Article Text

Abstract
Disproportional morbidity and mortality experienced by ethnic minorities in the UK have been highlighted by the COVID-19 pandemic. The ‘Black Lives Matter’ movement has exposed structural racism’s contribution to these health inequities. ‘Cultural Safety’, an antiracist, decolonising and educational innovation originating in New Zealand, has been adopted in Australia. Cultural Safety aims to dismantle barriers faced by colonised Indigenous peoples in mainstream healthcare by addressing systemic racism.
This paper explores what it means to be ‘culturally safe’. The ways in which New Zealand and Australia are incorporating Cultural Safety into educating healthcare professionals and in day-to-day practice in medicine are highlighted. We consider the ‘nuts and bolts’ of translating Cultural Safety into the UK to reduce racism within healthcare. Listening to the voices of black, Asian and minority ethnic National Health Service (NHS) consumers, education in reflexivity, both personal and organisational within the NHS are key. By listening to Indigenous colonised peoples, the ex-Empire may find solutions to health inequity. A decolonising feedback loop is required; however, we should take care not to culturally appropriate this valuable reverse innovation.
- applied and professional ethics
- education for health care professionals
- minorities
- public health ethics
- quality of health care
Statistics from Altmetric.com
- applied and professional ethics
- education for health care professionals
- minorities
- public health ethics
- quality of health care
Introduction
This article examines healthcare inequities in the UK potentially related to racial discrimination. The 2020 BMJ special issue on racism in medicine1 highlighted a growing interest in this area. The origins of Cultural Safety (CS) in New Zealand (NZ) and the Australian experience are then explored, with the differences between CS and cultural competence described. The ‘nuts and bolts’ of translating CS to the UK as a decolonising mechanism to address equity, diversity and human rights in healthcare are explained.
Ethnic diversity in the UK
Ethnic diversity within the UK has rapidly expanded with 13.8% of the population in 2018 from black, Asian and minority ethnic (BAME) backgrounds2 up from 5.9% in 1991,3 with the majority residing in urban cities, predominantly London, Manchester and Birmingham.4 We do acknowledge the term BAME is currently being debated as whether it is apt terminology for a grouping of darker skin toned people, however, as consensus has not been reached we have used the pre-existing term of BAME in this article in the context of anti-racism. Migration trends are seen worldwide due to social, economic and environmental factors within a country5 often with historical roots in the British empire. From 1971, 100 000 people migrated annually to the UK from Commonwealth countries until the early 2000s. As a long-term consequence of postcolonialism and Idi Amin’s dictatorship, 27 000 Ugandan Asians were forced to immigrate to the UK.6 The advent of the Asian corner shop with the expansion of Pakistani and Indian communities reduced racism and discrimination levels more prevalent elsewhere.7 Nearly half a million economic migrants, known as the ‘Windrush generation’ immigrated to the UK as a result of labour shortages following World War 2. Changes to immigration laws in 2012 led, for some, to threats of deportation and an inability to continue working for or accessing the National Health Service (NHS).8
Health outcome discrepancies in the UK
Alongside the changes to ethnic diversity within the UK over time, there are the ongoing and continuous signs of healthcare disparities between ethnic minority groups and white British communities. Asian women are almost twice as likely to die during childbirth than white women and black women up to five times more likely.9 Diabetes risk is between two to six times higher in South Asian patients compared with white British,10 with increased morbidity and mortality in this ethnic group.11 Admission rates under the Mental Health Act 2017–2018 remained higher than average among BAME groups, especially among ‘Black or black British’ groups who were sectioned ‘over four times’ the rates of white groups.12 Not only are differences seen in health outcomes, but also in healthcare provision and health-seeking behaviours. Internalised stigma was found to be a barrier to accessing support by HIV-positive African immigrants in London, leading to avoidance of non-essential services and reports of being stigmatised as health tourists taking advantage of the NHS.13 There are also unmet needs and inequities when accessing palliative care for BAME groups in the UK.14 Lack of referrals, knowledge about services, structural barriers and previous negative experiences with healthcare provide evidence of poor communication between health professionals and families. Western beliefs, such as autonomy and control over dying, do not always universally reflect the views of different cultures. Enforcing Western beliefs can violate a person’s sense of family and identity, with loved ones unable to fulfil their caring responsibilities.14 Provision of treatment with biologicals in South Asian patients with Crohn’s disease was proportionally lower than white British patients.15 A range of other inequities can be seen in the Race Disparity Audit of 2017 ranging from obesity, emotional problems, to rates of cancer diagnoses.2
The evidence provided thus far are only descriptive studies as there is a scarcity of randomised controlled trials (‘RCTs’) to demonstrate unconscious racial bias in healthcare delivery. Hussain-Gambles et al 16 explain that ethnic minority groups are under-represented in UK clinical trials. However, there is one UK RCT that found implicit bias in dentists’ clinical decisions on tooth restorability, with root canal therapy being recommended to white patients and black patients recommended extractions.17 A prospective longitudinal study18 found poorer health outcomes in UK adults from BAME backgrounds who perceived racial discrimination. A prospectively defined observational cohort study19 that analysed registry data from five acute NHS hospitals in east London, to describe outcomes for people from BAME backgrounds hospitalised with COVID-19 infection, validates Hacket et al’s18 findings. The study identified ‘disproportionate rates of premature death from COVID-19’ in Asian and black patients compared with white patients.19 Despite the fact that people of BAME backgrounds comprise only 20% of NHS staff, 60 out of the first 100 staff to die of COVID-19 were from these backgrounds.20 Could the historical lack of high-quality evidence as well as lack of representation from ethnic minority groups in studies be considered a form of structural racism in itself? In both the USA and the UK, data limitations have greatly hampered investigations of ethnic inequalities in health. Perhaps, foremost of these, is the inadequate measurement of ethnicity, but also important is the lack of high-quality data on socioeconomic position, particularly data that address life course issues.21 The most robust longitudinal evidence from routine national data is found in ‘Health Equity in England: The Marmot Review 10 Years On’.22 Marmot’s review22 demonstrates that over time across the whole population of England, health inequalities have widened overall, life expectancy has stalled, and the amount of time people spend in poor health has increased over the past decade. In fact, the scenario is much harsher for ethnic minority groups who have higher rates of deprivation and poorer health outcomes. A BMJ analysis published early in 2021 by Razai et al 23 details the most recent triangulation of UK evidence regarding structural racism coupled with the effect of COVID-19. However, since the COVID-19 pandemic, the government’s reactionary reports to the raising of awareness of structural racism were initially in line with this accumulating evidence, such as the parliamentary report on ‘Black people, racism and human rights’.24 However, this has recently been disputed by the Sewell Report,25 which minimises structural racism and contends:
Put simply we no longer see a Britain where the system is deliberately rigged against ethnic minorities. The impediments and disparities do exist, they are varied, and ironically very few of them are directly to do with racism. Too often ‘racism’ is the catch-all explanation and can be simply implicitly accepted rather than explicitly examined.
The Sewell Report has given rise to much controversy such as authorship,26 contributorship27 and suggestions of cherry-picking data. As the response to this latest report continues to evolve, it should be noted that, alongside differences in genetics, epigenetics and background risk of certain diagnoses in diverse ethnicities, the way the UK provides westernised services may lead to poorer healthcare outcomes for ethnic minorities.28 Patients still report discriminatory behaviours in healthcare systems, and the COVID-19 pandemic reinforces racism as a social determinant of health.29
Human rights and ethics in healthcare in the UK
Several systematic failures in UK healthcare30 31 have highlighted the need for improved human rights in the National Health Service (NHS). Consequently, human rights principles of ‘Fairness, Respect, Equality, Dignity and Autonomy’32 are recommended to be embedded in the organisational structures of the NHS. Human rights and ethical principles are intertwined in healthcare. Principles such as autonomy of the person and social justice are common to both frameworks and informed by other ethical principles such as non-maleficence and beneficence.33 The importance of human rights and ethics in healthcare also informs the United Nations’ ‘Sustainable Development Goals’.34 However, putting human rights into context requires interpretation through a historical lens on the damaging impact of colonisation and lingering inequities of colonialism.35
The meaning of CS and its origins
Dismantling the discrimination that led to structural racism and other forms of healthcare inequity is crucial to decolonising healthcare.35 CS emerged as a way of overturning individual and structural racism experienced by colonised Māori peoples in NZ and has now been adopted in Australia. CS, as a decolonising intervention, could be translated back to the heart of the ex-colonial empire, the UK. This type of reverse innovation36 may address long-standing structural discrimination behind power imbalances in healthcare. ‘Reverse Innovation’ is a term that has gained footing within healthcare spheres, but the term translates from the process described in management literature37 to something slightly different in healthcare. Harris et al 38 explain that it is essentially about learning from others who have been traditionally subordinate and less powerful. Although the term has previously entailed the innovation moving from a low-income country to a high-income country, in the case of CS, the movement across the power differential refers to colonised marginalised communities within a high-income country providing learning opportunities for more mainstream communities of practice in those same settings. Reverse innovations have the potential to disrupt and improve health systems.
CS could be seen as an ethical antiracist decolonial social justice strategy. Britain as the centre of a previous empire could reflect on the infliction of colonial injustices and learning from past mistakes and ‘make good’ whilst exhibiting cultural humility to learn from those previously colonised who have found solutions. However, it is essential to make sure that there is no cultural appropriation of CS. Humbly learning from low-income countries or colonised people resonates with Berwick’s debate point about ‘Lessons from developing nations on improving healthcare’,39 where he said:
It might help us in the wealthy world to pause for a moment and reflect not on what we lack but on our good fortune. And the best way to do that is to look at those with less in their hands…. We may well find ourselves not the teachers we thought we were, but students of those who simply will not be stopped under circumstances that would have stopped us long ago.
Those in positions of power and privilege are often unconscious of these power imbalances, further contributing to mortality and morbidity in healthcare. From an ethical perspective, CS offers a way of addressing social justice and aligns itself with the ethical principles of beneficence by helping those who are the recipient of health inequalities; promotes and facilitates health maximisation for all; and respect for autonomy by embodying patient centred care. CS exposes implicit and structural biases, therefore asserting non-maleficence.33
CS is distinct from cultural competence in that it acknowledges inherent power imbalances between clinician and patient. The inclusion of self-reflexivity, historical and social dynamics and recognition of white privilege validates CS healthcare as the more effective approach than cultural competence in achieving health equity and reducing discrimination within healthcare. The differences between CS and cultural competence are illustrated in table 1.
Comparing and contrasting Cultural Safety and cultural competence 40
The epistemological origins of CS stem from the negative impacts of colonisation on Māori people in Aotearoa/NZ. Cultural competence has a number of contexts and definitions, from a variety of sources and relies on practitioners’ ability to acquire the knowledge, values and skills required in delivering healthcare to people from minority and/or vulnerable ethnic groups.40 Disagreement remains on how to operationalise, evaluate and apply varying concepts of cultural competence in health and social service settings.41 The term cultural competence is frequently used interchangeably with a variety of terms used for working with patients in cross-cultural settings (see table 1). These terms are at risk of becoming the focus, rather than the rationale for them. CS, on the other hand, clearly states the rationale of increasing health equity for minority groups by urging individual professionals to examine their own position of privilege and the need to examine and address inherent power imbalances in therapeutic relationships and encounters. Health practitioners must examine themselves and the potential impact of their own culture on clinical encounters. To do this they must be aware of difference and consider power relationships via reflective practice. Allowing the patient to determine whether a clinical encounter is culturally safe is a key component of CS that is missing from the cultural competence approach.40
The NZ experience
In Aotearoa/NZ, the birthplace of CS, we still see headlines such as ‘Māori babies less likely to be resuscitated, bias blamed’. According to the latest Perinatal and Maternal Mortality Review Committee,42 institutional bias or implicit biases are implicated.
The concept of CS arose out of a nursing education leadership hui (meeting) held in 1989. A Māori nursing student stood up and spoke her truth:
You people talk about legal safety, ethical safety, safety in clinical practice and a safe knowledge base, but what about Cultural Safety?43
Members spoke of challenging inherent institutional racism, increasing disparities, ill health and well-being of Māori in a neo-colonial context. An ensuing body of work undertaken by Māori nurse and educator, Irihapiti Ramsden, led to her realisation that student and graduate midwives and nurses could not connect the impact of colonisation to ill health and disparities for Māori. Ramsden recognised that midwifery and nursing education needed to incorporate the concepts of CS.43 In 1988, all nursing and midwifery education schools in Aotearoa/NZ were required to demonstrate their commitment to Te Tiriti o Waitangi.1 They did this by embedding a CS educational model and pedagogy.43–45 Ramsden argued the words ‘Cultural Safety’ should always be presented in upper case to emphasise it as a process, one which has a real place in health practice and education.43
An essential element of CS is undertaking self-reflexivity,43 a process of understanding one’s own culture and the inherent power in relationships. CS is about ‘you’; it is concerned with seeing the uniqueness of the individual you are interacting with and respecting difference. It is about replacing and demystifying colonial history and having an appreciation of the impact of colonisation on health and well-being. It is acknowledging that racism exists and has no place today. CS is also political and informed by power relations. Any attempt to depoliticise CS is to misunderstand any of its key points.43 44 47
Ramsden advised non-Indigenous academics who have experienced professional development can teach CS, however, not when the topic is directly related to the subjective experience of being Indigenous.43 48 A critical element of CS is that the recipient of care/education defines and decides whether ‘care’ or the experience is safe for them.43 44 49 50
One of Ramsden’s biggest fears was that CS would evolve into something else. A complex timeline of political events and lack of understanding from Pākehā2 about what honouring the principles of Te Tiriti o Waitangi means for Māori, health equity has colonised the term. CS has morphed into less politically contentious terms such as ‘cultural awareness’, ‘cultural sensitivity’ or ‘competence’. The recognition of power differentials within society and critical self-reflection by health professionals has been lost. Challenging conversations about racism have been diluted with history told from the perspective of the coloniser. Facing up to the impacts of colonisation and achieving equity, as Ramsden feared, had been forgotten.51 52
Thirty years on, with deeper understanding and commitment, we have begun to revisit CS in Aotearoa/NZ. In a recent publication, Curtis et al 40 recommend an approach to CS across all health professions that encompasses the following core principles:
Achieving health equity that is measurable.
Centred on concepts of CS and critical consciousness and not cultural competency.
Mandated CS professional development.
CS accreditation at an institutional level.
Health outcomes and systemic monitoring of CS.
CS be acknowledged as an independent requirement and expectation for competency (p. 15).
If we embrace and integrate these core principles, there is potential for health professions in Aotearoa/NZ to lead the way and transform the health experience for Māori and other Indigenous populations.
CS from an Australian perspective
Australian Aboriginal and Torres Strait Islander People experience the worst health inequities of any cultural group in Australia and are more likely to die before they are old.53 Healthcare for Indigenous Australians3 is constrained by institutional racism.54–56 The true story of violence and racism under which Australia was colonised is missing from school curricula. This ignorance has enabled white Australians’ denial of history within a culture of systemic and individual racism, fuelled by negative media representation of Australia’s First Nations Peoples.57 Since the early massacres and removal of tribal groups into institutions and prisons, successive governments have attempted to eliminate Indigenous culture and language.58 Lack of recognition and acknowledgement of colonisation as the origin and ongoing cause of ‘epidemic’ proportions of chronic disease and early mortality experienced by First Nations Australians contribute to high levels of victim blaming and ‘othering’ by health professionals within healthcare.59 60
CS is informed by a postcolonial lens that critically explores issues of power imbalances and social inequities, aiming to achieve systemic change by confronting stereotypical assumptions as the tools of dominant systems and structures.61 CS aims to ensure that First Nations Australians’ cultural and treatment preferences are upheld and respected within health systems.62 The principles of CS are interconnected and central to delivery of acceptable healthcare to all recipients outside the dominant culture of any nation. In Australia, critical reflection by healthcare professionals, on their own white privilege and the ongoing impacts of transgenerational trauma, originating from colonisation and power imbalances, is essential to reducing First Nations Australians’ health inequities. Failure to do so alienates Indigenous Australians, reinforcing barriers to acceptable and accessible healthcare and validates the dominance of the colonisers.63
Unlike the Māori experience in NZ/Aotearoa, Aboriginal and Torres Strait Islander peoples have neither a treaty nor a voice in the Australian constitution and parliament. Australian government rhetoric resonates strongly with the current controversy in the UK over the Sewell report,64 where parallel arguments are being used to deny systemic racism and dismiss or downplay black and ethnic minority people’s voices and concerns. CS has a crucial role in building health services that can deliver greater health equity and access in both countries, where the same conversations are currently being had.
Given the substantial evidence of racial discrimination, could we translate the decolonial intervention of CS to the heart of the postcolonial empire?
The taxonomy of CS translation to UK
For the translation of CS to the UK, we have developed a scaffolding model to assist readers. We use the tree model as both a practical taxonomy but also as a metaphor that symbolises and resonates with its Indigenous ideals.
CS tree model
The nuts and bolts of translating CS to the UK are now considered. The model of the process is illustrated in an infographic (figure 1). This model has three essential parts:
The three roots of this model stem from NZ and involve understanding experience of care, self-reflexivity and structural reflexivity in the context of understanding power imbalances causing biases and privileges.
The tree trunk represents the core values of human rights and is symbolic of the nurturing and humanistic approach to healthcare and the need for institutions to commit to examining and upending structural bias.
The allegory of the branches, leaves and flowers relates to activities or services that pre-exist in the UK and are either budding or well developed and can be incorporated into a CS model.
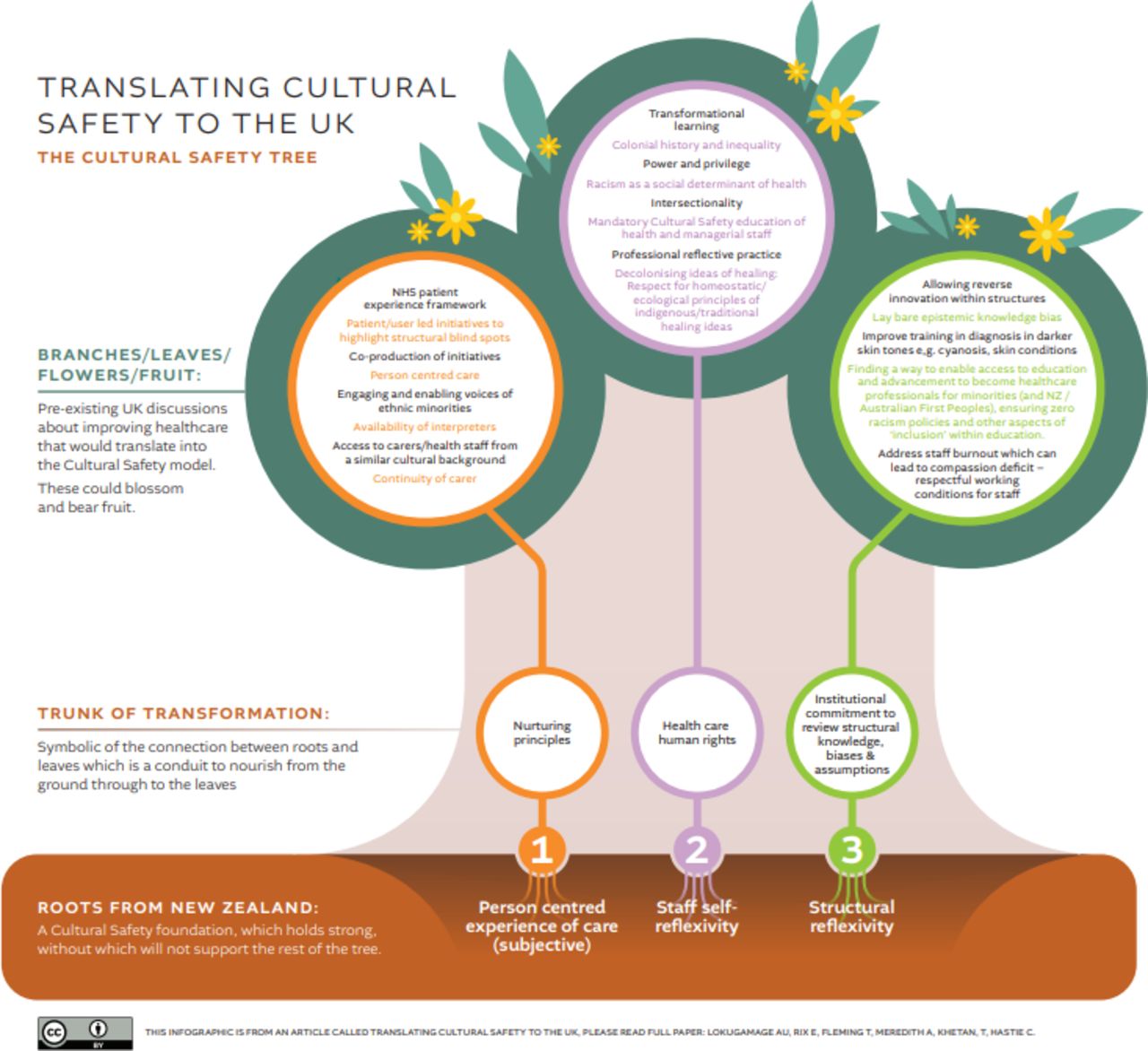
{kind=link}
Infographic of the Cultural Safety tree.
The translation will involve healthcare education and absorption in healthcare policy. However, educational curricula and health services need to acknowledge the key points as illustrated in the CS tree and adapt them into their local syllabi and healthcare guidelines. We do not recommend a ‘one size fits all’ approach, and the utilisation of the concepts raised in this paper and our infographic will ultimately be bespoke to the target organisation. Because the information is complex, for readers who are not visual learners, we have also included the same information in table form (table 2) within this paper and discussed the elements further in the next section of the paper. Table 2 is colour coded to match the infographic.
The Cultural Safety tree in table format
Translating CS and dovetailing with pre-existing healthcare human rights, ethics and decolonial activity within the UK
There is already much happening in the UK that is oriented towards a CS approach, just not yet explicitly stated as such. We have located examples of these efforts in the UK and refer to them in the context of CS themes. We have listed them broadly under nurturing principles, healthcare human rights, ethical considerations and institutional commitment to review structural knowledge, biases and assumptions. The themes we have identified weave and interlock around those principles but are tailored to the UK situation. However, translating CS to the UK using our suggested taxonomy would provide a unifying conceptual approach but the UK would have to acknowledge its origins and the trajectory of this Indigenous healthcare reverse innovation.
Active listening to user and staff experience with cultural humility
From the perspective of overturning racism in healthcare, it is paramount that healthcare providers listen through public engagement to the subjective experience of ethnic minority peoples experiencing healthcare inequity. In the UK, top-down initiatives exist regarding listening to patient experience.28 65 66 Equally bottom-up initiatives are important to address healthcare structural blind spots.67 It is from these conversations that priorities should be distilled by codesign. Educating healthcare providers to listen to topics that critique healthcare provision can provoke defensive reactions. Thus, it is imperative that healthcare providers be educated in active listening,65 with transformational learning methodology, to facilitate cultural humility when listening to the stories of patients to maximise the benefit from public engagement. In the underfunded NHS, where ‘burnout’68 is reported by workers, the absence of cultural humility and active listening may be a symptom. Both patient and staff experience reflect systemic overload. We suggest that restorative justice processes inherent in CS may reduce conflict between staff and patient groups.69
Interpreters must be available
Adequately funded interpreter services are vital for communication between individuals and their care providers.70 Miscommunication can impact on morbidity, mortality and evaluation of healthcare experiences. Inadequate or culturally unsafe care alienates and disadvantages healthcare consumers. However, CS enhances accessibility of healthcare for ethnic minorities. Good examples of consumer experience using interpreters and performance art are increasing in the UK, including coproduced projects highlighting ethnic voices on their experiences of maternity care.71 This work is helping to expose structural blind spots.
Addressing racism towards staff
In NZ and Australia, where Indigenous peoples have been colonised by white invaders, access to healthcare staff from similar racial backgrounds is the ‘pinnacle’ of CS in addressing racism in healthcare. However, there is a different dynamic in the UK, where BAME communities have migrated to take up residence within a country with a white population. From UK census data of the general population, the proportion who identify as white British has decreased from 94% in 1991 to 86% in 2011.72 Government statistics show that four out of five (79.2%) NHS staff (whose ethnicity is known) are predominately white.73 There was a higher percentage of staff from BAME groups in medical roles than in non-medical roles. Kline’s BMJ blog74 explores the ‘double-edged’ sword of white patients wanting to see white doctors and displaying racism towards doctors of ethnic minority groups. There is also CS activism in maternity care in response to the appalling maternal mortality in the UK to support pregnant women with carers from similar ethnic backgrounds.75 However, carers from similar backgrounds may not necessarily display the kindness and compassion needed for culturally safe healthcare in the UK. As the goal of translating CS to the UK health system is to replace racism with humility, respect, kindness and compassion for all, the implementation of continuity of empathetic care models may be a solution. Continuity of empathic care has been found to reduce stress, increase feelings of control and improve outcomes.76–79 Another form of discrimination is explored by Woolf.80 The paper exposes the lack of progression and opportunities in the careers of BAME graduates across the disciplines. This resonates with obstacles recognised in the original aspirations of NZ’s CS model: to enable more Indigenous healthcare providers to be educated. With no evidence-based solutions for this phenomenon, it is an area requiring future research across all areas of higher education in the UK.
Epistemic knowledge bias
Biomedical knowledge has limitations, being derived from the conceptual framework from the global north. This is known as geographical bias.81 This creates an epistemic bias for the knowledge base of medicine that disadvantages traditional ‘healing knowledge’ and research exploring health derived from the global south. Healthcare structure should not be disrespectful of Indigenous knowledge of health and homeostasis. The decolonising framework critiquing biomedicine’s medical hegemony must be part of decolonial education.35
Decolonising history of healthcare within training
In the UK, decolonial healthcare history has been omitted from medical, nursing and midwifery education, so syllabi need to be developed. Such curricula should insist on the opportunity to hear/privilege the voices/stories of those colonised and therefore demonstrate the impact of colonisation. User/patient voices and stories of lived experience potentially enhance compassion and empathy.66 Crucially, education in self-reflexivity regarding power and privilege as a part of reflective practice needs to be prioritised. Nursing and midwifery education curricula in NZ and Australia have models of reflection that include self-reflexivity and considerations of power.82 While the General Medical Council is constantly updating its reflective practice advice, it has yet to include reflections on power and privilege.83 Such learning is vital to creating lasting emotionally intelligent behavioural change.
Decolonising diagnostic bias
A significant area to address is the lack of teaching materials related to diagnosis in darker skin tones where traditional pictorial resources have focused on white skins.84 For life and death situations, traditional medical syllabi do not teach how to diagnose cyanosis in a black person for instance.85 However, innovations are afoot to address this such as Mukwende’s handbook of clinical signs in black or brown skin called ‘Mind the Gap’.84 This, or similar resources, will need to be propagated to healthcare training to reduce morbidity and mortality from misdiagnosis in darker skins. Teaching about pathologies in ethnic minorities needs to be done without racial discrimination. Ideally, racially tailored diagnostic practices, such as serum biochemical values, should be rigorously critiqued and mediating variables, such as epigenetic changes or ‘weathering’ due to structural social adversity, should be analysed and taken into account.29 86 If this is not done, this may lead to assumptions about biological determinism as well as under or overdiagnosis of pathology in ethnic minorities.
Conclusion
The history of racial discrimination in the UK is contextually different from antipodean countries that have developed CS frameworks from the voices of Māori and Aboriginal and Torres Strait Islander peoples. Any translation to the UK, whose ethnic minorities stem from immigration, will be different. However, care must be taken, as with any reverse innovation, that this innovation must not be culturally appropriated. The Indigenous origins of this human rights innovation must always be recognised and acknowledged.
Educating healthcare providers to be culturally safe, by exploring, weaving and using the elements of the CS tree in practice are the ‘nuts and bolts’ of translating it to the UK. In doing so, institutions should create tailored CS training depending on the syllabi or organisational structure and resources. We cannot be prescriptive about the precise educational format due to heterogeneity of target organisations. Each of the elements could work through facilitated workshops, patient public involvement and coproduction of education, health services and development of structural institutional policies. Translating CS to the UK in the manner presented would also satisfy the human rights agenda and ethical responsibilities for the provision of healthcare. We would hope that further research to evaluate such CS programmes will form a growing evidence base of this possible reverse innovation over time. These are all stepping stones to overturning structural racism.
Supplemental material
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank Teresa Krishnan, Māori Liaison Lead, AUT, Aotearoa/NZ and Darlene Rotumah, a Bundjalung woman from Fingal Heads, New South Wales, Australia, for their valuable assistance in creating this paper. Dayal Pathberiya’s assistance with cultural safety tree in table 2 is also acknowledged.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Docamali, @tania_fleming2016, @CarolynHastie
E(L)R and TF contributed equally.
Contributors AUL conceived the idea of the paper and contributed to the manuscript. Both ER and TF contributed to the manuscript as joint second authors. CRH contributed to the manuscript, TV and AM both contributed to the manuscript. All authors drafted the work or revised it critically for important intellectual content, approved the final approval of the version published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AUL is on the Board of Directors of the International MotherBaby Childbirth Organisation and also a member of a Patient & Public Voice Partners level 3 advisory group in NHS England (both roles are voluntary with no financial interests). TF, ER, AM, TK and CRH have no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
↵The Māori of Aotearoa/New Zealand’s founding document. It takes its name from the place in the Bay of Islands where it was first signed on 6 February 1840.46
↵Pākehā, derived from ‘Pakepakeha’, is a mythical human-like being with fair skin and hair. Originally, the Pākehā were the early European settlers; however, today ‘Pākehā is used to describe any peoples of non-Māori or non-Polynesian heritage. Pākehā is not an ethnicity but rather a way to differentiate between the historical origins of settlers, the Polynesians and the Europeans, the Māori and the other.
↵The authors use the term Aboriginal and Torres Strait Islander people as the respectful and inclusive term for Australia’s First Nations Peoples. However, the term Indigenous Australians is also used to enable the complexity of this topic to be adequately discussed in this paper.
Other content recommended for you
- Anti-racist interventions to reduce ethnic disparities in healthcare in the UK: an umbrella review and findings from healthcare, education and criminal justice
- Decolonising ideas of healing in medical education
- Racial differences in management and outcomes of acute myocardial infarction during COVID-19 pandemic
- Mitigating ethnic disparities in covid-19 and beyond
- Diversity matters: the other doctor within the Dutch academic healthcare system
- Systematic review of Indigenous cultural safety training interventions for healthcare professionals in Australia, Canada, New Zealand and the United States
- Access to health care for ethnic minority populations
- Experimental studies testing interventions to promote cultural safety, interculturality or antiracism in healthcare: protocol for a systematic review
- Post-COVID-19 paediatric inflammatory multisystem syndrome: association of ethnicity, key worker and socioeconomic status with risk and severity
- To be, or not to be BAME, in the time of COVID-19: does it matter?