a trend towards greater support among Pacific smokers, but this was not statistically significant. The beliefs and behaviours that were significantly associated with support in the fully adjusted model (model 3) were concern around smoking impact on health and quality of life in the future and strength of intention of quitting.
Independent associations between smoker characteristics and support for increased regulation of the tobacco industry
Table 3 shows the results of the logistic regression analyses to identify the determinants of agreeing that tobacco companies need to be more tightly regulated. Support was higher for Māori in all models (with a non-significant trend for greater support among Pacific smokers), for women in the model with just demographic variables (model 1) and for older smokers in model 3. One of the two measures of financial stress (not spending on household essentials) was also associated with greater support (models 2 and 3). Greater awareness of smoking-related harms was significantly associated with support in the fully adjusted model (model 3). In contrast, having a positive attitude to smoking and having strong self-exempting beliefs were associated with less support.
Logistic regression analysis for smoker agreement with the statement ‘tobacco companies should be more tightly regulated’ (all the results weighted and adjusted for the complex design)
Discussion
Main findings and interpretation
We found strong support for increased tobacco control efforts by the government and greater regulation of the tobacco industry among a nationally representative sample of New Zealand smokers. A key finding of this report was that among those expressing an opinion, around one-half supported the banning of sales of cigarettes in 10 years, provided effective nicotine substitutes were available.
The multivariate analysis indicated that those suffering from deprivation and/or financial stress are more likely to support a ban on cigarette sales in 10 years time. There were no statistically significant associations with ethnicity. The multivariate analysis also found that those with a greater intention to quit and concerns about the health effects of smoking are more likely to support such a future sales ban. Similarly, in multivariate analyses to identify possible determinants of support for increasing regulation of the tobacco industry, markers of socioeconomic disadvantage of financial stress and a greater concern or awareness of harms of smoking were associated with increased support. Māori ethnicity was associated with statistically significantly increased support for greater regulation of tobacco companies. Our findings for these New Zealand smokers were similar to those of the ITC four-country study,12 except that we found no consistent association with gender. The association with ethnicity was not examined in the ITC four-country study.
One explanation for support among Māori for greater regulation of the industry is that efforts by Māori tobacco control advocates over the last 5 years have focused significantly on the role of the tobacco companies in creating the tobacco epidemic among Māori. This argument also resonates well with broader colonisation arguments explaining the current marginalised position of Māori in NZ society.
Our data and the data from the ITC four-country study refer to support among smokers. Support is likely to be greater still among non-smokers. For instance, a telephone survey conducted in the USA in November 2009, with a sample weighted by race and gender, found that 45% of smokers and 71% of non-smokers agreed that ‘tobacco products should be regulated as a drug by a government agency such as the Food and Drug Administration’.13 In New Zealand, a survey conducted in 2008 involving face-to-face interviews with 1608 smokers and non-smokers found that six of 10 (59%) respondents overall and four of 10 (42%) current smokers agreed that the ‘government should do more to tackle the harm done by smoking’.21 ,36 In the same survey, 50% of all participants agreed that ‘cigarettes and tobacco should not be sold in NZ in 10 years time’ (30% disagreed).
Strengths and limitations
Strength of this study was that it involved a nationally representative sample and included a large proportion of Māori and Pacific smokers. A wide range of questions on different regulatory issues were asked and many of the questions have been used previously in other ITC studies, allowing for cross-country comparisons.
The findings may be specific in time and place. New Zealand has relatively advanced tobacco control policies, and the findings may well not apply in other settings with weaker tobacco control interventions. Furthermore, in New Zealand, since the data were collected for this study (2007–2009), there has been substantial additional tobacco control activity in this country including two tobacco tax increases, a decision to ban point-of-sale tobacco displays and a highly publicised enquiry by the Māori Affairs Select Committee into the tobacco industry which proposed further rigorous tobacco control measures.37 It is therefore plausible that smoker awareness of the problems around tobacco has increased and hence support for tobacco control regulation in 2011 might now be higher than is reported in this study.
A possible weakness with this study is that the respondents might have displayed some ‘social desirability bias’ in their responses and been more likely to have articulated pro-tobacco control views. This is possible because smoking is becoming increasingly denormalised in New Zealand (along with many other countries). For example, there have been reductions in socially cued smoking following the recent expansion of indoor smoke-free environment laws in this country.38 This social desirability bias may act both as a confounder and as a source of measurement error (ie, both correlated and dependent measurement error). Nevertheless, we feel it is unlikely to have been substantial, given that responses to other questions about support for tobacco control measures (not reported here) found highly nuanced and variable responses.39 For example, a large majority of smokers supported smoking being permitted in outdoor hospitality settings. This suggests that most respondents were not simply defaulting to the most pro-tobacco control answers.
The question relating to support for the government to set a date for banning of sales of cigarettes in 10 years was predicated on effective nicotine substitutes being available. This may have increased support. The findings of another survey from 200821 give an indication of the level of support without this qualifier. The proportion of smokers agreeing with the statement ‘Cigarettes and tobacco should not be sold in New Zealand in 10 years time’ was 26% (55% did not support).
The relatively low response rate may have resulted in selection bias. However, as noted in the Methods section, a two-phase calibrated weighting procedure was used to address non-response and hence minimise any resulting selection bias due to differential non-response.
Research and policy implications
The major policy implications of this research are that New Zealand smokers would support more vigorous tobacco control efforts and regulatory approaches. In particular, that those most at risk from deprivation and/or financial stress appear most likely to (conditionally) support a ban on tobacco sales. This research suggests that governments should not be deterred from introducing such measures due to possible political unpopularity among smokers. Indeed, New Zealand research indicates that tobacco tax increases would be supported by a majority of smokers if the extra revenue was used for health and quit help purposes.40 Furthermore, our impression is that the substantial tax increases in April 2010 and January 2011 in New Zealand were well accepted by the public and in media discourse and seemed to reflect positively on the politicians involved by showing them in a clear leadership role.
Another possible policy implication comes from the finding of greater support for the tobacco control measures among smokers with a greater intention to quit, concerns about the health effects of smoking and knowledge of smoking harms. This suggests that intervention which increase smokers' knowledge and beliefs about the health effects of smoking and enhance motivation to quit will in turn lead to more support for new tobacco control interventions.
One of the areas for further work highlighted by the findings of this study is the need to explore what additional interventions would enhance support among smokers for endgame strategies. For example, further work could explore what type of more effective nicotine substitutes would need to be available for smokers to accept a future ban on tobacco sales. We acknowledge that this is a one off survey, and it will also be important to carry out further work to document trends in support for tobacco control interventions and strategies, particularly as these become more familiar and public debate about them increases. There are many other facets of smoker and public support that could be investigated further as this country moves towards its tobacco-free goal. For example, the levels of support for different levels of tobacco tax increases, options to restrict the supply of tobacco products and various proposed ‘endgame’ solutions included structural reforms to the market, distribution systems and regulatory apparatus.
Conclusions
In summary, this study extends on previous ITC four-country findings that stronger government action to control the tobacco industry is likely to be supported by the majority of smokers. In addition, this research found moderate support for more radical ‘endgame’ approaches to tobacco control among smokers. The support for increased tobacco control measures was found across both genders and all age groups, socioeconomic groups and ethnicities. Support was greater among Māori and possibly Pacific smokers, an important finding, given their very high smoking prevalence and hence high priority for targeted tobacco control interventions. Results from other studies in New Zealand and elsewhere suggest that levels of support among non-smokers will be even higher still. We conclude that the findings suggest that difficulty in gaining public support should not be considered an impediment to introducing strong tobacco control measures, including measures to achieve the tobacco endgame that will greatly improve and protect the health of populations afflicted by the current tobacco epidemic.
What this paper adds
-
There has been little documentation of support for rigorous tobacco control measures including of endgame solutions, which aim to end the use of tobacco products.
-
This paper found majority support among smokers for greater regulation of the tobacco industry and more government action on tobacco.
-
Almost half supported a ban on cigarette sales in 10 years time. Support was at least as strong among lower SES and Mâori smokers.
-
The findings suggest that stronger government action to control the tobacco industry is likely to be supported by most smokers and that there is already substantial support for more radical ‘endgame’ approaches to tobacco control among smokers.
-
Difficulty in gaining public support should not be considered an impediment to introducing strong tobacco control measures, including measures to achieve the tobacco-free 2025 goal in New Zealand.
Acknowledgments
The ITC Project (New Zealand) team thank the following for their support: the interviewees who kindly contributed their time to answer the survey questions; the NZ Ministry of Health, which provided a wide range of support for the Project, particularly access to the NZHS data; other members of our ITC Project (New Zealand) Team including Roy Morgan Research for conducting the interviews; the Data Management Core at the University of Waterloo, Canada, and the agencies which support the ITC Project internationally (particularly the Canadian Institutes of Health Research (#79551); the Roswell Park Transdisciplinary Tobacco Use Research Center (TTURC—P50 CA111236), funded by the US National Institutes of Health and many other funding agencies as detailed on the ITC Project website: http://www.igloo.org/itcproject/).
References
Footnotes
-
Funding The NZ ITC Project was funded by The Health Research Council of New Zealand (grant number 06/453).
-
Competing interests Although we do not consider it a competing interest, for the sake of full transparency, we note that some of the authors have undertaken work for health sector agencies working in tobacco control.
-
Patient consent This study did not involve patients. It included smokers drawn from the general population who gave their consent to take part in the surveys.
-
Ethics approval Ethics approval was provide by the Multi-Region Ethics Committee in NZ (MEC/06/07/071) and by the Office of Research Ethics, University of Waterloo, Canada (ORE#13547).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Unpublished data have not been made available to anyone as yet.