Article Text

Abstract
The Last Gift is an observational HIV cure-related research study conducted with people with HIV at the end of life (EOL) at the University of California San Diego. Participants agree to voluntarily donate blood and other biospecimens while living and their bodies for a rapid research autopsy postmortem to better understand HIV reservoir dynamics throughout the entire body. The Last Gift study was initiated in 2017. Since then, 30 volunteers were enrolled who are either (1) terminally ill with a concomitant condition and have a prognosis of 6 months or less or (2) chronically ill with multiple comorbidities and nearing the EOL.
Multiple ethical and logistical challenges have been revealed during this time; here, we share our lessons learnt and ethical analysis. Issues relevant to healthcare research include surrogate informed consent, personal and professional boundaries, challenges posed conducting research in a pandemic, and clinician burnout and emotional support. Issues more specific to EOL and postmortem research include dual roles of clinical care and research teams, communication between research personnel and clinical teams, legally required versus rapid research autopsy, identification of next of kin/loved ones and issues of inclusion. Issues specific to the Last Gift include logistics of body donation and rapid research autopsy, and disposition of the body as a study benefit.
We recommend EOL research teams to have clear provisions around surrogate informed consent, rotate personnel to maintain boundaries, limit direct contact with staff associated with clinical care and have a clear plan for legally required versus research autopsies, among other recommendations.
- End-of-life
- Ethics
- Research Ethics
- Clinical Ethics
- HIV
Data availability statement
No data are available. This paper details ethical reflections and documented lessons learned. As such, no data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Biomedical research should be an iterative process, one of constant learning. HIV cure-related research is no different. This is particularly true in the case of HIV cure-related research conducted at the end of life (EOL). The EOL is an emotionally charged time1 that often accentuates the already non-trivial challenges of conducting concurrent clinical research.2 Here, we detail our ethical and practical lessons learnt to date from the Last Gift, an observational HIV cure-related research study conducted on people with HIV (PWH) at the EOL at the University of California San Diego (UCSD).3
The search for an HIV cure (ie, either eliminating the HIV provirus from the body or inducing long-term suppression without the use of therapy) is currently gaining traction with over 250 completed or active studies worldwide.4 5 Most of these studies have enrolled otherwise healthy PWH.3 6 The latent reservoir, however, remains the main hurdle to curing HIV.7 HIV reservoir dynamics cannot be fully understood with non-invasive sampling procedures involving living participants; rapid research autopsies are necessitated to obtain the large deep-tissue samples required to adequately characterise and quantify them.3 8–11 A new research paradigm involves conducting HIV cure-related research with altruistic participants at the EOL to better understand the HIV reservoir throughout the entire body.3
We initiated the Last Gift in 2017 and have since enrolled 30 volunteers who are either (1) terminally ill with a concomitant condition and have a prognosis of 6 months or less or (2) chronically ill with multiple comorbidities and nearing the EOL.3 Last Gift participants agree to voluntarily donate blood and other biospecimens while living and their tissues for a rapid research autopsy postmortem.3 The next of kin (NOK)/loved ones of participants play an integral role in EOL research, and their respect, cooperation, acceptance and involvement are often necessary.12
Ubiquitous ethical and practical challenges abound in any study conducted at the EOL, but even more so in HIV cure research involving rapid research autopsies.9 10 13 As we initiated the study, we detailed ethical considerations for conducting HIV cure-related research at the EOL in collaboration with our community advisors.3 The purpose was to anticipate ethical considerations that would be encountered during the study and devise a strategic ethics plan. Despite our best attempts to foresee ethical and practical challenges, some arose which we did not predict. Issues relevant to healthcare research include the COVID-19 pandemic, surrogate informed consent, personal and professional boundaries, challenges posed conducting research in a pandemic, and clinician burnout and emotional support. Issues relevant to EOL and postmortem research include dual roles of clinical care and research teams, communication between research personnel and clinical teams, legally required versus rapid research autopsy, identification of NOK/loved ones and issues of inclusion. Issues specific to the Last Gift include logistics of body donation and rapid research autopsy, and disposition of the body as a study benefit.
Where possible, we illustrate the challenge(s)/question(s) as well as the solution(s) that we employed. To inform ethical lessons learnt, we consulted published evidence from the HIV3 7 11 14 and non-HIV2 10 15 fields. We also consulted UCSD research ethics committees and stakeholder groups, such as the UCSD AntiViral Center (AVRC) Community Advisory Board (CAB) advising on the study. Our team is also committed to robust qualitative research12 16–18 to understand how interested parties perceive HIV cure research at the EOL, including what they consider ethical and acceptable. We hope our critical reflections and ethical analysis will meaningfully contribute to the field of HIV cure-related research at the EOL and that our lessons learnt may prove beneficial for future similar or analogous studies.
Issues relevant to healthcare research
Conducting research in a pandemic
When COVID-19 hit, the Last Gift had 10 participants in follow-up. We were met with the issues of balancing responsibility to the participants and reducing spread of COVID-19. Guidance in March 2020 from the US Centers for Disease Control and Prevention and local authorities to avoid unnecessary interactions19–21 led to the suspension of study visits and new enrolment.
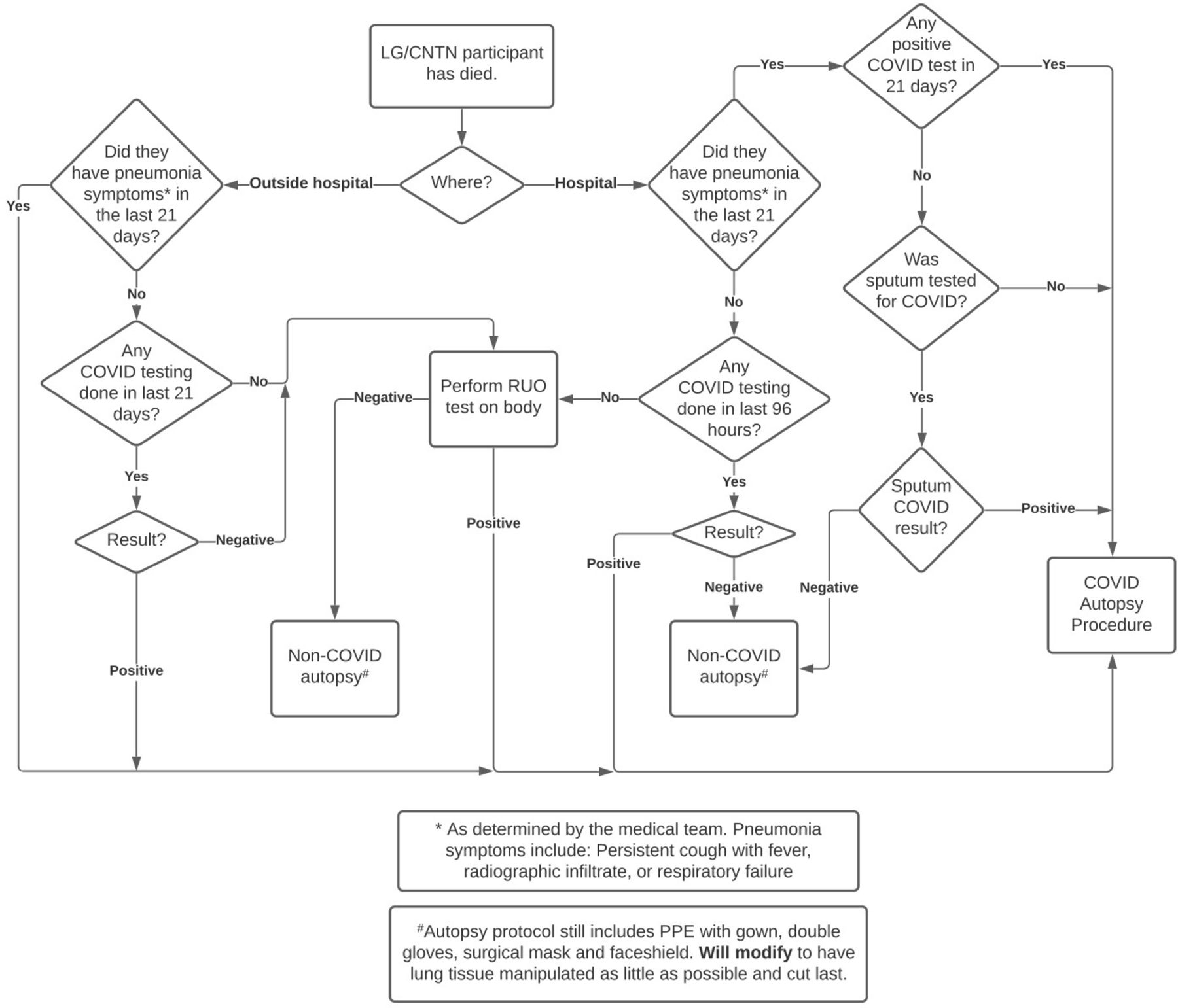
We developed a decision tree for testing deceased participants for SARS-CoV-2 to minimise risk of spread (figure 1).1 By May 2020, we were able to conduct limited study visits with participants and converted many surveys and check-ins to telephone visits to reduce unnecessary contact. In-person visits were reduced by at least half from the normal schedule and, whenever possible, blood collections were done in conjunction with visits that participants already had with their medical providers, rather than conducting home visits. These efforts served to conserve personal protective equipment and limit risk to study staff. All study staff were vaccinated against SARS-CoV-2, and home visits only occur where necessary for participants who are unable to come to our phlebotomy site. With the emergence of new SARS-CoV-2 variants (eg, BA.1 and BA.2 Omicron subvariants) and as the pandemic continues to evolve, we keep monitoring and conservatively adapting our protocol and visit schedule. Of course, safety of our participants and staff remains our priority.

{kind=link}
Last Gift study COVID-19 autopsy decision tree. CNTN, California NeuroAIDS Tissue Network.
Surrogate informed consent
Informed consent is of paramount importance in the Last Gift to ensure a participant’s autonomy in making EOL decisions that uphold their personal values.22 Obtaining informed consent, however, can be challenging when dealing with volunteers near the EOL.22 23 Informed consent is obtained initially from Last Gift participants.3 We also employ consent checks throughout the study to ensure participants’ continued willingness to participate.3 We also ask for a legally authorised representative to be able to provide ongoing consent in the event of the participant losing capacity. Surrogate (ie, NOK) consent may sometimes be necessary for enrolling patients who cannot provide consent themselves.10 24 This must be considered on a case-by-case basis,3 and we have extensive institutional review board (IRB)-approved protocols in place for such a situation. In particular, we require documented proof that the participant would want to be involved in tissue donation for research, such as enrolment into the California NeuroAIDS Tissue Network. All Last Gift participants underwent standardised neuropsychological evaluation at enrolment and during the study.3 The research team recognises that neurocognitive impairment in late-stage HIV and high prevalence of depression at the EOL25 could confound decisions about study enrolment and ongoing participation, and carefully monitors the mental health state of participants throughout the entire study.
A situation arose in which surrogate consent was used; however, a Last Gift participant later had to be withdrawn from the study after regaining capacity and on learning about his desire to no longer participate. We recommend other research teams to have clear provisions around surrogate informed consent, particularly those conducting research at the EOL.
We further recommend participants to prepare advance directives separately from the Last Gift study. The research staff explaining the informed consent form asks if the potential participant has an advanced care planning document. If not, the Last Gift research staff provides the forms and educational materials when requested to do so. Potential participants do not have to have an advanced care directive document to participate. Although advance directives may lack specificity for the EOL HIV cure research context,26 they serve as a catalyst for meaningful conversations. In the Last Gift, we view advance directives as taking precedence over the aims of the research protocol. The Last Gift does not require any changes to the advance directives. On the contrary, the Last Gift team does its best to comply with all wishes as listed in the advance directives.
Burnout and emotional support
HIV cure-related research at the EOL has the potential to significantly advance science towards an HIV cure,6 8 but it can also take a heavy toll on the mental health of team members. The AVRC CAB raised the issue of staff burnout. To mitigate against this, they suggested having psychotherapy support in place for the Last Gift team, which was instituted. The rapid research autopsy team also valued taking a moment of remembrance at the start of each autopsy and decompressing after each one.
In some cases, the Last Gift team has participated in celebrations of life with NOK/loved ones. Our research team recognises the possible benefits and risks to NOK/loved ones and research staff in sharing these non-professional spaces. We have a separate sociobehavioural research component designed to examine the emotional effects of the programme on NOK/loved ones12 17 and research staff.18 In addition, a suggestion was made to create a grieving fund to support affiliated individuals who may need additional support.
Personal and professional boundaries
On paper, it is easy to separate research team members from participants. In EOL research,1 however, the line between personal and professional boundaries can become blurred. In one instance, a participant was known to our study nurse in a social context prior to the participant’s enrolment in the study. We held a discussion with the participant, the nurse and the study team to assess the non-research relationship between the participant and the nurse, as well as to establish safeguards for their new research relationship. As a result, the participant was offered visits by other staff members and the nurse was allowed to opt out of visiting the participant. The participant, however, felt more comfortable seeing the well-known nurse, and the nurse felt comfortable visiting an old friend knowing it would bring them solace. These decisions were regularly re-evaluated throughout the study. As the participant neared the EOL, they sought increasing support from the nurse. The study team began discussions on how to conduct future study visits, but the participant passed away before a resolution could be reached. As a result of this incident, we regularly check in with study personnel and rotate personnel, where appropriate, so that no single staff member is solely responsible for any one participant. We recommend this practice for future EOL research protocols.
In many cases, there is no resolution other that being aware of one’s own personal involvement. Team members sometimes become emotionally invested in participants, and participants come to see them as part of their extended family. In one example, a participant became such an advocate for the study and worked so closely with one of the study investigators that that investigator opted not to participate in the autopsy. We encourage self-awareness such as this and, further, we suggest regular discussion as to how various roles can be shared so that no individual becomes too burdened by EOL emotions.
Issues relevant to EOL and postmortem research
Dual roles: clinical care and research
Many of our investigators provide clinical care outside of the Last Gift. In a study as specific as the Last Gift, the pool of potential volunteers is very limited. Thus, on rare occasions, members of our team initially encountered patients who later became participants in our study, as part of clinical care. This can prove challenging because the investigator role is separate from the clinician role as both serve different objectives15: biomedical research seeks to develop generalisable scientific knowledge, while clinical care seeks to directly provide health benefits to patients.27 Additionally, the Last Gift was not designed to provide care for participants, not even palliative care.3
From a participant’s perspective, we were aware that the Last Gift could become conflated with clinical care because of this shift in roles. Participants may also feel compelled to participate in the study because they may fear losing their clinical care if they do not.15 Further, if a participant’s clinical care is not going well, they may blame the study for their negative experience.
Though this tension between the role of researchers and clinical care providers is hardly unique to our study, it is sometimes more pronounced in the case of research at the EOL.15 The disparate roles that members of our team sometimes play need to be explained in the enrolment process and revisited throughout the study. Future researchers could consider including the potential shift in roles from being a clinician caring for the potential participant to being a researcher in the consent forms.
Further, if a role can be performed by different study personnel (eg, study visits, blood draws and informed consent), Last Gift personnel who were not part of the participant’s clinical team are employed in lieu of faces participants may associate with clinical care. During the COVID-19 pandemic, the study team has been able keep the roles separate from the participant’s perception despite the shortage of clinical personnel. We recommend EOL research teams to limit direct contact with staff who may be associated with clinical care.
Communication between research personnel and clinical care team
Often, team members are asked to communicate on the participant’s behalf with the clinical care team and, on occasion, we discover concerns while reviewing the participant’s medical record. We should communicate on the participant’s behalf when we have consent to do so, when warranted or to minimise immediate harm to a participant. We must also carefully evaluate each situation on a case-by-case basis. Two examples illustrate this point. In the first, we encountered a participant asking one of our study team members to reinitiate his antiretroviral therapy, something that the study team has no control over. In the second example, we found a participant had been prescribed two complete antiretroviral therapy regimens following an emergency room visit, which the staff at their hospice facility had failed to notice.
The challenge arose in how the clinical team perceived our conveyance of such messages. If we relay a message of restart/increase/change medications, it may appear to be coming from a place of judgment, and the subtext may be seen as ‘Why are you not seeing your patient often enough to have heard this concern yourself?’ While we have no formal procedures in place for dealing with such, we usually forward the patient/participant’s request to their primary care provider (PCP) with the explicit proviso that we were asked by the patient/participant to communicate the request to the PCP. In the previous examples, study team members emailed the patient/participant’s PCP with the request and proviso. We also strive to maintain a good rapport and open communication with the Last Gift participants’ entire clinical care team as these are important sources of information about participants in follow-up, as well as referrals of possible future participants.
Legally required autopsy versus rapid research autopsy
On two similar occasions, a potential legally required autopsy was at odds with the participant’s wishes for their body to undergo a rapid research autopsy. In one illustrative case, a participant suffered a fall that resulted in head trauma while hospitalised. This fall could have triggered a legally required autopsy by the coroner if the fall was followed by the patient’s death and the fall contributed to their death. The patient was alert after the fall and concerned that the coroner’s autopsy would effectively exclude them from the Last Gift of which they adamantly wanted to be a part. If necessary, we were planning on having the hospice attending physician notify the coroner that the hospice attending physician did not believe the fall contributed to the patient’s death. In the end, the patient passed away after the 30-day deadline for requiring notification of the coroner of a fall in the hospital leading to death.
It is well known that legally required autopsy takes precedence over research.10 24 In cases such as the one described where the patient/participant is lucid after the fall and directs his body to be donated for a study rather than in a coroner’s inquest, does this ethically blur the black letter of the law? Should one have autonomy over their body in such instances that supersedes administrative legalities? A more robust discussion on this topic involving legal authorities, medical authorities, bioethicists, community members and other stakeholders is necessitated. This topic is outside the purview of this paper and, indeed, of our project. We raise the issue because it is a situation that will, inevitably, come to fruition in the context of future EOL studies. While a legally required autopsy would take precedence,10 it may not preclude a rapid research autopsy to occur. Provisions for legally required versus rapid research autopsy could be proactively written into a research or ethics protocols or evaluated on a case-by-case basis.
Identification of NOK and loved ones
General consensus exists that EOL care and research must focus not only on the participant but also on NOK/loved ones.1 2 25 The definition of each of these terms, however, varies among participants. Indeed, familial arrangements may be different for same-sex loving couples who often bear the greatest burdens of HIV. With PWH, the concepts of non-traditional or chosen family are highly relevant. We should ask participants to define whom they consider to be NOK/loved ones and adopt an inclusive approach. This determination will likely centre around interpersonal and interfamilial dynamics of which the study team may not have insight. For instance, we have had potential candidates who did not want their significant others know they were living with HIV. Further, participant-identified NOK/loved ones should be involved from the consent process forward so that they understand each aspect of the study and can provide support to the participant.1 12 This route, however, should only be followed after the expressed consent of the participant to respect their over-riding autonomy, as tensions may arise between NOK/loved ones and the participant over their participation in EOL research.12 Ongoing consent checks may also be relevant for NOK/loved ones. We recommend NOK/loved ones be a focus of EOL research, but only if participants explicitely consents to such involvement.28 The research team should be respectful of these relationship dynamics.
Issues of inclusion
The AVRC CAB asked if the Last Gift was considering enrolling prisoners with HIV. The topic of enrolling prisoners in medical research is ethically fraught with possible issues of coercion, autonomy and justice.29 The Last Gift is not currently enrolling, or considering enrolling, incarcerated PWH. Indeed, research such as the Last Gift is not legally authorised to enrol prisoners without obtaining special permissions.30 We raise the issue here because, if we are approached by someone specifically, we would not want to deny them the self-fulfilment that often prompts people to enrol in EOL studies1 23 31 32 simply because they are incarcerated.
Likewise, similar discussions are also warranted for other groups who are often under-represented in clinical trials because they pose unique ethical and practical challenges, such as people struggling with homelessness and heavy substance abuse, among others.
The Last Gift team is cognisant that individuas from racial, ethnic and gender-expansive groups have been found to participate less frequently in HIV cure research.33 34 Special efforts are being made to increase their inclusion and representation in the EOL HIV cure research. For example, the Last Gift actively partners with entities serving under-represented populations in research, such as Veterans Affairs and well-respected community-based organisations. The Last Gift maintains a strong commitment to diversity.
Issues specific to the Last Gift
Logistics of body donation and rapid research autopsy
Because the latent HIV reservoir begins to deteriorate immediately after death,14 the window for performing a rapid research autopsy is incredibly narrow, limited in the Last Gift to within 6 hours postmortem.3 7 The research team explains to participants that a rapid research autopsy is crucial to maintain quality of cells, proteins and nucleic acids to perform subsequent analyses. Thus, the research autopsy is highly choreographed and, should anything go wrong, it could jeopardise the potential scientific knowledge to be gained. On one occasion, an enrolled participant was transferred to the intensive care unit. The NOK/loved ones planned to withdraw life support on a day when the autopsy team could not be ready until the following morning. To more easily fulfil the participant’s wish to donate their body after death, we considered asking the clinical care team and their NOK/loved ones to wait until the following morning, but altogether decided against it. We did not feel it was ethically appropriate to interfere with clinical care (which takes precedence over research) and subject the family to more distress, medical costs and disruption for purposes of the study. The feelings and mental health of the NOK/loved ones necessarily must be taken into account and weighed in decisions relating to EOL research.1 2 25 ,2
One way to address the time contraints between death and the rapid research autopsy would be medical assistance in death (MAiD).11 14 Similar to ongoing research efforts in Canada,14 the Last Gift allows MAiD to occur; however, the decision to undergo MAiD must be made outside of the study. In other words, the process of enrolling in the Last Gift must remain independent from the process of seeking MAiD. For example, one participant with amyotrophic lateral sclerosis decided to undergo MAiD to preserve dignity and compassion at the EOL.35 It is possible, however, that Last Gift participants who decide to undergo MAiD on their own are pragmatic about their mortality and their desire to contribute to science.
Disposition of body perceived as study benefit
The disposition of the body after research autopsy may be perceived by some to be a benefit of the Last Gift, which could be ethically problematic.10 12 16 Currently, the cremation costs (or an equivalent amount if burial is requested) is covered by the study. We significantly engaged the AVRC CAB (composed of several ageing PWH in Southern California) with regard to the cremation issue. The IRB initially believed the cremation may unduly influence people to participate. However, after extensive consultation with the AVRC CAB, we felt that providing cremation at no charge was a necessity, given the invasiveness of the research. Cremation is not considered an incentive to participate per say, but a fair compensation for time and burdens,36 and should not be presented as a benefit.3 We are sensitive to the possibility of this being perceived as a deciding factor and are raising it here as a caution to future EOL studies. We attempt to screen Last Gift participants to ensure no undue influence and advise them that disposition of the body after autopsy should not be perceived as a benefit.
Consistent with ethics guidelines with the recently dead,10 the degree of invasiveness of the research autopsy must be minimised and justified in terms of expected scientific benefits. The research autopsy team usually does not touch the face during autopsy to minimise the risk of unanticipated disfigurement. It would be possible to reconstruct the body for an open casket if somebody felt strongly about this. The open casket would be an option if the research autopsy team could know in advance. The participant’s EOL wishes are discussed throughout the study to ensure the body is handled appropriately to meet whatever those wishes are (cremation, closed-casket burial or open-casket burial).
Conclusion
Studies such as the Last Gift promise remarkable scientific advancement and, in many cases, provide participants with a deep-seeded feeling of self-fulfilment. EOL research, however, has long been a taboo subject. If we wish to continue to learn from such innovative research, we must be transparent, willing to learn and willing to share our formative experiences. We hope our lessons learnt and ethical analysis will prove useful to other research teams designing EOL protocols. These critical reflections have implications to protect research participants, to protect research teams, and protect trust and integrity in the clinical research enterprise. While we devised a strategic ethics plan at the start of the Last Gift,3 we could not anticipate ethical and practical issues that would arise. Some of these challenges intersected with clinical care, public health (eg, COVID-19 pandemic) and the law. In an area as novel as EOL HIV cure research, we recommend continued reflection to improve study designs to ensure research remains acceptable to all involved interested parties and the public. We will continue to document and report on the challenges and questions we face in the Last Gift to promote open dialogue about HIV cure-related research at the EOL. Ethical reflections should be complemented with robust empirical research to address and resolve complex ethical issues as they unfold.
Data availability statement
No data are available. This paper details ethical reflections and documented lessons learned. As such, no data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. This paper stems from our own reflections and lessons learned. Thus, this paper did not require institutional review board (IRB) approval. The Last Gift study was approved by the University of California San Diego IRB (project #160563). The participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors JK and KD drafted the initial version of this paper. All authors reviewed the manuscript for intellectual contents. KD, SH and SC-G made substantial revisions to the manuscript. All authors approved the final version of the manuscript. KD is the guarantor.
Funding This study was funded by the National Institutes of Health (5T32AI007384), National Institute of Allergy and Infectious Diseases, National Institute of Mental Health, National Institute of Neurologic Disorders and Stroke and National Institute on Drug Abuse (UM1AI126620), National Institute on Drug Abuse (DP2DAO51915), National Institute of Allergy and Infectious Diseases (P30AI036214 and R01AI147821), National Institute of Mental Health (R21MH118120).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
↵We drafted new protocols for performing the rapid research autopsy: a non-COVID-19 autopsy would be done following normal protocols22 except the lungs, the organs with the highest risk of viral particles and highest potential for aerosolisation, would be processed last to minimise exposure to the study team. In a COVID-19 autopsy, only two medical doctors with fit-tested, approved N95 masks would process tissues by sealing them in transportation containers in the morgue and decontaminating the outside of these containers. The containers would then be transported across the street to laboratory facilities equipped with biosafety cabinets and, there, the tissue would be processed for flash-freezing. Tissue collection was reduced by approximately 33% in a COVID-19 rapid research autopsy to stay within the prescribed 6-hour time limit.22
↵It is of note that requesting a delay in removal of life support is routinely done in the case of organ transplantation, but the costs of intensive care unit (ICU) care are paid by the organ procurement organisation,36 which the Last Gift does not have funds to provide. ICU resources are also usually highly constrained (and particularly more so during the COVID-19 pandemic).
Other content recommended for you
- Key challenges and ways forward in researching the “good death”: qualitative in-depth interview and focus group study
- Learning from stakeholders to inform good practice guidance on consent to research in intensive care units: a mixed-methods study
- End-of-life care for older first-generation migrants: a scoping review
- Using the Clinical Research Network for psychosocial cancer research: lessons learned from two observational studies
- Reconceptualising risk–benefit analyses: the case of HIV cure research
- Dissemination and Implementation Research in Health (R21): PAR-13-054
- New Potential Risk Factor of Heart Disease Reported in NIH-Funded Study
- Developing a pan-cancer research autopsy programme
- We don’t need unilateral DNRs: taking informed non-dissent one step further
- Factors affecting physicians' decisions to forgo life-sustaining treatments in terminal care