Article Text

Abstract
Introduction Hydroxychloroquine (HCQ) is an important medication for treating systemic lupus erythematosus (SLE). Its blood concentration ([HCQ]) varies widely between patients and is a marker and predictor of SLE flares. This prospective randomised, double-blind, placebo-controlled, multicentre study sought to compare standard and adjusted HCQ dosing schedules that target [HCQ] ≥1000 ng/ml to reduce SLE flares.
Patients and methods [HCQ] was measured in 573 patients with SLE (stable disease and SELENA-SLEDAI≤12) treated with HCQ for at least 6 months. Patients with [HCQ] from 100 to 750 ng/ml were randomised to one of two treatment groups: no daily dose change (group 1) or increased HCQ dose to achieve the target [HCQ] (group 2). The primary end point was the number of patients with flares during 7 months of follow-up.
Results Overall, mean [HCQ] was 918±451 ng/ml. Active SLE was less prevalent in patients with higher [HCQ]. A total of 171 patients were randomised and followed for 7 months. SLE flare rates were similar in the two groups (25% in group 1 vs 27.6% in group 2; p=0.7), but a significant spontaneous increase in [HCQ] in both groups between inclusion and randomisation strongly suggested improved treatment adherence. Patients at the therapeutic target throughout follow-up tended to have fewer flares than those with low [HCQ] (20.5% vs 35.1%, p=0.12).
Conclusions Although low [HCQ] is associated with higher SLE activity, adapting the HCQ dose did not reduce SLE flares over a 7-month follow-up.
ClinicalTrials.gov NCT00413361
- Systemic Lupus Erythematosus
- Pharmacokinetics
- Treatment
Statistics from Altmetric.com
Systemic lupus erythematosus (SLE) is a systemic disorder with significant morbidity and mortality. Therapeutic management is based on the type and severity of organ involvement and may include non-steroidal anti-inflammatory drugs, hydroxychloroquine (HCQ), low to high doses of corticosteroids, and several groups of immunosuppressive agents.1 Long-term use of the latter two remains associated with morbidity and mortality.2
HCQ, an inexpensive antimalarial drug, is now recognised as an important medication for SLE.3–5 In addition to its efficacy in preventing SLE flares,6 HCQ protects against diabetes mellitus, thrombotic events, dyslipidaemia and overall damage accrual in patients with SLE.4 It may therefore improve survival in SLE.4 ,7
Blood HCQ levels ([HCQ]) can be quantified by high-performance liquid chromatography (HPLC). The great interindividual variability in [HCQ] raises the question of a possible relation between drug concentration and efficacy. Such a pharmacokinetic/pharmacodynamic (PK/PD) relation for HCQ has been found in rheumatoid arthritis8 ,9 and cutaneous lupus.10 Similarly, we have reported that low [HCQ] is a marker and predictor of SLE exacerbations, with a target threshold [HCQ] of 1000 ng/ml.11 These findings led us to conduct this randomised prospective study designed to determine the potential benefits of individualising HCQ dosing schedules to reach this target [HCQ] and thereby decrease SLE flare rates (Plaquenil LUpus Systemic: PLUS Study; ClinicalTrials.gov number, NCT0041336).
Patients and methods
Patients
The PLUS Study was a randomised, double-blind, placebo-controlled, multicentre trial conducted from June 2007 through August 2010 at 37 centres in France.
The inclusion criteria required that patients: be adults with a diagnosis of SLE according to the American College of Rheumatology classification criteria12; have received HCQ treatment for at least 6 months; have not had their HCQ dose modified for 2 months; have a stable daily dose of HCQ (200 or 400 mg every day); have stable SLE with steroid dose no higher than 0.5 mg/kg/day of prednisone equivalent and not increased during the preceding 3 weeks; have had no modification of an immunosuppressant during the previous 2 months; and have a Safety of Estrogens in Lupus Erythematosus National Assessment SLE Disease Activity Index (SELENA-SLEDAI)≤12.13
Exclusion criteria were known or suspected non-adherence to the treatment, known retinopathy, a severe cataract that made ophthalmological monitoring impossible, monophthalmic status, history of HCQ intolerance (in particular, gastrointestinal or retinal), use of chloroquine during the preceding 3 months, biotherapy during the preceding 12 months, estimated glomerular filtration rate (calculated from serum creatinine according to the Cockcroft–Gault equation) lower than 60 ml/min, chronic alcoholism, liver failure, pregnancy or desire for pregnancy in the next 7 months, breast feeding, or lack of coverage by the French national health insurance fund.
At inclusion, all patients had blood tests that included whole-blood HCQ measurements in a centralised laboratory by HPLC with fluorimetric detection, as previously described.11
All participants provided written informed consent.
Randomisation
Patients with [HCQ] ranging from 100 to 750 ng/ml at inclusion were eligible for randomisation. Patients with [HCQ] <100 ng/ml were considered non-adherent and were therefore not randomised.14 Patients with [HCQ]>750 ng/ml were not eligible for randomisation because they were so close to the therapeutic target.
Other randomisation criteria required that patients had not had any increase in their steroid dose or any immunosuppressant modifications since inclusion, SELENA-SLEDAI ≤ 12, had stable SLE activity (maximum SELENA-SLEDAI increase 2 points), had an ophthalmological examination in the preceding 6 months with no contraindication to HCQ, and had no significant conduction disorders on ECG, and that women of child-bearing age should be using effective contraception and have a negative β-human chorionic gonadotropin (hCG) test.
Eligible subjects (ie, patients with [HCQ] ranging from 100 to 750 ng/ml at inclusion and meeting the other randomisation criteria) were randomly assigned in a double-blind manner to receive either the same dose of HCQ that they had been receiving (group 1) or an increased dose aimed at achieving [HCQ] of 1000 ng/ml or higher (group 2). The maximal allowed daily dose was 800 mg/day.
The randomisation scheme was stratified according to centre and steroid dose (<10 or ≥10 mg/day).
Treatment
HCQ (Plaquénil, tablets of 200 mg) and placebo (appearance identical with the Plaquénil tablets) were conditioned in weekly boxes with four tablets per day, according to the four possible randomisation doses to maintain the double-blind condition. For example, patients assigned to receive 200 mg/day received boxes containing one HCQ tablet and three placebo tablets daily, while those assigned to receive 800 mg/day received boxes containing four HCQ tablets for each day. Thus, four packaging boxes were available, containing 200, 400, 600 and 800 mg/day. All four boxes were sent to the pharmacy of the hospital of each patient eligible for randomisation.
Patients with no HCQ daily dose modification (group 1) were assigned to receive either 200 or 400 mg/day, according to their usual treatment. Patients in group 2 were assigned to a HCQ daily dose adjusted to their previous daily dose and to their [HCQ]. Since the pharmacokinetics of HCQ is linear, the adaptation of the dose was determined with an adaptation table, and they received 400, 600 or 800 mg/day (see online supplementary table S1). At randomisation, the computer determined the randomisation group (1 or 2), calculated the required dose (200–800 mg/day) and attributed to the patient a number corresponding to one of the four boxes available in the centre.
Follow-up
Randomised patients were followed-up for 7 months (1 month to allow group 2 to reach the target concentration plus 6 months of follow-up). SLE activity and side effects were assessed for all patients at randomisation and at 1, 3, 5 and 7 months (visits at month 1, month 3, month 5 and month 7). Patients were asked to contact their physician if they developed symptoms of an SLE flare and were then promptly examined. Follow-up data were collected until the end of the 7 months, even for subjects who had discontinued the study drug.
End points
The primary end point was the percentage of patients experiencing at least one SLE flare, as assessed by the SELENA-SLEDAI flare composite score, which defines both mild/moderate and severe flares13 (see online supplementary table S2), between randomisation and month 7. Briefly, this score includes three elements: the SELENA-SLEDAI score; an assessment of new or worsening disease activity, medication changes and hospitalisations not captured with the use of the SLEDAI; and the score on the physician's global-assessment visual analogue scale.13 Information about the use of this score was provided at each site before the study began.
Secondary end points were: (1) the percentage of patients experiencing at least one severe SLE flare; (2) the percentage of patients experiencing at least one SLE flare after exclusion of patients who had flares between randomisation and month 1, meaning before any effects of the study intervention were to be expected; (3) the percentage of patients experiencing at least one SLE flare in patients who met the [HCQ] target (all [HCQ]≥1000ng/ml after randomisation, defined as the high-[HCQ] group) compared with this percentage among patients in the low-[HCQ] group (all [HCQ])<1000 ng/ml after randomisation).
Assessment of SLE flares
The specialist treating each patient scored all components of the flare composite index. At each visit, all patients underwent a complete physical examination and laboratory testing—that is, complete blood cell count, serum creatinine assay, urinalysis, C3 assay by nephelometry, antinuclear antibody test (HEp2000 slides; ImmunoConcepts, San Diego, California, USA; positivity set at 1/80), and anti-double-stranded DNA (anti-dsDNA) antibody measurement by ELISA (Eti-dsDNA; DiaSorin, Saluggia, Italy) and Farr (Trinity Biotech, provided by InGen) assays.
The C3 assays, antinuclear antibody tests and anti-dsDNA antibody measurements were centralised in the Immunology Laboratory of the Pitié-Salpêtrière Hospital. The study was conducted in accordance with the International Conference on Harmonisation Guidelines for Good Clinical Practice and the ethical principles of the Declaration of Helsinki. The study protocol was approved by a French ethics committee (Comité de Protection des Personnes St Louis). The study was monitored by an independent data and safety monitoring committee. Adverse events were reported to the institutional review board if they were serious or contributed to discontinuation of the study drug. More than 2 million tablets of HCQ and placebo were provided free of charge by Sanofi. The company had no role in the initiation, planning, conduct, data assembly, analysis or interpretation of the study.
Statistical analysis
Sample size was calculated by assuming that during the 7-month follow-up, 30% of the patients in group 1 and 11% of those in group 2 would experience at least one SLE flare. Accordingly, 200 randomised patients were needed to conclude that HCQ dosing adaptation was superior to standard management with a power of 80% and a two-sided type I error rate of 5%. However, the PLUS Study data and safety monitoring board elected to close enrolment after 171 patients had been randomly assigned, because recruitment was difficult and the 3-year planned study duration had elapsed.
The intent-to-treat population was used for all analyses. It was defined to include all randomised patients who received at least one dose of study medication. Predictive factors of [HCQ] at inclusion were identified with a stepwise multivariate linear regression model. Changes from randomisation to month 7 in [HCQ] were compared between randomisation groups with analysis of variance for repeated measures. Adjustment for multiple comparisons used the Tukey–Kramer method.
The percentages of patients with at least one SLE flare during the follow-up were compared using the χ2 test, and the percentages of those with severe SLE flares using Fisher's exact test. Factors predictive of SLE flares were identified by stepwise multivariate logistic regression. Variables included in the model were SELENA-SLEDAI scores, C3 levels (binary), anti-dsDNA antibody levels, and physician's global-assessment visual analogue scale at randomisation.
All tests were two-sided. The level of significance was set at 0.05. Statistical analyses were performed with SAS V.9.2.
Results
Enrolment
A total of 573 patients were included and had [HCQ] assessed at inclusion (figure 1). Their mean±SD age was 39±12 years, 92% were women (n=525), and 96% had positive antinuclear antibodies at inclusion. Median disease duration was 8.0 (range 0.5–38.9) years, and the median duration of HCQ treatment was 6.7 (range 0.5–33.4) years. Mean [HCQ] was 918±451 ng/ml. Only 12% (n=68) had active SLE (SELENA-SLEDAI>4). Mean [HCQ] was significantly lower in patients with active than inactive SLE (793±411 vs 935±454; p=0.01). Conversely, 16% of patients with [HCQ] ≤ 750 ng/ml had SELENA-SLEDAI>4, compared with 8.9% of those with [HCQ]≥1000ng/ml (p=0.02).
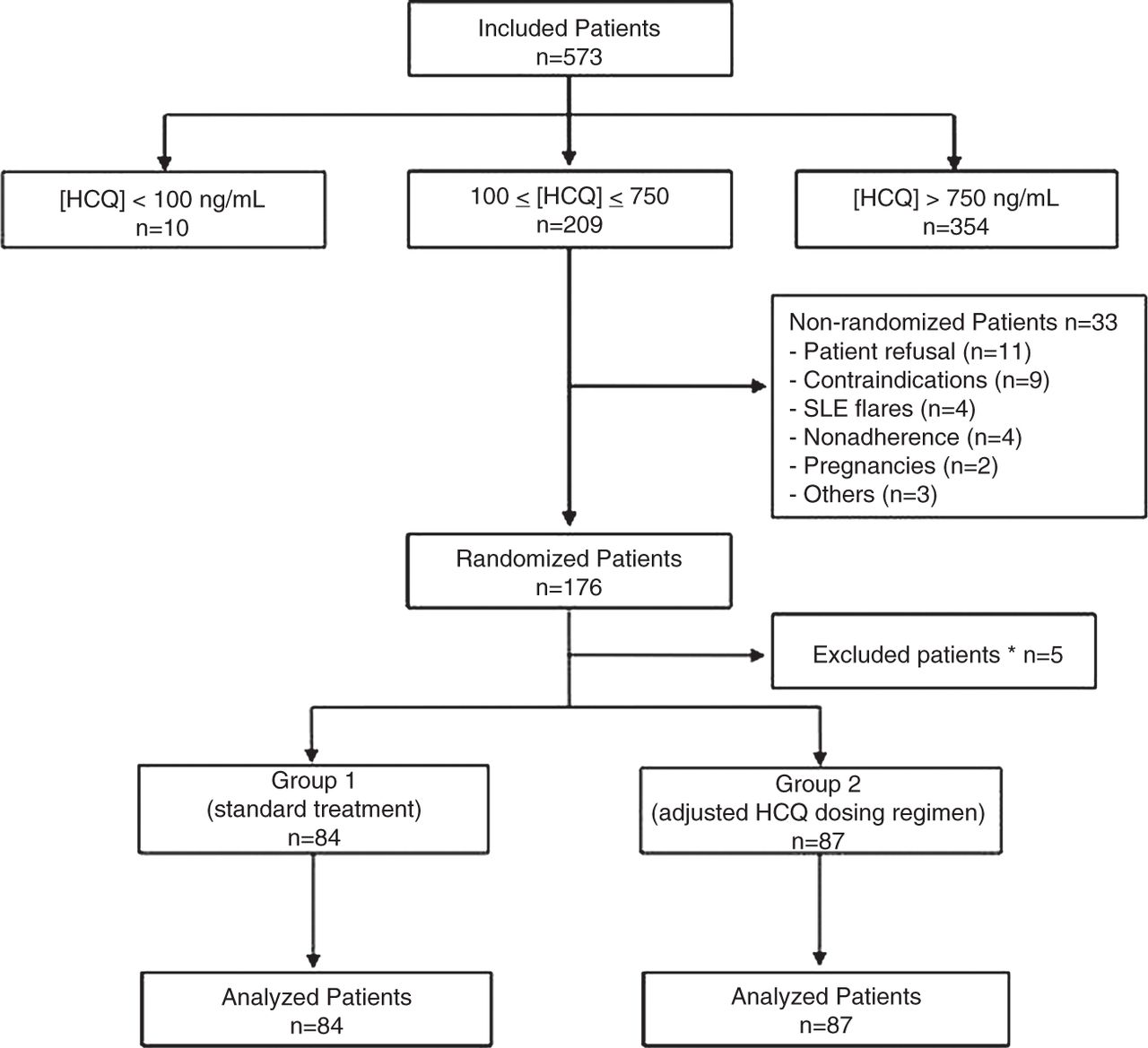
Study flow chart. *Randomisation criteria were not met, and patients did not receive the study treatment. Group 1: standard treatment (no change in daily hydroxychloroquine (HCQ) dosage). Group 2: adjusted HCQ dosing regimen (to obtain a blood HCQ concentration of ≥1000 ng/ml).
Ten patients had very low [HCQ](<100 ng/ml), and 354 had [HCQ]>750ng/ml. [HCQ] for the remaining 209 patients ranged from 100 to 750 ng/ml, a range that we had previously identified as associated with a higher risk of developing flares.11 These 209 were accordingly eligible for randomisation. Of these, 33 were not randomised because of late refusal (n=11), contraindications to a high HCQ dose (ophthalmological, n=8, and renal insufficiency, n=1), SLE flares between inclusion and randomisation (n=4), report of non-adherence to treatment (n=4), pregnancy (n=2), or other causes (n=3).
Of the 176 randomised patients, five were excluded from the analysis because they finally did not meet the randomisation criteria and did not receive the study treatment. The remaining 171 patients were followed for 7 months. Four patients (one in group 1 and three in group 2) stopped the study treatment during the follow-up. No patient was lost to follow-up.
Table 1 summarises the subjects’ clinical characteristics at randomisation.
Characteristics of the study subjects at randomisation, by group
Primary end point
The number of patients with flares between randomisation and month 7 did not differ significantly between the groups: 25% in group 1 (21 of 84 subjects) and 27.6% in group 2 (24 of 87 subjects; p=0.70) (table 1).
Secondary end points
The number of patients with a severe flare was low and similar in the two groups: 4.8% in group 1 (4 of 84 subjects) and 3.4% in group 2 (3 of 87 subjects; p=0.67). Nor did the groups differ when we excluded patients with flares between randomisation and month 1—that is, before any effect of the study intervention was expected (p=0.93).
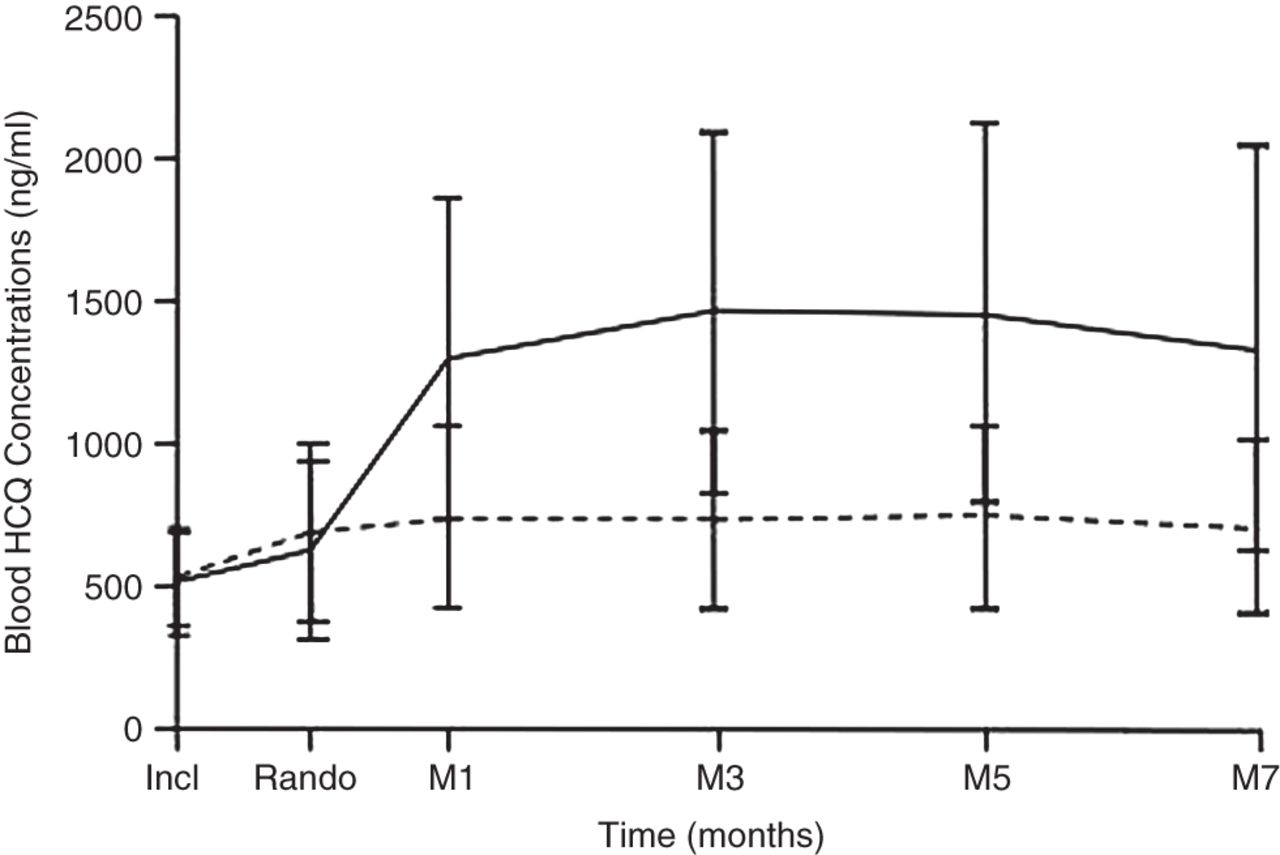
Between inclusion and randomisation—that is, before any change in treatment—[HCQ] for the two groups together increased significantly, by a mean of 136±301 ng/ml (p=0.0001) (figure 2). This finding strongly suggests that adherence to treatment improved. At randomisation therefore, only 114 randomised patients (66.7%) still had [HCQ] between 100 and 750 ng/ml. To minimise the effect of variations of adherence during the study, and because our initial goal was to compare patients with low [HCQ] with patients with ‘therapeutic’ [HCQ] (ie, ≥1000 ng/ml), we analysed the occurrence of flares in the high-[HCQ] group (patients in whom all [HCQ] values after randomisation were equal to or higher than 1000 ng/ml; n=39) and in the low-[HCQ] group (patients in whom all [HCQ] values were below 1000 ng/ml after randomisation; n=57) (table 2). These two groups were similar with regard to age, sex, SLE characteristics, other treatments, body mass index, smoking status, physician-reported treatment adherence, serum creatinine level, C3 level, SELENA-SLEDAI at randomisation, and percentage of patients with active SLE at randomisation. The high-[HCQ] group showed a trend toward a lower median duration of HCQ treatment (4.8 (0.7–20.5) vs 7.8 (0.7–30) years in the low-[HCQ] group; p=0.06). The high-[HCQ] group had a lower rate of SLE flares (20.5% vs 35.1%; p=0.12). Only three severe SLE flares were observed in these 96 patients, all in the low-[HCQ] group (p=0.27). When the analysis was restricted to patients who had no flares between randomisation and month 1 (36 in the high-[HCQ] group and 55 patients in the low-[HCQ] group), the rate of SLE flares was 13.9% vs 32.7% (p=0.04), respectively.
Characteristics at randomization of the patients who met the objectives of [HCQ] ≥1000 ng/ml and of those with [HCQ]<1000 ng/ml from month 1 to month 7

{kind=link}
{kind=link}
Course of blood hydroxychloroquine concentrations (mean±SD) during the study in randomised patients. Incl, inclusion; Rando, randomisation; M1, month 1; M3, month 3; M5, month 5; M7, month 7; HCQ, hydroxychloroquine. The number of patients was 573 at inclusion and 171 patients at randomisation and after. Broken line, group 1 (standard treatment; n=84 patients); plain line, group 2 (adjusted HCQ dosing regimen to obtain a HCQ concentration of ≥1000 ng/ml; n=87 patients). Blood HCQ concentration increased significantly in both groups between inclusion and randomisation (before any therapeutic intervention). After randomisation, blood HCQ concentration was significantly higher in group 2.
In the multivariate analysis, the only factors associated with SLE flares throughout the entire follow-up were the SELENA-SLEDAI score at randomisation (OR=1.35 (95% CI 1.11 to 1.64); p=0.002) and low [HCQ] (all post-randomisation [HCQ] values <1000 ng/ml; OR=3.82 (95% CI 1.16 to 12.58); p=0.027).
Adverse events
At least one adverse event occurred during the study to 17 (20.2%) patients in group 1 and 23 (26.4%) patients in group 2 (p=0.34). Specifically, 12 patients in group 1 and eight in group 2 reported nausea and vomiting, three and six diarrhoea, zero and four pruritus, and two and two blurred vision. No difference in the rate of adverse events was observed between the high-[HCQ] group (28.2%) and the low-[HCQ] group (26.3%) (p=0.84).
The side-effect rate was 38.9% in patients receiving 200 mg/day (n=18), 15.5% in patients receiving 400 mg/day (n=71), 25% in patients receiving 600 mg/day (n=20), and 27.4% in patients receiving 800 mg/day (n=62). Specifically, no differences were seen between groups in terms of nausea, vomiting, diarrhoea or blurred vision. Four patients had pruritus and all were treated with 800 mg/day HCQ. None stopped treatment because of pruritus.
Discussion
The adaptation of HCQ dose aimed at maintaining [HCQ] above 1000 ng/ml did not reduce the rate of SLE flares during a 7-month period. The first and simplest explanation may be that higher HCQ doses do not have an added therapeutic effect. However, several factors may provide an alternative explanation of why our study did not prove its primary hypothesis.
The maintenance of [HCQ] above 1000 ng/ml during the 7-month follow-up was difficult to achieve. Only 39 patients had [HCQ] that remained at this therapeutic target throughout the entire follow-up (high-[HCQ] group). Interestingly, when analyses were restricted to these patients, there was a trend toward fewer SLE flares compared with patients in the low-[HCQ] group (20.5% vs 35.1%, p=0.12). This difference reached statistical significance when patients with flares between randomisation and month 1—that is, before any effects of the study intervention were to be expected—were excluded (13.9% vs 32.7%; p=0.04). It is thus possible that, if we had adapted the daily dose of HCQ to [HCQ] at each study visit, we would have proved our hypothesis. For logistical reasons, this was not feasible: given the delay between visits and results of [HCQ] measurement, a modification of treatment at each point of the study while maintaining the double-blind condition would have required all patients to return a second time for each study point, after their results were ready, and restocking all pharmacies at each point. Our results indicate, however, that the design of future studies must allow for more than one adjustment and must continuously monitor [HCQ].
Two factors might explain the failure to maintain [HCQ] above 1000 ng/ml. The first is the pharmacokinetic variations of HCQ, but this explanation is unlikely because HCQ has a long terminal half-life and these patients were thought to be in a steady state. The second potential explanation might be adherence problems, even though known or suspected non-adherence was a major criterion for exclusion in our study. We found 10 patients with [HCQ] sufficiently low at inclusion to constitute an objective marker of lack of compliance.14 Four additional patients eligible for randomisation admitted that they were non-adherent and were therefore not randomised. Nonetheless, between inclusion and randomisation, [HCQ] significantly increased despite the lack of any therapeutic intervention; this finding strongly suggests that some patients were more adherent to HCQ after inclusion than before. Consequently, at randomisation, only 66.6% of the patients were still in the target [HCQ] for randomisation, and only a few patients remained at their target concentration throughout the entire study.
This result underlines the utility of [HCQ] measurement for identifying and correcting non-adherence. In a previous study, we found that 7% of 203 patients with SLE were non-adherent,14 and this proportion increased to 30% when the analysis was restricted to patients with active SLE (SELENA-SLEDAI ≥12). Recently, Ting et al15 found that 29% of adolescents and young adults with SLE were non-adherent, as defined by undetectable [HCQ], and that medication adherence estimates using [HCQ] correlated with adherence rates obtained from pharmacy refill information (Pearson correlation coefficient r=0.50, p<0.0001). One of the main causes of treatment failure in patients with chronic diseases, including SLE, is the lack of adherence to treatment, especially among younger patients.16 We have observed that the ability to identify poor adherence routinely and easily helps us to manage patients with SLE in daily practice14 (and personal data). This seems particularly useful in patients with active disease who are at higher risk of non-adherence.
We observed a 26.3% rate of SLE flares during a 7-month follow-up period. This rate is lower than those found in other studies with quite similar patients with SLE and end points. For example, in the OC-SELENA trial, the probability of at least one flare during the 12-month follow-up period was 76% for subjects receiving oral contraceptives and 69% for those receiving placebos.13 It is possible that, even if there is a strong PK/PD relationship for HCQ, the simple fact of any HCQ treatment at all markedly reduces the rate of SLE flare and thus makes it difficult to observe a difference related to HCQ doses adapted to [HCQ]. Consistent with this hypothesis, the Canadian HCQ Study Group found in their 6-month, randomised, double-blind, placebo-controlled study of the effect of discontinuing HCQ treatment in 47 patients with SLE with clinically stable SLE that 36% of patients receiving HCQ had SLE flares versus 73% in those receiving placebo.6
Finally, it is a common theme of SLE trials that observed differences in treatment effects are considerably smaller than expected. Apart from the limitations specific to our study discussed above, reasons might include: (1) populations heterogeneous for disease pattern, severity, duration or treatment; (2) insufficient control of concomitant medications with steroids up to 0.5 mg/kg/day permitted in our study; (3) short follow-up; and (4) use of a flare assessment tool that, like other SLE flare definitions, has problems with reliability and sensitivity as recently emphasised by Isenberg et al.17 Although the failure to prove our hypothesis through our primary end point was disappointing, we confirmed the close relation between SLE activity, determined by the SELENA-SLEDAI, and [HCQ] among the 573 patients: the prevalence of active SLE was lower in patients with higher [HCQ]. This finding is consistent with our previous results in patients with SLE11 and in 300 patients with cutaneous lupus.10 Because patients with ongoing SLE flares, who are known to have lower [HCQ],11 ,14 were not included in our study, the persistence of a link between [HCQ] and SLE activity clearly emphasises the importance of the PK/PD relation for HCQ. Interestingly, the cut-off of 1000 ng/ml is consistent with the cut-off associated with biological effects in in vitro studies.18 ,19
Finally, we note that these patients, including the group treated with a dose of 800 mg/day, received high HCQ doses for 7 months without significant side effects. In the past decade, a renewed interest in HCQ has emerged in the field of cancer, because of the drug's antiautophagic properties.20–22 Preliminary results show a strong PK/PD relation, but a dose of 600 or 800 mg/day might be required to reach the desired antiautophagic effect in clinical practice.23 Our safety data are reassuring in this context.
The primary limitation of our study is that we included only 171 patients even though the calculated sample size called for 200, so that the power of our study might be questioned. Nonetheless, this is very unlikely to have affected our results given the similarity of the flare rates in groups 1 and 2. Another limitation is that the trend toward lower SLE flare rates in patients with higher [HCQ] must be interpreted cautiously, since this analysis was not performed according to randomisation group. This result might also be explained by better adherence to other medications, especially steroids.
In conclusion, this study confirms the PK/PD relation for HCQ in patients with SLE. Our results do not justify recommending a therapeutic adaptation of HCQ dose to [HCQ]. However, we suggest that [HCQ] be measured to detect non-adherence, especially in patients with active disease, and to help patients with poor adherence reach [HCQ]≥1000 ng/ml.
Acknowledgments
To the patients, to the Association France Lupus (AFL) for a grant for this study, to the Clinical Research Unit of Pitié-Salpêtrière Hospital, which dealt with the methodological aspects, data management and monitoring, to the sponsor of the study—Assistance Publique–Hôpitaux de Paris—and to Sanofi, which provided the HCQ and placebo tablets.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
ZA and JCP contributed equally.
-
Collaborators Leonardo Astudillo, Cristina Belizna, Nadia Belmatoug, Olivier Benveniste, Audrey Benyamine, Holly Bezanahary, Patrick Blanco, Olivier Bletry, Bahram Bodaghi, Pierre Bourgeois, Benoît Brihaye, Emmanuel Chatelus, Richard Damade, Eric Daugas, Christian de-Gennes, Jean-François Delfraissy, Céline Delluc, Aurélien Delluc, Pierre Duhaut, Alain Dupuy, Isabelle Durieu, Hang-Korng EA, Dominique Farge, Christian Funck-Brentano, Frédérique Gandjbakhch, Justine Gellen-Dautremer, Pascale Ghillani-Dalbin, Bertrand Godeau, Cécile Goujard, Catherine Grandpeix, Claire Grange, Lamiae Grimaldi, Gaëlle Guettrot-Imbert, Loïc Guillevin, Eric Hachulla, Jean-Robert Harle, Julien Haroche, Pierre Hausfater, Jean Jouquan, Gilles Kaplanski, Homa Keshtmand, Mehdi Khellaf, Olivier Lambotte, David Launay, Hervé Levesque, Olivier Lidove, Eric Liozon, Kim LY, Matthieu Mahevas, Kubéraka Mariampillai, Xavier Mariette, Alexis Mathian, Karin Mazodier, Marc Michel, Nathalie Morel, Luc Mouthon, Rokiya Ngack, Jacques Ninet, Eric Oksenhendler, Jean-Luc Pellegrin, Olivier Peyr, Anne-Marie Piette, Vincent Poindron, Fabienne Roux, David Saadoun, Sabrinel Sahali, Bernadette Saint-Marcoux, Françoise Sarrot-Reynauld, Yoland Schoindre, Jérémie Sellam, Damien Sene, Jacques Serratrice, Pascal Seve, Jean Sibilia, Claude Simon, Christelle Sordet, Benjamin Terrier, Salim Trad, Jean-François Viallard, Elisabeth Vidal, Bertrand Wechsler, Pierre-Jean Weiller, Noël Zahr.
-
Contributors The first author wrote the initial draft of the manuscript. All the authors contributed to subsequent drafts and had unrestricted access to the data during this process. All the authors made the decision to submit the manuscript for publication and assume responsibility for the accuracy and completeness of the data. All the authors attest that the study was performed in accordance with the protocol and the statistical analysis plan.
-
Funding This study was funded by a grant from the French PHRC 2005 (number 05-125) Ministère de la Santé; the ‘Direction de la Recherche Clinique et du Développement’ provided logistic and administrative support. Sanofi provided the HCQ and placebo tablets. The company had no role in the initiation, planning, conduct, data assembly, analysis or interpretation of the study.
-
Competing interests None.
-
Ethics approval The study protocol was approved by a French ethics committee (Comité de Protection des Personnes St Louis Hospital, Paris).
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.