Article Text

Abstract
Background: We were finding volunteers for functional magnetic resonance imaging studies with abnormalities requiring referral surprisingly frequently. The bioethics surrounding the incidental findings are not straightforward and every imaging institution will encounter this situation in their normal volunteers. Yet the implications for the individuals involved may be profound. Should all participants have review of their imaging by an expert and who should be informed?
Methods: The normal volunteers that were imaged with magnetic resonance (MR) which were reviewed by a consultant neuroradiologist. All participants completed a volunteer consent form in addition to a standard departmental MR safety screening form. The volunteer screening form requires the general practitioner details to be completed and asks the participant to consider closely the possibility and implications of finding an unexpected but potentially serious abnormality before signing.
Results: 525 different individuals were scanned as normal volunteers, the mean age was 35-years and 330 were males. Of these 525, 46 had definite significant abnormalities (8.8%), mean age 50-years.
Conclusion: We have found a high rate of incidental abnormalities amongst individuals participating in imaging studies at our institution. It is our current practice to inform the research study participant of the findings, counsel them and inform their primary care physician. We think that it is advisable for researchers utilising MR imaging of the brain to have access to trained neuroradiologists, a protocol in place to deal with this problem and take consent in a way that allows the participant to realise the possibility of an abnormal finding.
Statistics from Altmetric.com
Over the past decade there has been a huge expansion of interest in functional magnetic resonance imaging (fMRI) of the brain for neuroscience research and it is capturing the interest of the general public. Illes has estimated that between 1991 and 2000 using fMRI as the keyword search that there may have been at least 30 000 research participants in fMRI studies in the published literature.1 Magnetic resonance imaging (MRI) is an extremely powerful diagnostic tool for the central nervous system. Pathology may be detected in asymptomatic individuals as the sensitivity of MRI has been shown to be equal to or better than competing technologies.2 The bioethics surrounding the incidental findings are not straightforward and every imaging institution will encounter this situation in their normal volunteers. Yet the implications for the individuals involved may be profound not only for the health of the individual but also financially, with implications for driving licenses, insurance eligibility and borrowing. Should all participants have review of their imaging by an expert? If abnormalities are found, who should be informed?
We decided to review the incidental findings from volunteers in our institution as it was felt that abnormalities were being found in an unexpectedly high number. We reviewed the findings from the volunteers who underwent intracranial magnetic resonance (MR) scanning on a new 3T installation (2003) and from when an existing 1.5T was previously installed (1998) in the same university research MRI Unit.
MATERIALS AND METHODS
The normal volunteers that were imaged on a 3T Intera MR system (Philips Medical Systems, Best, Holland) and on a 1.5T Edge Eclipse (Philips Medical Systems, as before) were reviewed by a consultant neuroradiologist. All participants completed a volunteer consent form in addition to a standard departmental MR safety screening form. The volunteer screening form requires the general practitioner details to be completed and the participant information sheet asks the participant to consider closely the possibility and implications of finding an unexpected but potentially serious abnormality before signing to give their consent to participate in the research. The participant information sheet also states that the participant’s general practitioner and/or consultant of the appropriate specialty will be contacted.
All volunteers were then re-screened verbally before entering the magnet room in compliance with departmental protocol.
A range of MR sequences were performed depending on the research study imaging protocol. No formal clinical protocols were used, however, each examination contained at least axial T2 weighted imaging of the whole brain except 69 participants all in a single study that had volume T1 weighted imaging only.
The participant’s primary care physician was informed in all cases as per our institutional protocol.
RESULTS
No volunteer was asked to remain in the MR scanner for longer than one hour. General compliancy was good and no examination was terminated due to claustrophobia. In total there were 525 different individuals scanned as normal volunteers, of whom 46 (8.8%) had definite significant abnormalities (see table 1). A further four individuals had scans suggestive of significant pathology. Significant pathology we have defined in terms of diagnoses requiring referral (see the Discussion section), these have been classified by Illes et al in 2004 as categories 2 to 4.3

{kind=link}
The mean age amongst the volunteers with abnormalities was 50-years and there were 17 males and 29 females. The mean age amongst the volunteers as a whole was 35 years and 330 were males out of the 525. The mean age of the 151 participants imaged at 3T was 36 years (range 20–67 years; median 34 years) and 35-years (range 20–81 years; median 30 years) at 1.5T. On both systems, unexpected pathology had not changed between the first installation (a 1.5T scanner) in 1998 and the second (a 3T scanner) in 2003. No difference in the incidence of pathology was demonstrated between the different field strength scanners (31/374 at 1.5T, 15/151 at 3.0T; p = 0.6). It was noteworthy that our incidental pathology did not include any cerebral aneurysms as might have been expected in a sample of this size, although the average age of these participants was relatively low.
Among the “others” category there were cases of cerebellar atrophy, one pituitary microadenoma, one large temporal arachnoid cyst, one of a perinatal infarct and one volunteer had bilateral frontal parafalcine encephalomalacia consistent with previous head injury.
DISCUSSION
Incidental findings are topic of current debate and importance to the ethical undertaking of research with human participants. Most studies appear to be quite consistent in reporting a 1 to 2% rate for the most serious pathology such as tumours and cerebral aneurysms on MR brain imaging.3–8 In our study we have detected four cerebral tumours and one pituitary tumour (out of 525 volunteers) but we have also seen six cases felt on imaging criteria to be suggestive of inflammatory/demyelinating disease which we consider to also be serious and potentially treatable conditions. This manuscript and an increasing number of others demonstrate the inevitability of such serious findings and they expose the nature of the relationship between researcher and participant. Ultimately they lead us to scrutinise the duties of care that lie between researcher and participant, and raise several important practical issues. These include whether researchers have a duty to look for incidental findings and how hard should they look? Do the same principles apply to all researchers, including non medical ones? How large a problem are incidental findings on brain imaging? How much should the participants be told and who else if anyone should also be told? What mechanisms are required to deal with the incidental findings research throws up?
In our institution all of the neuroscience research groups have members who are also practising doctors. It is our opinion that as stated in the introduction to the Declaration of Helsinki that “It is the duty of the physician to promote and safeguard the health of the people” (author’s italics).9 This is further reinforced by the Declaration “Physicians should abstain from engaging in research projects involving human subjects unless they are confident that the risks involved have been adequately assessed and can be satisfactorily managed.” Incidental findings appear to be inevitable in research volunteers and, in our view, the systems for dealing with them must be in place. Belsky and Richardson have put forward the concept of entrustment between researcher and participant giving rise to a duty to provide ancillary care.10 They suggest that since a participant’s permission is required to do a test or collection of confidential information, the scope of the entrustment typically includes following up on any clinically relevant information or diagnoses generated. The scale of the resulting responsibility to provide ancillary care is then related to the vulnerability of the participants, their uncompensated risks or burdens, the depth (length and intensity of relationship) and participants’ dependence on the researchers.
Though experienced neuroscientists may be good at spotting scans that deviate from normality, they are not trained neuroradiologists with the necessary background and training to interpret the images clinically. Indeed there may not be any standard clinical sequences available for review, but if we accept the argument of Belsky and Richardson a duty of care still exists. If there is no responsibility to act on information generated by tests performed in the course of research then it implies participants are a means to a research end.10 Just because the researchers are not trained to evaluate images clinically it does not preclude the engagement with those that are. Our current practice has been agreed and developed with our local medical ethics committee and is to include whole brain T2 weighted or fluid attenuated inversion recovery (FLAIR) weighted imaging for research participants. It is our current policy that we do have review of imaging by a practising specialist neuroradiologist. This service is, and has been provided, free of charge, nor are the clinical reviewers included amongst the authors of the publications relating to the research (as payment “in kind”). However, it has been seen as an important part of research governance within the academic radiology department. We believe the cost should be included in the full economic costing of research studies. Given the reduction in reporting costs occurring, certainly in the UK, where a single body area MR scan can be commercially reported for less than £30 ($54, €37), this represents less than 10% of the full economically costed price of MR scans funded by UK government agencies. Our views are echoed by others such Charles Nelson, who has advocated the inclusion of the costs into research grants in the US.11
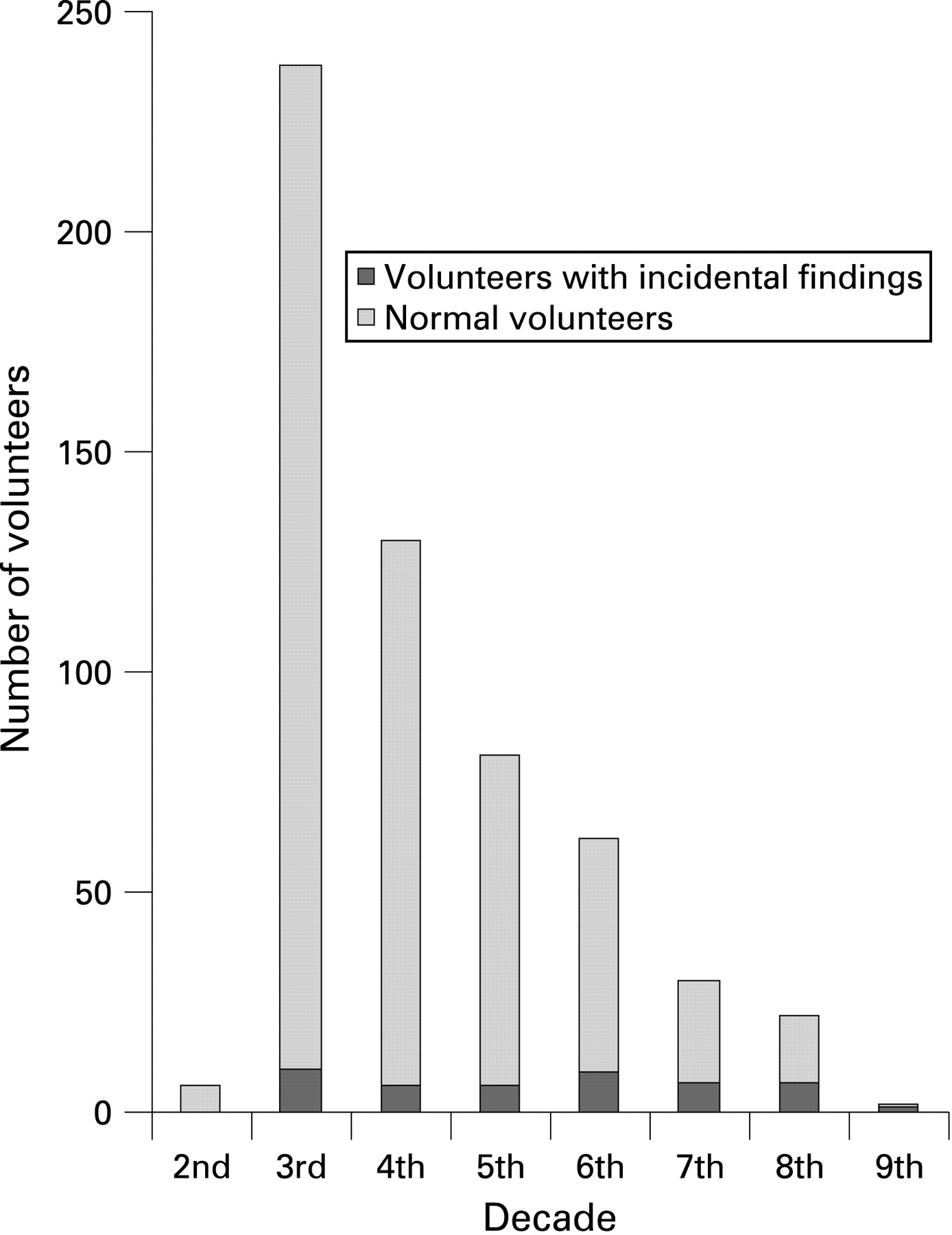
Central to the interpretation of this and other studies that have found surprisingly high rates of abnormality in “normal” volunteers is the definition of abnormality and how its importance is categorised. The assumption made in the previous sentence is that what is “normal” is clearly known. However, what constitutes normality, particularly in the population of older people, is not clear. In addition the amount of gathered information may be insufficient to determine normality. We ask volunteers about their past medical history and medication but do not, for example, measure blood pressure at time of attendance for imaging. As discussed by Farrel et al in a commendably thorough study, there may be considerable variation in cerebral volume amongst normal older people.12 They obtained detailed neurocognitive testing and blood pressure measurement, added to routine questioning about past medical history and medication, yet still found marked variation in brain volume. This is in keeping with our very conservative approach to including atrophy amongst our abnormal scans. However, the same limitations of knowledge about the truly healthy older population in the context of cerebral atrophy by Farrell et al may also apply to white matter disease. How far away from the truth is the generally accepted definition of white matter normality one unidentified bright object per decade? Certainly the proportion of normal volunteers with white matter disease deemed “vascular” in nature (as apposed to inflammatory/demyelinating white matter disease) rises sharply from one person in their third decade out of 228 to six out of 15 in their eighth decade in our study (p = 0.001). With two people with white matter disease out of 75 in their fifth decade and five out of 53 in their sixth decade it suggests there may be an acceleration in frequency after the age of 50, though this is not a statistically significant result, p = 0.1).
Katzman et al utilised the classification used in the cardiovascular health study.8 13 This simplifies and categorises the incidental findings as those that do not require referral as they are normal variants or common asymptomatic findings; routine referral required with old infarction given as an exemplar; urgent referral required that needs urgent invention but not as an emergency, such as a low grade brain tumour and immediate referral required such an acute intracranial haemorrhage. Thus, of the 18% abnormal scans seen in the Katzman study, abnormalities that were classified as needing no referral were sinus disease, age related changes and solitary non specific T2 hyperintensities. Routine referral included pathologies such as old lacunar infarcts, possible demyelinating disease, choroid and pineal cysts, hypothalamic lipoma and old traumatic damage. The other groups were for urgent referral in which they included arachnoid cysts, cavernous angiomas, low grade tumours and aneurysms. No immediate referrals for emergency treatment were made in the group studies by Katzman.
Although we concur with the approach of the Bryan-Katzman categorisation, in practice there are a number of problems with this approach.8 13 Firstly, it is unlikely that there will be any individuals requiring immediate referral in “normal” volunteers. Secondly, the categorisation reflects its time. We would argue that possible demyelinating disease is more urgent than say a small incidental arachnoid cyst, as the risk from the latter is extremely small and rarely acted upon, whereas demyelinating disease may be amendable to treatment now. Similarly, given the importance of blood pressure control in older people, detecting features such as small vessel disease that may reflect its presence is of importance whether the person is 80 years or not, though we accept that the finding in a 30-year-old person may represent more severe disease with greater life time risk.
In our assessment of incidental pathology in research volunteers we have tried to be pragmatic and have simplified the classification still further to “would you put this finding into a clinical report and would you intend the physician to act upon it”, whether this meant review of either hypertension or medication, for example, or more urgent neurosurgical opinion for a tumour. We have not included at all any findings that we consider of no clinical consequence in routine clinical practice such as unidentified bright objects consistent with age, so called age related changes, small arachnoid cysts and inflammatory mucosal disease, for example. This is similar to the categorisation used by Illes et al,3 but we have been more stringent since we have excluded inflammatory mucosal disease of the sinuses and mastoid fluid. Paranasal mucosal inflammatory change is frequently found as an incidental finding in our routine clinical practice, which reflects that of Patel et al14 who found incidental inflammatory mucosal changes in 49.2% of patients studied in their series from the UK. Atrophy has only been included as a significant finding when in the context of definite atrophy in the opinion of the neuroradiologist reviewing the imaging in an unexpectedly young individual, which would have necessitated further investigation in routine clinical practice. White matter disease consistent with small vessel cerebrovascular disease has been included amongst the significant results as this would be included in any routine clinical report of an MR brain scan and may necessitate review for hypertension, other cardiovascular risk factors or medication in clinical practice.
Katzman et al8 found a rate of 4.1% for the type of pathology we describe in 8.8% of volunteers in our study, and Illes et al3 had a rate of 6.6% including cases of “acute sinusitis” as judged from the imaging performed which included both T1 and T2 or dual echo T2 weighted scans. Why should this be? There will have been differences in patient mix, but Katzman et al do not include full demographic details to make a comparison with. It is clearly not safe to assume that all volunteers are normal controls as volunteers can “self refer”, with existing symptoms. Following discussion with the volunteers after the scan in this study, one was aware of the diagnosis of multiple sclerosis but had omitted to inform the MR Unit staff, one was aware that there had been a problem in the past but had undergone no prior investigations. No other volunteers were symptomatic. This is the first series of this type reported from the UK, it is possible that there are either cultural differences between the previous series, from North America and Scandinavia, and our own.3–8 Alternatively, it could perhaps reflect the local perceived ease of access to MR scanning, in our institution—as throughout much of the UK—there is no primary care access to MR imaging of the brain.
Perhaps the best study of young people who can be expected to be entirely fit and well has been performed by Weber and Knopf.15 They found abnormal findings in 6.55% of 2536 males, mean age 20.5 years, who were applicants for military flying duties in the German Air Force. This included arachnoid cysts (1.7% of the 2536) and Chiari deformities (also diagnosed in 1.7% of the 2536). All of the arachnoid cysts, except one particularly large cyst, were excluded from our positive findings as these are not acted upon by our neurosurgeons and Chiari deformities cannot be reliably detected on axial brain imaging available for review unless quite marked, thus we may have missed these cases. This rate of 6.55% of scans showing abnormalities in the German study seems very similar to our finding of 4.4% incidence of abnormalities in those volunteers in their 3rd decade after these two main differences are considered.
Paternalism has receded greatly in medicine, with a presumption that patients should be given the available information in an understandable form to allow them to fully participate in their own care and its associated management decisions. Shalowitz and Miller have echoed this, stating that research participants have a “presumptive entitlement to information about themselves”.16 Indeed Illes et al also suggest that as a principle there is an obligation to disclose incidental findings of potential health importance to research participants.17 18 Interestingly, in a survey of research subjects, a majority expected a research scan to detect abnormalities if they existed and the overwhelming majority (>90%) expressed the wish to be told of such findings with a most wanting this done by a physician attached to the research team.19 Currently, we adopt a similar position to that of Illes and others and only inform participants of incidental findings that we believe may have significant clinical importance, which they may derive net benefit from knowing. However, we have some concern as this is surely paternalism; in truth we may not know the risk of certain findings for an individual, which at best can only be based on current knowledge. What was once thought to be insignificant may in the future, with greater knowledge, not be so, or indeed vice versa. At present it is being generally advocated that the balance of psychological harm that the burden of knowledge brings means that minimal risk findings should not be passed onto the research participant. We agree with this as it seems humane but we are also aware that this is not how clinical medicine increasingly works.
One of the problems with incidental findings is that their significance may be unknown or controversial, as suggested above. There will also be some false positives, though temporarily worrying; at least these see some closure when they are proven to be artefacts, for example. However, the natural history of some of these incidental pathologies is not clear even when the diagnosis is certain, what is the lifetime risk of a small incidental convexity meningioma or even a solitary small 3 mm cerebral aneurysm in a subject without previous subarachnoid haemorrhage? As far as we know from the International Study of Unruptured Intercranial Aneurysm II trial, anterior circulation aneurysms less than 7 mm have lower risk of haemorrhage than the risk of serious complications from treatment.20 But how many of us would still opt for treatment because we could not cope with idea of a “ticking time bomb which could go off at any time throughout one’s life”? Other findings are a matter of debate, for example, cerebellar ectopia is decent of the cerebellar tonsils through the foramen magnum with in the past up to 5 mm seen as normal, yet it has been found that considerably less than 5 mm of decent may be associated with neurological problems.21 It is these kinds of controversies that make us aware of the paternalistic approach we have adopted and others also appear to be advocating.
The Cambridge Wolfson Brain Imaging Centre has a policy of only informing the participants’ primary care physician with the express permission of the participant.22 This seems from the participants’ perspective entirely reasonable. However, if the person involved, for example, was at risk of epilepsy and a driver who continued to drive, the potential consequences for the individual lead us to ask if we have done the participant a disservice. We would also have a competing duty to society that potentially perhaps outweighs our duty to the individual, irrespective of the Declaration of Helsinki. Indeed, what is the response of this approach that doesn’t automatically trigger primary care referral if it emerges that the participant may not be capable of making a rational decision on their illness and its treatment? For example, what if the participant has a frontal lobe tumour and their judgement is impaired? Although we counsel our participants with the help of our neurosurgical and neurology colleagues, people sometimes change their minds or need time to decide what course of action to take. We believe this process is more robust with the involvement of the participant’s primary care physician who may know a great deal more about a person and their circumstances than is known from the research and subsequent counselling interaction. Even if there is no existing relationship between research participant and their primary care physician, participants could benefit from another informed and independent opinion whose primary concern is the health and wellbeing of the participant. The continuity that a primary care physician provides must not be overlooked and their involvement at the start of any ongoing treatment is clearly valuable. It is likely that a rapport and relation will emerge which will be valuable to the participants’ future care. This is why, at the time consent is being sought, we make clear that we will inform the primary care physician of any clinically significant incidental findings.
The effect on the quality of life of “normal” volunteers having been found to have unexpected pathology may be profound, for example, in the case of the diagnosis of multiple sclerosis there may be a detrimental effect upon the individual’s ability to legally drive a motor vehicle, obtain health insurance or mortgages etc.23 Findings that turn out to be medically insignificant can still cause tremendous stress for volunteer subjects and their families.24 We consider it is our duty to point out potential hazards during consent and have to accept it will deter some volunteers; joining a research study even as a normal volunteer is not a trivial thing.
We believe structures need to be in place for incidental findings starting with the consent process. Participants need to be made aware of the possibility, given some guide to the actions the researchers will then take as part of their protocol for significant incidental findings (see box 1). We also later re-emphasise that if volunteers do not wish to know about any potential problems that they do not volunteer for the study.
Box 1 Information for participants: protocol for significant incidental findings
What if you find an unexpected but potentially serious abnormality?
This is a matter that you should consider closely before agreeing to become a volunteer.
The scan being done is designed to answer our research questions, not examine your brain medically. This MRI scan is not a substitute for one a doctor would order. It may not show problems that would be picked up by a medical MRI scan. However, if a significant important abnormality is detected then your GP will be informed. We will also recommend referral to a hospital doctor of the appropriate specialty.
If you are unhappy to be asked about your medical history then you should not take part. If you do not agree with this course of action then it is important that you do not participate in this study.
In our opinion, ethics committees and review boards need to insist that a protocol is in place for dealing with the review of the imaging, communicating with the participant and then the onward referral in to the clinical environment. In the UK the NHS means that concerns over the cost of medical care arising from these incidental findings is not an issue for us. But it would seem disproportionate to us that the researchers should bear the costs of the medical care if the depth of their relationship with the participant is that the participant has simply volunteered for an fMRI study with no other interventions.
In our institutional protocol, as indicated above, when an abnormality is discovered we first contact the principal investigator as the owner of the study with access to contact details for the normal volunteers in their study. If the findings invalidate the participant as a control subject the primary investigator is informed of this but full clinical details are not given. Then we counsel the participant and inform their primary care physician. We appreciate, however, that this easy access to clinical neuroradiology support is not the case in many research facilities.
If clinical evaluation of the participant’s imaging is to take place, fMRI images alone are not suitable for this purpose but at the other extreme should a formal clinical MR scan should be performed routinely on all volunteers? The most commonly used research sequence is T1 imaging but though an abnormality may be seen on it, pathology is generally better characterised by T2 weighted imaging (or FLAIR sequences). Our practice has evolved over the last few years; initially we did not insist on T2 weighted imaging in all volunteers but as we became more aware of the apparently high frequency of incidental pathology we changed to always include either axial T2 or FLAIR weighted imaging. Having now completed this study we believe we should offer a minimum level of diagnostic imaging to include the axial T2 or FLAIR sequence and a T1 weighted sequence in another plane. Certainly in the UK we still use CT as a diagnostic brain imaging tool but we would suggest that even a single T2 weighted sequence offers overall more sensitivity than a CT head scan without intravenous contrast. On the other hand, this is clearly less than has been adopted by some National Institutes of Health centres who have introduced a full diagnostic MR brain scan, but in our consent process we do make clear that we are not undertaking a clinical quality scan and that the primary purpose of the scan is research (see above). We simply want to use the least imaging that can minimise the number of equivocal findings that could lead to unnecessary investigation and the anxiety that goes with that investigation to the individuals involved. However, as noted above we did not find any unequivocal cerebral aneurysms in our volunteer group, which is somewhat surprising given a sample size of 525, but we do not advocate “chasing” pathology, as for example, by including an angiographic sequence of the circle of Willis to exclude aneurysms. Though it should be noted we would expect to find those anterior circulation aneurysms most likely to be beneficial to treat with a diameter of 7 mm or more with axial T2 weighted imaging with a slice thickness of 4 mm, no gap between slices and an “in-plane” pixel size of 0.45 mm2.20
In summary, we have found a significant rate of incidental abnormalities amongst individuals participating in imaging studies at our institution. It is our current practice to inform the research study participant of the findings, counsel them and inform their primary care physician. We think that it is advisable for researchers utilising MR imaging of the brain to have access to trained neuroradiologists, a protocol in place to deal with the incidental abnormalities that will be found amongst their volunteer normal control participants and take consent in a way that allows the participant to realise the possibility of an incidental finding.
REFERENCES
Footnotes
Competing interests: None.
Read the full text or download the PDF:
Other content recommended for you
- Incidental findings on brain magnetic resonance imaging: systematic review and meta-analysis
- Incidental findings on brain imaging and blood tests: results from the first phase of Insight 46, a prospective observational substudy of the 1946 British birth cohort
- Management of pineal and colloid cysts
- Fifteen-minute consultation: incidental findings on brain and spine imaging
- Detection of aneurysmal subarachnoid hemorrhage 3 months after initial bleeding: evaluation of T2* and FLAIR MR sequences at 3 T in comparison with initial non-enhanced CT as a gold standard
- Potentially serious incidental findings on brain and body magnetic resonance imaging of apparently asymptomatic adults: systematic review and meta-analysis
- Novel asymptomatic CNS findings in patients with ACVR1/ALK2 mutations causing fibrodysplasia ossificans progressiva
- Incidental findings on brain MRI of cognitively normal first-degree descendants of patients with Alzheimer's disease: a cross-sectional analysis from the ALFA (Alzheimer and Families) project
- A guide to imaging for common neurological problems
- Brain MRI roulette