Article Text

Abstract
Objective Physical and mental well-being are threatened by climate change. Since hospitals in high-income countries contribute significantly to climate change through their greenhouse gas (GHG) emissions, the medical ethics imperative of ‘do no harm’ imposes a responsibility on hospitals to decarbonise. We investigated hospital stakeholders’ perceptions of hospitals’ GHG emissions sources and the sense of responsibility for reducing GHG emissions in a hospital.
Methods We conducted 29 semistructured qualitative expert interviews at one of Germany’s largest hospitals, Heidelberg University Hospital. Five patients, 12 clinical and 12 administrative employees on different levels were selected using purposive maximum variation sampling. Interviews were transcribed verbatim and analysed using the framework approach.
Results Concerning GHG emissions, hospital stakeholders perceived energy and waste as most relevant emission sources followed by mobility. Climate change mitigation in general was considered as important. However, in their role as patients or employees, hospital stakeholders felt less responsible for climate change mitigation. They saw providing best possible medical care to be the top priority in hospitals and were often concerned that patients’ health could be jeopardised by climate change mitigation measures.
Conclusion Perceptions of most important emission sources did not coincide with those in literature, highlighting the need to inform stakeholders, for instance, about pharmaceuticals as important emission source. A frequently perceived conflict between reducing emissions and providing high-quality medical care could be eased, if reducing emissions would not only be justified as a contribution to mitigation, but also as a contribution to preventing ill health—a basic principle of medical ethics.
- Environment
- Ethics- Medical
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Worldwide, anthropogenic climate change is increasingly impacting physical and mental health. Heat-related deaths, allergic diseases or post-traumatic stress disorder due to extreme weather events, are examples of the many health impacts.1 The health sector, and hospitals as part thereof, are seen as key to adapting to these health impacts. In contrast, hospitals’ role as an important emitter of greenhouse gas (GHG) emissions and thus a potential contributor to mitigation is less well known and hardly on the political agenda.2 4.4% of global3 and 6.7% of German GHG emissions4 are estimated to stem from the health sector, including GHG emissions related to energy and upstream and downstream processes, for example, along supply chains and disposal of medical instruments or pharmaceuticals. Hospitals account for about one-third of these GHG emissions.4 Thus, hospitals do not only protect people from negative health impacts of climate change, but also contribute to worsening them.
The Paris Agreement, ‘potentially the strongest health agreement of the century’,5 aims at limiting global warming to 2°C and even calls for efforts not to exceed 1.5°C.6 Medical associations endorse this aim and see a responsibility to reduce the health sectors’ GHG emissions based on ethical premises.7 Medical ethics considerations are often based on four principles: autonomy, beneficence, nonmaleficence and justice.8 If the health sector does not respond to climate change, it fails at least to meet the last three of these principles: beneficence, by failing to preserve people’s health now and in the future; non-maleficence, by failing to prevent climate change-related harms; justice, by increasing (global) inequities, for instance, resulting from which populations cause the most GHG emissions and which populations suffer the most from climate change impacts.9
The transformation towards climate-neutral hospitals requires the engagement of various hospital stakeholders, such as doctors, administrators, nurses and patients.10 Stakeholders can be considered ‘any group or individual who can affect or is affected by the achievement of the organisation’s objectives’.11 Most doctors are aware of the anthropogenetic nature of climate change and related health consequences.12 However, hospital stakeholders’ perceptions of relevant GHG emission sources in hospitals has received little scientific attention so far. Meanwhile, it is a prerequisite that stakeholders develop environmental awareness in the hospital context to make informed decisions about mitigation measures.13
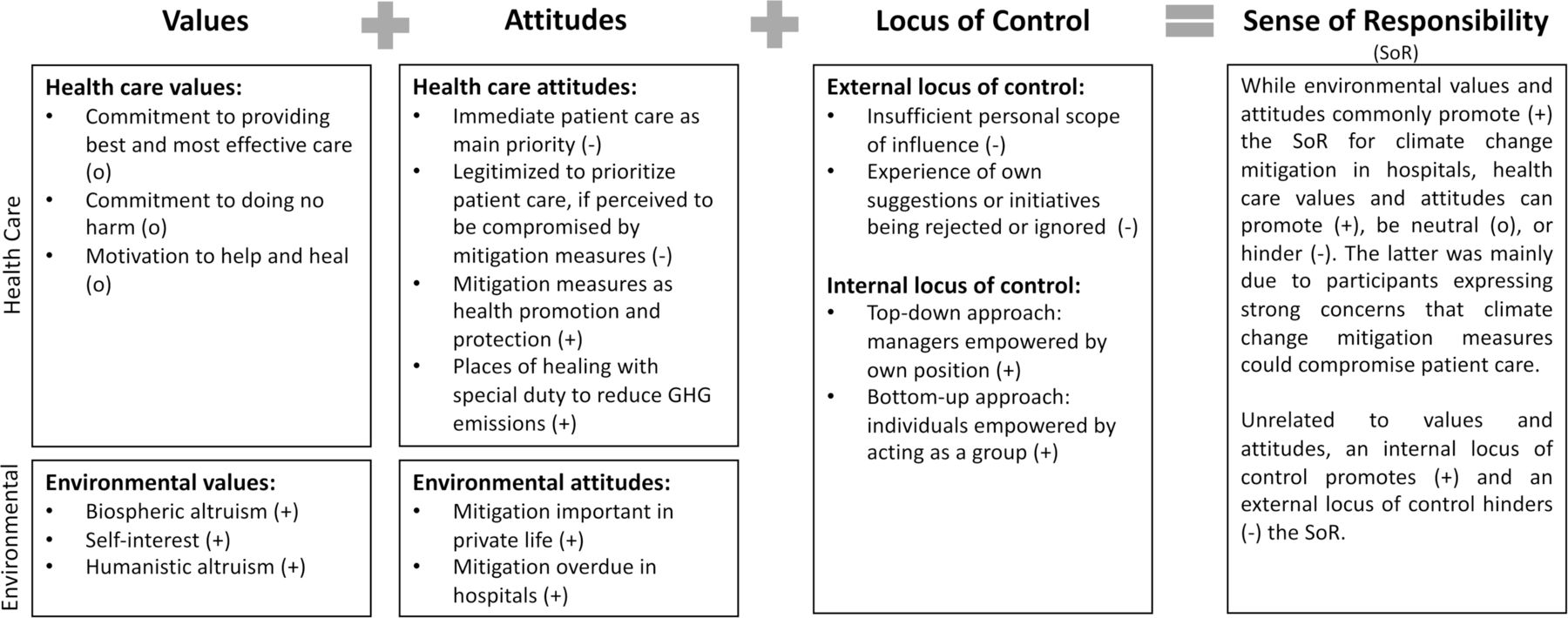
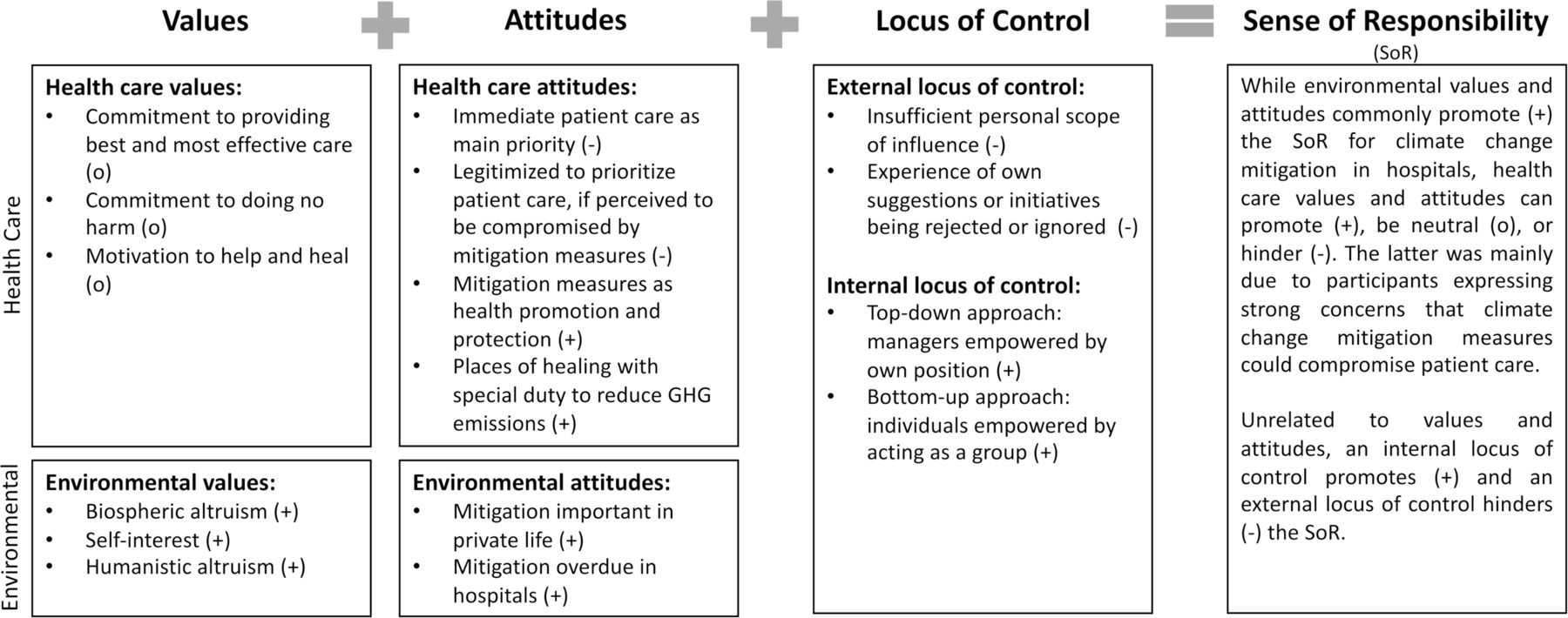
Beyond perceptions of emissions, the sense of responsibility also is important: do hospital stakeholders feel responsible for reducing GHG emissions in the hospital they are affiliated with? Few studies have raised this question to date.14–16 Personal and operational aspects shape the sense of responsibility for environmentally friendly behaviours. These aspects comprise values, attitudes and locus of control.13 More specifically, values are personal or commonly accepted principals and judgements about what holds importance in life.17 Attitudes describe persistent positive or negative feelings towards a topic.13 Regarding healthcare, specific values and attitudes are those underlying practices of empathetic, safe and ethical care.18 Regarding the environment, values and attitudes are those that guide human behaviour towards the environment.19 Locus of control represents a person’s perception of having (internal locus of control) or not having (external locus of control) the ability to effect change through the own behaviour.13
The urgency to address climate change is great.1 While the English National Health Service is leading by example, aspiring a net-zero health system by 2045,20 this issue is less present in the German health sector. Thus, this study aimed at examining hospital stakeholders’ perception of the main sources of GHG emission and characterising their sense of responsibility for climate change mitigation (hereafter: mitigation) in a German hospital.
Methods
Research design
We conducted semistructured qualitative expert interviews21 with stakeholders in one of Germany’s largest hospitals, Heidelberg University Hospital. The study is part of a broader research project at this hospital, which assesses GHG emissions and implements mitigation measures.
Sampling and recruitment
A purposeful, maximum variation technique was applied.22 Based on literature search and team discussion, we wanted to reach maximum variation in the sample regarding participants’ function in the hospital, age and gender (online supplemental appendix 1). Recruitment took place from November 2020 to March 2021. To recruit employees, 50 administrative and clinical employees were identified via the website of the studied hospital and contacted by email. Reminders were sent via email. The response rate was 48% (24 clinical and administrative participants). Administrative stakeholders were chosen according to their responsibility for areas related to the hospital’s GHG emissions based on literature.20 23 Contacts to upper management positions were partially provided and facilitated by a contact person in a middle management position. To recruit patients, we contacted 19 self-help groups affiliated with the hospital via email. We thus recruited five participants who were inpatients or outpatients of the studied hospital. Recruitment on site was not possible due COVID-19-related constraints.
Supplemental material
Expert interviews
Expert interviews were conducted using a semistructured interview guide (online supplemental appendix 2). The interview guide covered three main themes: General attitude towards mitigation, perception of hospitals’ GHG emissions and main emission sources, enabling and hindering factors for mitigation measures in this hospital. Questions addressed GHG emissions, not broader environmental impacts.
With regard to the perception of GHG emission sources, categories and subitems were created inductively; qualitative data were counted and reflected with numerical data in the results to illustrate trends.
After exploring participants’ perceptions of emission sources in open questions, they were shown data on main sources of GHG emissions of the English ‘National Health Service’ (online supplemental appendix 3): energy including fuels and electricity (16%), medical instruments and equipment (13%), pharmaceuticals (12%), mobility of patients, staff, visitors (11%), food and catering (6%). We informed participants that NHS data refers to the entire healthcare system and not specifically to hospitals.
As part of the enabling and hindering factors, the sense of responsibility was discussed. Further results about enabling and hindering factors regarding mitigation measures will be reported elsewhere.
Data analysis
Interviews were audiorecorded and transcribed verbatim, supported by the software ‘f4x’.24 Data were analysed using the framework approach,25 a qualitative content analysis technique for applied policy research comprising five steps: By transcribing and reading the interviews, the familiarisation (step 1) was accomplished. While analysing the data, a thematic framework was developed (step 2) and the transcripts were indexed (=coded) (step 3) using the software ‘NVivo’.26 An overview of the data was obtained through charting them (step 4). Finally, the data were mapped and interpreted (step 5). A second person performed steps 1–3 independently for three interviews to triangulate the main investigator’s codes. In steps 4 and 5, senior investigators were closely involved to discuss the data and their abstract levels of meaning. While the analysis process was mainly conducted inductively, a deductive framework with the categories ‘attitudes’, ‘values’ and ‘locus of control’ was applied to the theme of ‘sense of responsibility’ as it proved suitable to structure the data in a meaningful way.13 The subcategories for values were also applied deductively.18 19
Results
Sample description
Our sample consisted of 29 stakeholders: five patients, twelve administrative and twelve clinical employees. Clinical employees included six nurses, five doctors and one pharmacist. For more details see online supplemental appendix 4.
Data saturation was reached after 26 interviews.27 We conducted three more interviews to ensure that no additional themes emerged. On average, the interviews took 37 minutes. Four interviews were conducted in person, seven by telephone and 18 used video conferencing tools, given COVID-19-related restrictions during data collection. Three participants did not consent to audiorecording, so notes were taken during these interviews instead.
Perceptions of hospitals’ GHG emission sources
Table 1 presents the overview of emission sources and related subitems mentioned by participants. Almost all participants stated, they had never thought about GHG emission sources in hospitals before the interview. Nonetheless, this topic was seen as interesting and helpful.
Emission sources and subitems mentioned by the participants (created by the authors)
Energy and waste were not only perceived as main emission sources when participants were asked directly but were also recurring themes throughout the entire interviews. Energy was considered an obvious emission source. Few participants distinctly referred not only to GHG-related impacts of waste, but also to harmful presence of waste in the nature. Waste, especially packaging waste and the disposal of disposable medical instruments, were prominent because of their tangibility, visibility and increase in daily hospital life:
When I look at the garbage we create in one day in one shift, I work in an intensive care unit, and what we create there in one shift in one day: It’s always whole bags full of it. And it’s INSANE. (B2, clinical staff, female, 29).
Although the use of disposable medical instruments was not appreciated, it was often seen as necessary for patient safety:
Yes, but there are quite a lot of disposable materials, materials that end up in the patient’s body, that somehow get inserted into the skin like catheters. That will never be changed. (B13, clinical staff, male, 36).
However, there were also disposables whose use was perceived to be incomprehensible; these were disposable, which usually are not in direct patient contact or at least not in contact with wounds (eg, laundry bags, tourniquets). Many participants mentioned they attempted to reduce packaging waste in their private life and saw waste as a publicly discussed topic associated with negative emotions:
A huge, huge issue, HUGE issue. We're choking on garbage. (B15, clinical staff, female, 57).
Other emission sources were mentioned less often.
Participants frequently commented on the shown NHS data, but not necessarily on all five emission sources. Participants’ reactions were assigned to three inductively created categories: ‘expected’, ‘unexpected, but comprehensible’ and ‘surprising’ (see table 2). While emissions related to energy and medical instruments and equipment were generally expected, some participants commented that they tended to overestimate their share of total emissions. Regarding mobility emissions, some participants had not expected them to be part of hospitals’ emissions, because they found them to occur outside of hospitals’ premises. Particularly pharmaceuticals were often perceived as a surprise, because participants said they had never thought about this before.
Participants’ reactions to the English National Health Service (NHS) data on the health sector’s GHG emissions (created by the authors)
Sense of responsibility to reduce GHG emissions
Considerations regarding participants’ sense of responsibility to mitigate climate change in their current role as hospital stakeholders was an important theme emerging early during the first interviews as part of enabling and hindering factors. Thus, the interview guide was expanded to include explicit questions about the sense of responsibility. The initial participants were not re-interviewed because the interviews had already sufficiently covered it.
Most participants perceived a sense of responsibility for mitigation in the hospital to some degree. The sense of responsibility (figure 1) is shaped by values, attitudes and locus of control, as described in the introduction.13 Values and attitudes related to both healthcare and the environment were strong among participants. However, they often seemed to clash, when discussing mitigation measures in the hospital. Responsibility to pursue healthcare values and attitudes was prioritised in their role as hospital stakeholder. The sense of responsibility for mitigating climate change in the hospital was further weakened by the prevailing perception of not being able to influence action (external locus of control).
{kind=link}
Hospital stakeholders’ sense of responsibility to reduce GHG emissions in the studied Hospital (created by the authors). GHG, greenhouse gas.
Next, we will describe participants' healthcare and environmental values and attitudes as well as their locus of control more specifically.
Values
Healthcare18 and environmental19 values were mentioned, when talking about the sense of responsibility regarding mitigation in general and in the hospital (table 3). Some quotations already hint at potential conflicts between healthcare and environmental values. This will be discussed in detail in the attitudes section.
Codes and illustrative quotes regarding healthcare values and environmental values (created by the authors)
Most participants expressed several of the healthcare values shown in table 3. One participant assumed that health professionals are particularly willing to mitigate climate change because their motivation is to help people, but that they usually help immediately and not in a future-oriented way as in the case of mitigating climate change. About half of the participants indicated a sense of altruism towards ecosystems or other species (biospheric altruism), which was often directly or indirectly related to mitigation. Some expressed a self-interest in mitigation. It was rare, that a sense of altruism towards all humanity was addressed (humanistic altruism).
Attitudes
Attitudes illustrated in this section address the issue of mitigation in the hospital more specifically than values (table 4). Stakeholders often perceived best patient care and mitigation as conflicting aims (eg, infections from reusable medical instruments, limited medical imaging if energy consumption had to be considered). Immediate patient care, currently COVID-19, was mentioned as unchallenged priority. Thus, GHG emissions were partially considered as unavoidable and participants felt legitimised to not prioritise mitigation in hospitals due to the higher aim of patient care. Only very few participants, who had already been engaged in the climate change and health movement, saw hospitals as places of healing with a special moral obligation to combat climate change. Participants very rarely addressed health cobenefits of mitigation measures, negative health impacts of climate change, and that hospitals could help reduce the latter by implementing mitigation measures. An example for health cobenefits of mitigation measures is evidence-based prescription of pharmaceuticals, which can reduce GHG emissions as well as potential side effects in patients.28 When approached about evidence-based prescribing, participants named health benefits as reasons for interventions already implemented but were not making the connection to mitigation.
Codes and illustrative quotes regarding healthcare and environmental attitudes (created by the authors)
On the other hand, the environmental attitudes identified show that most participants payed attention to mitigation in their private life. Therefore, most participants also felt that mitigation in hospitals was important and overdue.
Locus of control
Participants often addressed whether they have the ability to influence the implementation of mitigation measures through their own behaviour.
Frequently, participants perceived no opportunity to advance mitigation at the hospital (external locus of control). They described an insufficient personal scope of influence, for example, ‘SUPER little room for manoeuvre’ regarding vegan food offers for patients (B2, clinical staff, female, 29). Moreover, they reported that suggestions were rejected or ignored by higher management levels.
Few participants expressed that they felt able to initiate small mitigation measures at the hospital when forming a group of like-minded (internal locus of control). One participant in a high management position described feeling empowered by his position to ‘simply open the doors [for mitigation measures]’ (A11, administrative staff, male, 55).
Discussion
Strengths and limitations
This study is the first to comprehensively explore stakeholders’ perceptions of emission sources and responsibility to mitigate climate change in a German hospital. The qualitative design and focus on one hospital do not allow to generalise the results. But as results correspond to findings in literature, it seems feasible to transfer them to similar contexts.
Overall, different stakeholder groups in the sample showed similar results. However, due to the small sample size, an analysis of subgroups was not possible and could be subject to further research. Also, we cannot rule out any form of social desirability bias.
Due to the COVID-19 pandemic, interviews had mainly to be conducted via videoconferencing systems or telephone, which was shown to be a good alternative to face-to-face interviews.29
Raising awareness for the amount and sources of GHG emissions in the health sector
Although the health sector contributes to 4.4% of net global GHG emissions,3 little attention has been paid to mitigation in the health sector compared with other sectors.30 This was also reflected in our sample, as most participants were unaware of how hospitals contribute to climate change: While the majority perceived energy and waste as main emission sources, scientific results show that medical goods and energy, followed by pharmaceuticals, are the main ones.23 31 Awareness of enormous amounts of hospital waste and desires to reduce it are also found in other research.32 However, focusing on GHG emissions, waste contributes relatively little.31 Waste has many other detrimental impacts on ecosystems and biota that were indicated by participants but were not a focus of this study and will not be discussed further here. A quantitative study among medical, nursing and physician assistant students showed that the health sector’s GHG emissions and the burden of disease linked to the health sector’s pollution are usually underestimated.33
As known from health innovation implementation, hospital stakeholders have to perceive a need for innovation in order to implement changes.34 Regarding mitigation in hospitals, stakeholders’ perceptions of main GHG emission sources are essential for effective action13 35: If, as in the case of our participants, the contribution of certain emission sources is overestimated (eg, waste), there is a risk that mitigation measures with little GHG saving-potential will be implemented. Consequently, awareness and knowledge of hospitals’ contribution to climate change must be increased, for example, through compulsory integration in university medical curricula and continued medical education of healthcare staff.36 Only then, a sufficient share of hospital stakeholders will have the ability to reflect on the responsibility of the health sector.
Reconciling healthcare and environmental values and attitudes
In line with the German population, participants saw mitigation as an important issue.37 However, as in studies with other hospital stakeholder groups, it appeared that beneficence through mitigating climate change was seen as subordinate priority compared with beneficence through immediate patient care.14–16 In the hospital context, as our study showed, there is often a significant concern about harming patients, while in the general context, mitigation measures predominantly raise concerns about limited personal freedom and imposed financial burdens.38 Results from a study comparing per capita GHG emissions from the health sector in different US states indicate that reduced GHG emissions do not compromise the quality of health systems.39 Various mitigation measures have already been shown not to jeopardise patients' health, including utilising reusable surgical gowns or laparoscopic instruments.40 41 Nonetheless, with regard to a variety of products and processes, hospital stakeholders currently lack sufficient data on GHG emissions42 and patient outcomes. Several mitigation measures, however, are known to even embody the principle of beneficence due to direct (individual climate-friendly behaviour leading to positive health effects) and indirect (collective action leading to positive health effects) health cobenefits; for example, eating plant-based food or using non-motorised transportation.43 Although health cobenefits are said to be the ‘greatest health opportunity of the 21st century’,44 they were rarely addressed by the participants. A strong focus on curative medicine may have contributed to this,45 as health cobenefits are often rather on the level of disease prevention. Direct and indirect health cobenefits of mitigation measures can increase the willingness to implement them. Therefore, they are a powerful, currently unexploited resource for climate change communication with hospital stakeholders.46 Moreover, non-evidence-based assumptions that certain climate-friendly alternatives harm patients should be corrected through education. This can reconcile healthcare and environmental values and attitudes, thereby strengthening the sense of responsibility for mitigation in hospitals. For interventions that currently lack data on GHG emissions and patient outcomes, both should be evaluated.
Increasing medical ethics considerations to guide climate change mitigation in hospitals
Among medical societies, there is an increasing discourse about the responsibility of the health sector, including hospitals, to mitigate climate change. Based on considerations consistent with medical ethics principles, medical societies conclude that hospitals must reduce their GHG emissions.7 47 This rationale was rarely taken up by participants and even at odds with their perceptions, as they partially saw medical ethics principles threatened by mitigation measures, as further discussed above. If evidence-based conflicts arise between mitigation and high-quality patient care, medical ethics can help evaluate and balance patients’ needs and mitigation considerations. Yet, drawing on the examples of overdiagnosis and overtreatment, it seems likely that there are more areas where reducing GHG emissions and promoting health could go hand in hand. For example, the widespread use of non-beneficial treatments at the end of life48 reflects the complexity and need for ethical considerations in this area.
Integrating medical stakeholders at all levels into mitigations strategies
As our research showed, motivated participants were partly discouraged from implementing mitigation measures because they felt unable to effect change due to lacking support from their superiors or colleagues. Thus, it is important that governing structures of hospitals commit to climate change mitigation and the sustainable use of resources as a guiding principle in their organisation.49 Environmental management systems and green teams should be established to integrate patients and staff on all levels into implementing changes.50 The resulting feeling of being able to effect change through own actions strengthens stakeholders’ internal locus of control and thus, the sense of responsibility for mitigation in hospitals.
Conclusion
The urgency of climate change and its health impacts require action by the health sector. To promote climate-friendly hospitals and to make mitigation effective, stakeholders at all levels should be made aware of hospitals’ contribution to climate change. The common (mis-)perception that mitigation measures jeopardise quality of care should be overcome by emphasising, that many mitigation measures have (in)direct health cobenefits or can be implemented while maintaining high quality of care. Finally, climate-friendly hospitals can strengthen fundamental medical ethics principles—beneficence, nonmaleficence and justice—by preserving health and preventing climate change-related harm to people worldwide.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by the ethical board of the medical faculty of Heidelberg University (sign S-497-2020). The staff council of Heidelberg University Hospital approved the study. All participants were informed about the study and gave written informed consent. Permission to audiorecord the interview was given voluntarily.
Acknowledgments
We thank all patients and employees of Heidelberg University Hospital, who have taken part in the interviews and made this research possible. We acknowledge financial support by the Else Kröner-Fresenius-Stiftung within the Heidelberg Graduate School of Global Health. Moreover, we would like to thank Dr. rer. medic. Saskia Wilhelmy of the "Institut für Geschichte, Theorie und Ethik der Medizin" (RWTH Aachen) for comments and help to refine the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY. 17th May 2023.
Contributors CQ, RS and AH were responsible for the study concept and design. CQ conducted the interviews and coded the data. AH had oversight of the coding of the data. The data were interpreted by all authors. CQ wrote the original draft while RS, ID and AH reviewed and edited the draft and the visualisations. All authors critically revised the manuscript for important intellectual content. RS and AH supervised the study. All authors gave final approval of the work to be published. CQ is the guarantor of this publication.
Funding This study was funded by Nationale Klimaschutz Initiative (03KF0150B); Else Kröner-Fresenius-Stiftung; Robert Bosch Stiftung (01000035-002). For the publication fee we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding programme „Open Access Publikationskosten“ as well as by Heidelberg University.
Disclaimer The Else-Kröner-Fresenius-Stiftung, Nationale Klimaschutz Initiative and Robert Bosch Stiftung had no role in the design, execution, interpretation or writing of this study.
Competing interests AH is member of the German Climate Change and Health Alliance (KLUG e.V.). The other authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Other content recommended for you
- Assessing the impact on chronic disease of incorporating the societal cost of greenhouse gases into the price of food: an econometric and comparative risk assessment modelling study
- Impact of a reduced red and processed meat dietary pattern on disease risks and greenhouse gas emissions in the UK: a modelling study
- Carbon footprint of hospital laundry: a life-cycle assessment
- Mortality, greenhouse gas emissions and consumer cost impacts of combined diet and physical activity scenarios: a health impact assessment study
- Reductions in inhaler greenhouse gas emissions by addressing care gaps in asthma and chronic obstructive pulmonary disease: an analysis
- How the low carbon economy can improve health
- Improving the environmental sustainability of paediatric care
- Health effects of adopting low greenhouse gas emission diets in the UK
- Tackling climate change: the pivotal role of clinicians
- Before/after intervention study to determine impact on life-cycle carbon footprint of converting from single-use to reusable sharps containers in 40 UK NHS trusts