Article Text

Abstract
Objectives Medical futility at the end of life is a growing challenge to medicine. The goals of the authors were to elucidate how clinicians define futility, when they perceive life-sustaining treatment (LST) to be futile, how they communicate this situation and why LST is sometimes continued despite being recognised as futile.
Methods The authors reviewed ethics case consultation protocols and conducted semi-structured interviews with 18 physicians and 11 nurses from adult intensive and palliative care units at a tertiary hospital in Germany. The transcripts were subjected to qualitative content analysis.
Results Futility was identified in the majority of case consultations. Interviewees associated futility with the failure to achieve goals of care that offer a benefit to the patient's quality of life and are proportionate to the risks, harms and costs. Prototypic examples mentioned are situations of irreversible dependence on LST, advanced metastatic malignancies and extensive brain injury. Participants agreed that futility should be assessed by physicians after consultation with the care team. Intensivists favoured an indirect and stepwise disclosure of the prognosis. Palliative care clinicians focused on a candid and empathetic information strategy. The reasons for continuing futile LST are primarily emotional, such as guilt, grief, fear of legal consequences and concerns about the family's reaction. Other obstacles are organisational routines, insufficient legal and palliative knowledge and treatment requests by patients or families.
Conclusion Managing futility could be improved by communication training, knowledge transfer, organisational improvements and emotional and ethical support systems. The authors propose an algorithm for end-of-life decision making focusing on goals of treatment.
- Medical futility
- withdrawing treatment
- end of life
- intensive care
- palliative care
- neuroethics
- clinical ethics
- care of the dying patient
- definition/determination of death
- anaesthetics/anaesthesiology
Statistics from Altmetric.com
- Medical futility
- withdrawing treatment
- end of life
- intensive care
- palliative care
- neuroethics
- clinical ethics
- care of the dying patient
- definition/determination of death
- anaesthetics/anaesthesiology
Introduction
If medical treatment is ineffective or unlikely to achieve an effect that the patient could appreciate as a benefit, it has been termed futile.1 ,2 The notion of medical futility has been heavily criticised on the grounds that it is ill-defined, blurs medical and ethical justifications of treatment and contains negative overtones.2
However, medical futility appears to be a relevant problem in clinical practice, and a cause of frequent concern for healthcare professionals, patients, relatives and the law, especially concerning life-sustaining treatment (LST) at the end of life.3–5 Many hospitals have developed futility policies, and states have drafted futility laws.6 A growing concern is how clinicians should react if patients or family members demand futile treatment, such as ineffective chemotherapy for end-stage cancer.7 Given the confusion and controversies of the discourse, it might be helpful to study what clinicians themselves think about futility.
Such a study is particularly feasible in a country like Germany where there is no equivalent term for medical futility and no associated polemical battlefield. Instead, German law and ethics focus on the positive opposite of futility, the so-called medical indication.8
Our aims were to explore how clinicians themselves define medical futility (in German ‘Fehlen einer medizinischen Indikation’), who they think should assess this, how they justify performing futile treatment and how they communicate futility situations to patients and caregivers.
Methods
Study design
Because of the explorative nature of our research aims, and in order to gather in-depth data on the experiences, attitudes and thoughts of clinicians, we used a predominantly qualitative mixed-methods approach, analysing protocols of ethics consultations and interviews with clinicians. The study was done in accordance with the requirements of the Ethics Committee at our university hospital.
Document analysis
We analysed 17 ethics consultations at a large tertiary referral centre in Germany over a 12-month period. These consultations were sought by clinicians who were uncertain whether to administer LST, offered by ethically trained palliative care specialists, and conducted in the setting of a team conference with or without the patient and his family. They were in accordance with the standards of clinical ethics consultation as formulated by the German Academy of Ethics in Medicine.9 For each consultation, a complete digital result protocol was accessed, anonymised and analysed using quantitative content analysis.10 The protocols have a length of 424–1408 words, were written by the consultants within 2 days after the consultation, and summarise the clinical situation, the participants and contents of the discussion, and the reasons and outcome of decision-making. They were sent to the care team, included in the patient's chart and sometimes given to the patient or family. Their intention is to document the decision-making process in order to guide carers, enhance consistent care across working shifts and provide legal evidence where needed.
Participant sampling and recruitment
For the interviews, we purposively sampled all physicians and nurses from intensive care medicine and palliative care medicine that were present at the ethics consultation meetings (combination of cluster and stratified sampling). They were considered to have, presumably, the longest experience with deciding about LST and futility at the end of life, yet from quite distinct perspectives. All clinicians could be identified in the consultation protocols and contacted by email or telephone. They were informed about the background, aims and procedure of our study, were introduced to the interviewer's professional background, and were guaranteed voluntary and pseudonymous data processing. All but one of the physicians we approached agreed to participate. We stopped sampling when the point of theoretical saturation was reached and additional interviews did not provide new insights.
Data collection
We conducted semi-structured interviews based on an interview guide that was developed after the document analysis, and with the help of pilot testing among experts. It consisted of four topics: (1) the definition of medical futility, along with typical examples of futile treatment at the end of life; (2) the persons who should assess futility; (3) the reasons for providing futile LST; and (4) the way futility is communicated to patients and their families. All interviews were conducted by AS, a male final year medical student pursuing his PhD, experienced in both intensive and palliative care and skilled in qualitative research methods. The interviewer was not known to the participants. The interviews took place in a quiet room in the hospital with no one else present except for the participant and the interviewer, and lasted 14–52 min. They were audio-recorded (Olympus WS-300M) and transcribed verbatim, using standard transcription rules. All transcripts received pseudonyms and identifiable information was eliminated.
Analysis
We conducted qualitative content analysis according to P Mayring.11 Transcripts were scrutinised with regard to the research questions; criteria for defining categories were established, and inductive coding was used to generate categories out of the material. The categories were continuously refined, ordered and reduced to a higher level of abstraction, using predefined rules. After 30% of the material had been worked through, the system of categories was reviewed, and reliability was tested by a second coder, a senior researcher and physician skilled in qualitative methods (RJJ). The whole material was analysed with the help of this category system, and the frequencies of categories in the material were counted. Finally, reliability was again tested and quotes were selected for publication, with the participants' profession and discipline in brackets. All interviews were conducted in German, but the quotes for publication were translated into English by an English native speaker. Text analysis was aided by the software MAXqda, V.2 (VERBI GmbH, Marburg, Germany).
Results
Document analysis
Table 1 summarises the information in the 17 consultation protocols with regard to the patients, the participants of the discussions, the treatment decisions made and how they relate to the ethical criteria of patient consent and futility.
Analysis of protocols on ethics case consultation (n=17)
Definition of medical futility
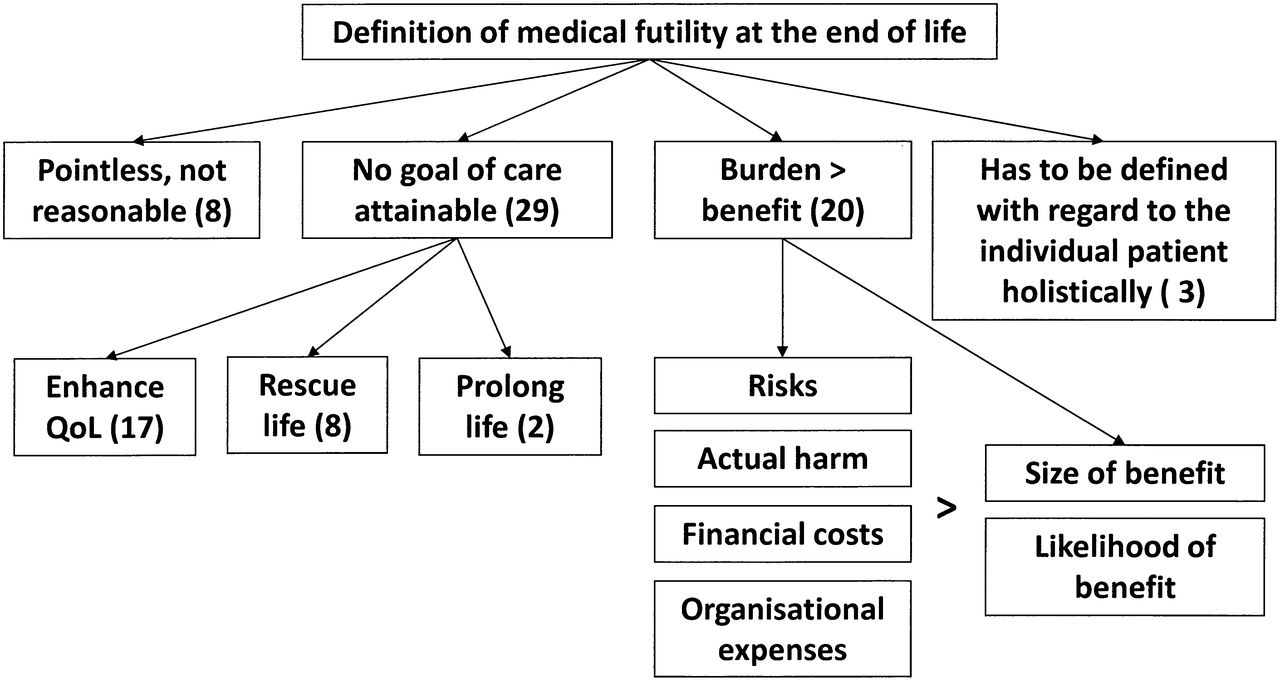
We interviewed 29 healthcare professionals, 17 from intensive care (12 physicians, five nurses) and 12 from palliative care (six physicians, six nurses). Asked whether they knew of situations when LST was medically futile, 18 participants (62%) responded affirmatively, 1 (3%) denied it and 10 (34%) were unsure. When asked to define medical futility at the end of life, interviewees displayed unease, demonstrated by a longer latency before the response and an increase of filler words by 17%. The categories they used for the definition are shown in figure 1.

Categories found in the interviews regarding the definition of medical futility at the end of life. Numbers in brackets show how often the categories were identified in the interview transcripts. (QoL, quality of life.)
Most frequently, participants associated futility with the lack of attainable goals of care:An intensive care unit is like a bridge which can be used to cross over a marsh. Having crossed the bridge the path must continue; if it does not, there is no reason to build the bridge in the first place or to force the patient onto the bridge (palliative care physician).
Many healthcare professionals also regarded a treatment as futile if the benefit conferred to the patient by the goal of care was surmounted by the burden with all associated risks, harms and expenses:If I have a patient who has a bronchial carcinoma, and it's compressing the large bronchial tubes and causing the patient to be short of breath, and by ventilation I can only temporise the decision for 1 or 2 weeks without ever being able to take the patient off the ventilator, then it's futile for me (…) Then I have to discuss with the patient whether the whole expenses and the burden is in relation to what comes out in the end (palliative care physician).
If the data show that a certain treatment measure will not, with a reasonable probability, and with reasonable side effects, lead to the desired goal, then it's futile (intensive care physician).
Some participants included financial aspects into their benefit-burden-assessment:I think it is not sufficient if the treatment doesn't do any harm. It also has to help the patient, I think, and, hm, it has to somehow be responsible within the financial system (palliative care nurse).
Prototypical situations where LST would be futile were reported to be: (1) an irreversible dependency on LST for the rest of life; (2) the terminal stage of malignancies; and (3) extreme injuries like a massive intracerebral haemorrhage.
Participants stated that it is the primary duty of the physician to assess whether the treatment is medically futile, yet only after consulting specialists of other medical disciplines (eg, neurologists) and the nursing team. Some also emphasised that the patient should be involved in this assessment:Well, the absolute indication, I think, is quality of life, and this can only be decided by the patient herself (intensive care nurse).
Reasons for providing futile treatment
Clinicians were asked about the reasons why LST is sometimes continued despite being considered futile. They came up with several reasons (figure 2), most notably personal reasons like concerns, fears and emotions:The reason is one thing: it's the fear of both physicians and patients to talk about death at all (palliative care physician).
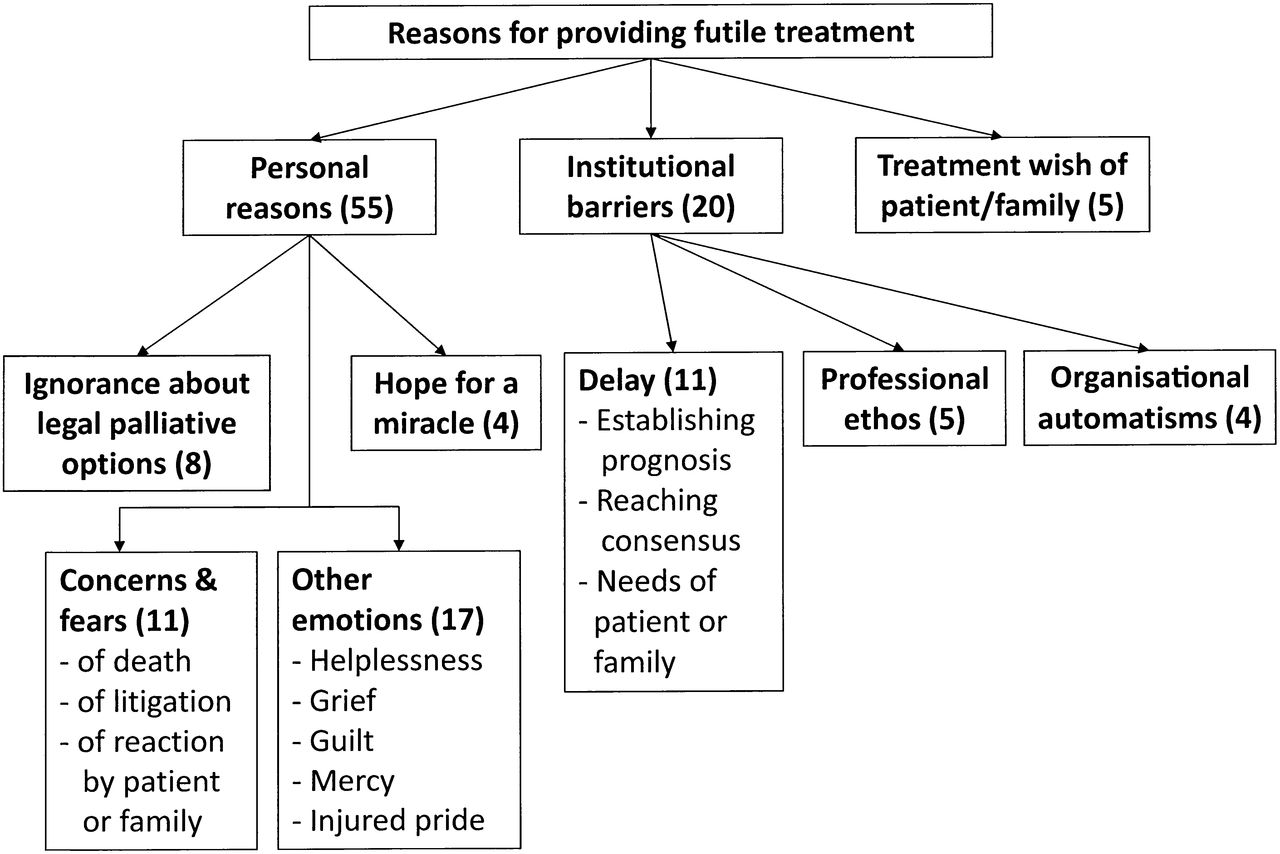
Categories found in the interviews concerning the reasons given for providing futile treatment at the end of life. Numbers in brackets show how often the categories were identified in the interview transcripts.
Somehow there is a blockade in your head. There is no other reason for it other than the fear that you could perhaps do something wrong (intensive care physician).
If, for example, patients come to us from the emergency unit with wide, fixed pupils and it is not quite clear whether treatment was really ceased, we still try doing everything. Then they receive everything, so that we can tell the relatives: ‘we did everything we could’ (intensive care physician).
Often times it is the doctors that are unable to say: ‘ok, let’s stop' (…). I don't know whether that has something to do with their ego that they think: ‘I do not want to lose him now’ (intensive care nurse).
Other reasons seem to be treatment wishes of patients or relatives, ignorance of law and of palliative treatment options, hope for a miracle, and institutional barriers:Often there is a surgeon involved who, of course, is still up to a cure, and for whom it is hard to accept that he cannot go any further at that point. He has to be heard, and this can take a while (intensive care physician).
If a patient is declared an emergency patient and comes to the ICU as such, in principle, he needs treatment, otherwise, there would be no reason for him to come to our unit (intensive care physician).
We have become so conditioned that we just have to do everything. And, and, withholding something, or not doing something, we learnt, means to not help the patient, and this simply contradicts our medical ethos (intensive care physician).
Communicating futility to families
While nurses and physicians did not differ in their statements, we found that participants from intensive care and those from palliative care focus on different aspects when they communicate futility to patients and their families (table 2). Regarding the setting and form of communication, these differences are exemplified by the following quotes:What is paramount is an empathetic conversation. What I always do at the beginning is to ask what the patient already knows. That is often different to what is found in the chart or what my opinion is (palliative care physician).
Reported practice of communicating futility to patients and their families
We usually try to explain to the relatives in several consecutive conversations, on different days, the difference between prolonging life and prolonging suffering, so to speak (intensive care physician).
The content of talks about futility also varies somewhat between the two disciplines. A palliative care physician and an intensive care nurse describe their approaches in the following way:It is very important to be honest with the patient right from the start. This means saying, for example, with regard to chemotherapy for a metastatic breast cancer, that it is only about containing and slowing the tumour growth, not curing it (…). And you have to tell the patient the alternatives, such as palliative care. I actually often heard doctors saying “either we do chemotherapy now or the pain will continue to increase”. I mean, what choice is then left for the patient? (palliative care physician).
Mostly, it is the case that we nurses and the relatives say “this does not make sense any more”, the physicians, however, say “yes, yes, we can manage this, he will go to rehab.” Then we just say to the relatives, rather secretly, “say that your husband would not want this” (intensive care nurse).
Discussion
Our data confirm the observation that medical futility is a relevant problem at the end of life.12 The majority of ethics case consultations that we retrospectively analysed (9 of 17) concerned cases on intensive care units in which the physicians considered LST to be futile. These situations were so controversial or difficult that they prompted large round-table discussions with the care team, family members and ethics consultants. Other reviews of ethics consultation confirm the high prevalence of futility disputes.4 The frequency and societal relevance of futile treatment at the end of life has just been underscored by a large retrospective cohort study demonstrating high rates of surgery in the last weeks and months of life.13 Considering the fact that a large part of lifetime healthcare costs are caused in the last year of life,14 ,15 and that reducing non-beneficial treatment on intensive care units may reduce the costs,16 this question bears considerable economic and ethical relevance to society.
Although 9 of the 17 case consultations clarified that LST was futile, this treatment had been provided up until the consultation meeting in all of these cases, and in four cases futile treatment was continued even after the consultation, mainly in order to give families more time to cope with the situation. From an ethical and legal perspective, futile treatment is not justified and should not be performed.17 However, if we want to improve the normative practice, we have to study the reasons why futile treatment is sometimes done, especially at the end of life. In the interviews with intensive and palliative care clinicians we identified several possible reasons. Interestingly, demands of family members was not the most frequently mentioned reason, in contrast to a survey among Canadian intensivists.3 A plethora of emotional difficulties surfaced in our interviews, in addition to well-known problems such as delay due to prognostication and consensus-seeking, communication problems and lack of legal or medical knowledge.18 ,19
Based on these results and the literature, it appears necessary to improve end-of-life decision making on intensive care units by various interventions: regular and proactive family meetings,20 effective ethics consultation,16 conducive organisational structures and applicable hospital policies,6 integration of palliative care expertise in intensive care,21 improved legal education, emotional support (eg, by supervision), and specific training of end-of-life communication skills.22
In our study, the fear of communicating futility to the patients and their families was mentioned as one of the reasons for providing futile care. It has been shown that German physicians tend not to disclose their unilateral decisions about the futility of treatment at the end of life, especially if they predict that the patient or family will not agree with this decision.23 On the other hand, German oncologists justify this practice by assuming ‘silent acquiescence’ by the patient or the family.24 It has also been documented that intensive care clinicians in Germany are dissatisfied with end-of-life communication, in particular nurses who run into moral distress when having to provide futile care despite their moral convictions.19 Of note, in our interviews, we heard that nurses sometimes team up with the patient's family and try to get the physicians to stop LST by supporting the futility judgement with the assertion of a presumed treatment-opposing will of the patient—be it true or not.
It is therefore relevant to know the communication styles that clinicians favour when disclosing the futility of further treatment. Our results justify the hypothesis that intensive and palliative care clinicians follow somewhat different communication strategies in this respect. While intensive care clinicians use a more cautious, indirect and matter-of-fact approach, palliative care clinicians favour a rather swift, direct and personal approach. Both may have their merits depending on the circumstances, and it may be necessary to combine elements of both.25 In order to develop and train the best communicative approaches, it is imperative to understand more about the needs of families.26
Last but not least, communication will only succeed if clinicians have a proper understanding of the meaning of futility and its place in decision making. Professional guidelines or hospital policies on medical futility have been advocated as a means to improve end-of-life decision making.6 ,27 In Germany, however, the few existing professional guidelines on end-of-life decision making only touch on the issue of futility, and are insufficiently known by healthcare professionals.28 Hospital policies are still in a pioneer stage, and the development of such a policy was one of the lessons our hospital drew from this interview study and a related survey.19 ,29
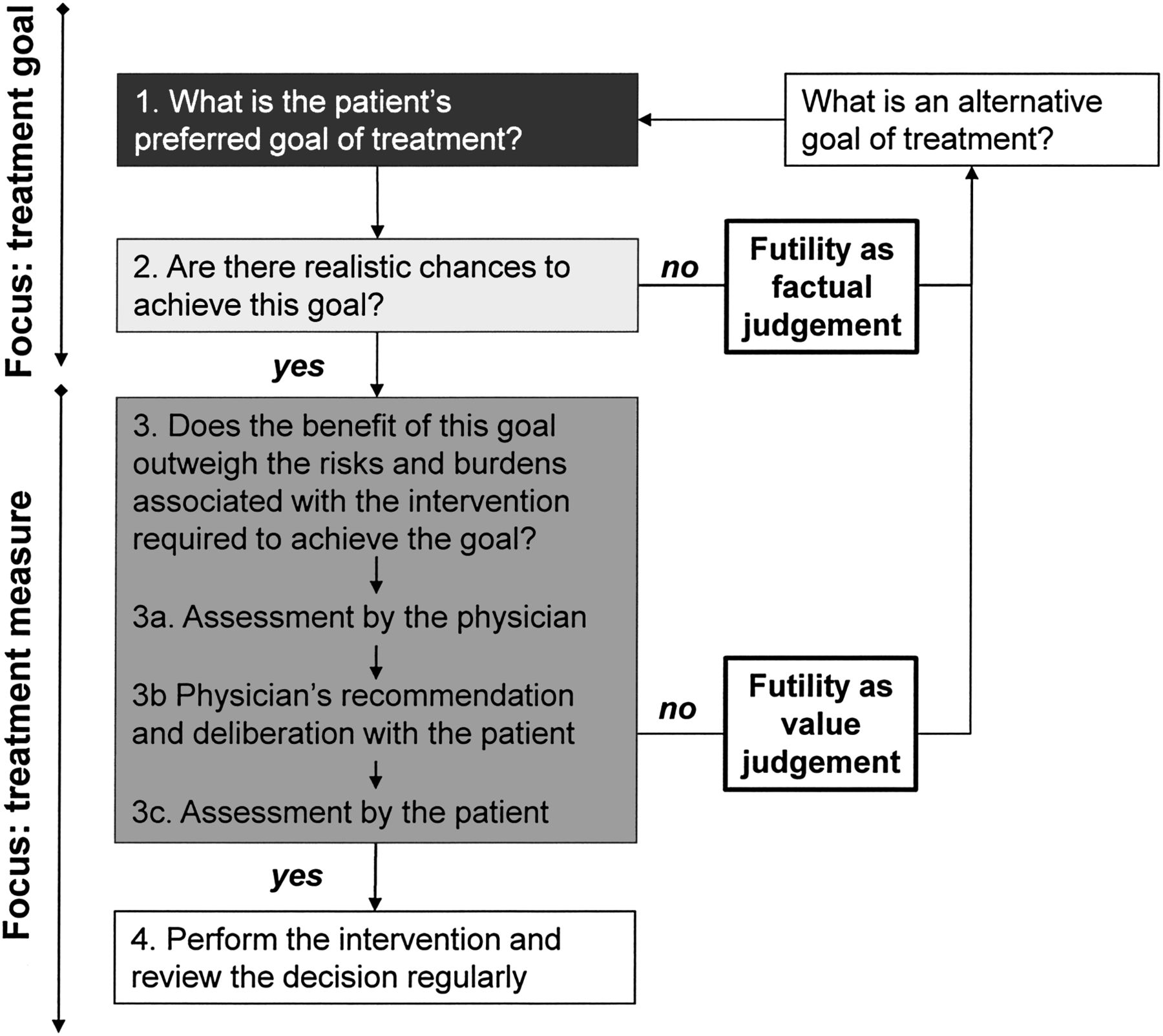
Our data show that clinicians do not share a widely accepted, readily accessible definition of medical futility. Yet, they identified key elements of futility that match with the predominant expert view1 and our own normative analysis. This analysis led us to a detailed algorithm for end-of-life decision making (see figure 3). It is not derived from the interview data, but intended to be a stimulus for normative discussion. The model focuses primarily on goals of treatment, and secondarily on treatment measures. It intertwines the two principal ethical grounds of treatment decisions: patient autonomy and patient wellbeing. The algorithm visualises that the patient's autonomous consent rests on two critical questions: (1) what is the patient's preferred goal of treatment; and (2) how does the patient evaluate the benefits versus risks and burdens of the intervention needed to achieve this goal? The responsibility of the clinicians is twofold: determining the chances to achieve the goal of treatment, and assessing the likely benefits, risks and burdens according to the standard of a reasonable person, as a basis for deliberating with the patient about the intervention. The model thus reflects a process of shared decision making between the patient, the family and the clinicians.

{kind=link}
{kind=link}
{kind=link}
Schematic algorithm of treatment decision making. The algorithm starts at the top left, focusing first on treatment goals and then moving on to specific treatment measures. Black box (1): questions to be answered by the patient or his surrogate; light grey box (2): question to be answered by the physician; dark grey box (3): question to be answered by the physician and the patient (or the patient's surrogate) together.
In contemplating the chances to reach the goal of treatment and performing a benefit-burden-analysis, this model covers both the quantitative and qualitative aspects of medical futility,2 ,17 sometimes also called the strict and loose definitions of futility.30 It clarifies that medical futility may be the result of a purely factual judgement of prognosis (futility as ineffectiveness). However, it may also be the result of a value judgement that the expected benefit for the patient is outweighed by the likely negative consequences for the wellbeing of that particular patient (futility as a negative benefit-burden-ratio). In the latter sense, it has to include the patient's view and, hence, reflects patient autonomy. It is therefore debatable whether ‘futility’ is a good name for this value judgement that expresses both the physician's obligations to beneficence and non-maleficence, and the obligation to respect patient autonomy.
The model deliberately excludes one further consideration that is sometimes relevant in treatment decision making, and has also been addressed by some of our interviewees: the interests of others, such as the patient's family or other patients. Some scholars have advocated that it may be ethically justified in extreme cases to perform futile treatment for the benefit of the relatives.31 Moreover, a treatment that is both indicated and supported by the patient's will may be legitimately withheld in a situation of scarce resources and the necessity to do a fair bedside rationing.7 However, both decisions are based on grounds of social justice and, hence, considerations of social ethics apply that may be quite different from that of individual ethics. Incorporating such considerations into the very concept of medical futility may obfuscate its meaning and jeopardise its applicability. Interestingly, neither treatment for the benefit of third parties, nor bedside rationing, was directly addressed by the clinicians in our study.
This study has several limitations. Due to the research questions and the methodology used, it does not purport to yield a representative picture of clinicians' perspectives on medical futility at the end of life, its aim being to generate hypotheses. The sample was confined to a German hospital and the setting of intensive care medicine. The descriptive results cannot be used to support certain normative ethical claims, but they may be of value for a critical review of the decision-making processes in clinical practice, and for the planning of future studies on this issue.
In conclusion, this mixed-methods study in the context of adult intensive and palliative care at a tertiary hospital in Germany confirms that medical futility is a practically relevant problem at the end of life, that clinicians have difficulties defining futility and communicating it to patients or relatives, and that the major reasons for them to provide futile treatment at the end of life are their own emotional problems and institutional barriers.
Acknowledgments
The authors thank all participating clinicians and all colleagues at the respective institutions for critically discussing the manuscript.
References
Footnotes
Competing interests None.
Ethics approval Ethics approval was granted by the Ethics Committee of the University of Munich.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- The concise argument
Read the full text or download the PDF:
Other content recommended for you
- Futile life-sustaining treatment in the intensive care unit – nurse and physician experiences: meta-synthesis
- Doctors’ perceptions of how resource limitations relate to futility in end-of-life decision making: a qualitative analysis
- The development of “medical futility”: towards a procedural approach based on the role of the medical profession
- Perceptions of patients on the utility or futility of end-of-life treatment
- Highlights from this issue
- Withdrawing life support and resolution of conflict with families
- Identifying futility in a paediatric critical care setting: a prospective observational study
- Reasons doctors provide futile treatment at the end of life: a qualitative study
- Palliative care integration in the intensive care unit: healthcare professionals’ perspectives – a qualitative study
- Association of medical futility with do-not-resuscitate (DNR) code status in hospitalised patients