Article Text

Abstract
The imbalance between supply of organs for transplantation and demand for them is widening. Although the current international drive to re-establish procurement via non-heart beating organ donation/donor (NHBOD) is founded therefore on necessity, the process may constitute a desirable outcome for patient and family when progression to brain stem death (BSD) does not occur and conventional organ retrieval from the beating heart donor is thereby prevented. The literature accounts of this practice, however, raise concerns that risk jeopardising professional and public confidence in the broader transplant programme. This article focuses on these clinical, ethical, and legal issues in the context of other approaches aimed at increasing donor numbers. The feasibility of introducing such an initiative will hinge on the ability to reassure patients, families, attendant staff, professional bodies, the wider public, law enforcement agencies, and the media that practitioners are working within explicit guidelines which are both ethically and legally defensible.
- non-heart beating organ donation
- end of life decisions
- definition of death
- conflict of interest
- double effect
- informed consent
Statistics from Altmetric.com
- non-heart beating organ donation
- end of life decisions
- definition of death
- conflict of interest
- double effect
- informed consent
Transplantation, in association with other medical advances that maintain life in the presence of organ failure, has, with each success, created more demand. Expansion of specific organs now deemed transplantable, such as bowel or limb, is less problematic in this regard than expansion of the potential recipient base for the more commonly used organs. Thus, the elderly patient, those with associated comorbidity, or those with disease such as hepatitis are not now viewed as beyond consideration. With a seemingly static or falling donor base, this generates a growing national1,2 and worldwide3 imbalance between organ supply and demand, with the inevitability of patients dying whilst on a waiting list.4
Certain professional groups consider it appropriate on the basis of this imbalance to explicitly restrict access to a waiting list, thereby avoiding the dishonesty of false hope and promoting furthermore one interpretation of fairness by ensuring a uniform policy nationwide.5 The fundamental principle is utilitarian, whereby listing is based on probability of longer term survival, rather than equitable, purely on the basis of need. Despite acceptance that the survival rate after transplantation of the sickest category of patient is reduced, the exclusion of those in whom death is imminent and inevitable without transplantation can, however, be considered contrary to justice.6,7 It remains unknown whether organ donation is influenced in either direction by this “efficiency” of organ allocation, but there is a certain irony if measures taken to restrict demand in the face of shortage of supply compound the problem. In the light of evidence that refusal of relatives is the commonest cause of lost potential donation,8,9 and can be in excess of 70% in some countries,10 it is timely to consider therefore whether strategies to improve supply may ultimately compromise societal commitment and increase the imbalance. There appears no alternative to this exercise since replacement autologous organs from human stem cells are clearly some way off and although breakthroughs have been made in reducing the immunogenicity of cloned animals,11 many hurdles still remain to xenotransplantation,12 not least an embargo by the Council of Europe on the basis of the inherent “considerable scientific, medical, ethical, social, and legal problems”.13
APPRAISAL OF THE POTENTIAL ORGAN DONOR POOL AND THE INHERENT ETHICAL ISSUES
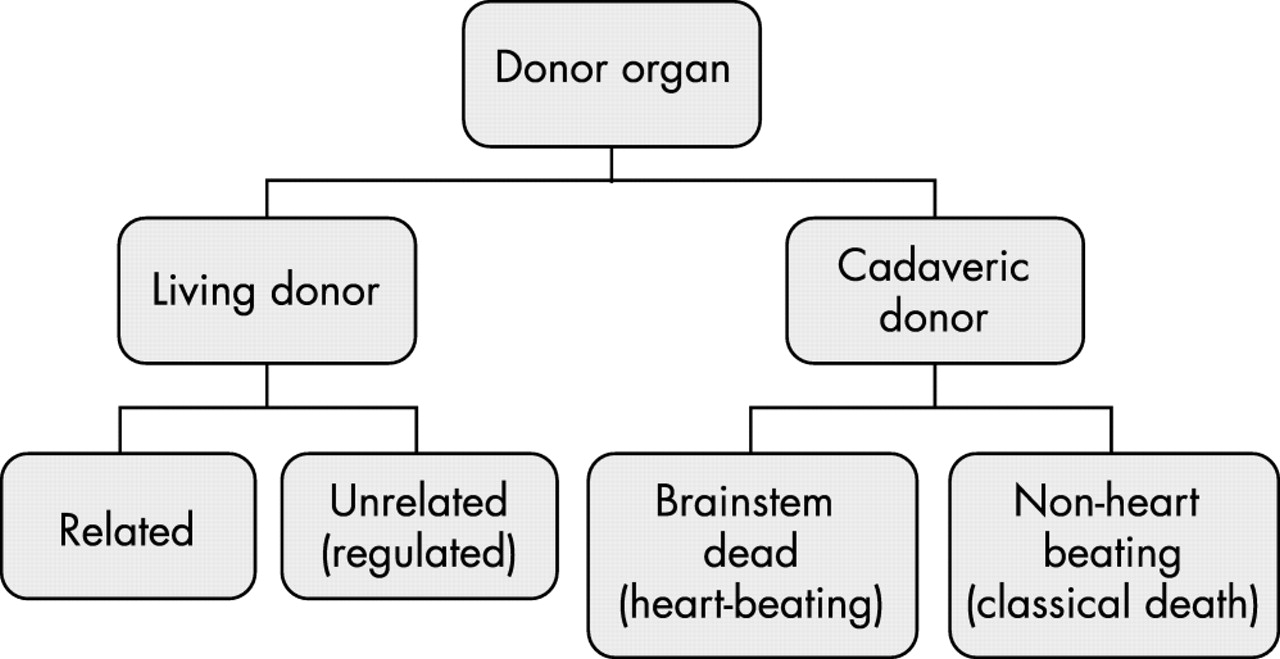
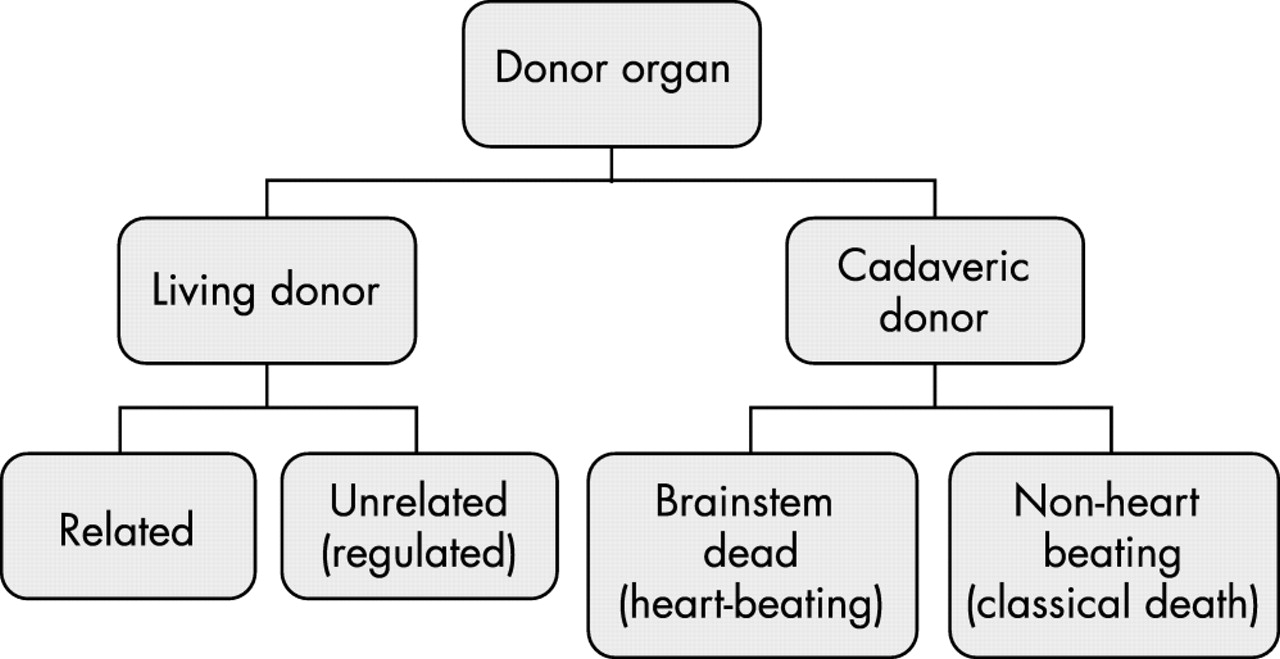
The greatest current source of transplantable organs in the Western world is the hospital based cadaveric donor (see figure 1). Other countries have alternative organ sources14 or in the face of non-acceptance of the concept of brain stem death,15 rely on the living to donate. Living related donation, given the shortage of cadaveric organs, is a significant aspect of practice worldwide, and although traditionally limited to a solitary kidney, has now extended to removal of liver or lung lobes, procedures not without hazard.16 This raises concerns as to validity of consent, in turn based on accurate information not only on immediate and longer term donor mortality and morbidity, but on graft function within the recipient,17 certainly an issue with the older donor.18 The other ethical issues regarding the inevitable explicit or implicit coercion inherent in living donation have been debated.19 The altruistic act of anonymous living donation has also been described,20 but although there is evidence that up to 32% of the population in British Columbia would be prepared to donate a kidney whilst alive to a stranger,21 it is difficult to expect that this will make major inroads into the deficit, and the process inevitably comes with an ethical dimension.22 Commercial traffic in organs is illegal and to this end any unrelated living donation in the UK requires the prior approval of the Unrelated Live Transplant Regulatory Authority (ULTRA).
{kind=link}
Current donor organ sources.
OPTIONS FOR INCREASING THE CADAVERIC DONOR POOL
The above problems associated with living donation lead to scrutiny of either the process of dying, or of recruitment of the brain dead population, to increase the donor pool (see table 1). Suggestions that the definition of death be expanded to allow procurement from anencephalic infants23,24 and patients in the permanent vegetative state (PVS)25,26 involve a degree of sophistry unable to be accommodated under current laws and even if this were to change it is difficult to expect that there will be widespread public tolerance. It is indeed possible that such attempts are cumulatively jeopardising public confidence in the current programme in the manner of airing of previous concerns as to the accuracy of a diagnosis of death (Panorama, Transplants: are donors really dead?, BBC2, 13 Oct 1980).27
Strategies to increase cadaveric donor numbers
Efforts need to be directed therefore to either increasing the pool of the brain stem dead donor population or to reconsidering classical cadaveric retrieval of organs.
EXPANSION OF THE BRAIN STEM DEAD (BSD) DONOR POOL
Expansion of the BSD pool targets those factors that act as current restrictions, in the first instance generating the scarce resource of intensive care unit (ICU) beds to accommodate those likely to progress to BSD and ensuring professional motivation to encourage this. It must be accepted that if this exercise is conducted purely to that end, as in elective ventilation,28 although seemingly accommodated within codes of practice,29 practitioners would be considered as acting outside the law.30 The transplant services have also reconsidered in the light of shortage, expansion of donor criteria whereby organs previously considered unsuitable in view of age,31 dysfunction,32 or general disease33–35 are utilised. This practice clearly has an ethical dimension because of the inherent risk to the recipient and, in certain circumstances, the magnitude of the surgery.36 Although it has been customary to match poor donor with high risk recipient, this creates the greatest chance of worst outcome with inevitable consideration of efficient use of resources.37 Many different approaches have been taken to the high rate of donor loss of the potential or actual BSD such as compulsory requests, but an impasse is inevitably generated by the high rate of relatives’ refusal.
There still remains a discrepancy between expression of public willingness to donate and actual donation, with uncertainty as to the efficacy of education programmes.38
The introduction of presumed consent39–41 appears to have been effective in increasing donor numbers in other European countries,42,43 but carries the risk of organs being removed against a patients’ wishes,44 and public disquiet has led to repeal in other jurisdictions.45 Mandated choice has been considered as an alternative, promoting public awareness and allowing choice, whereby individuals engaged in official documentation such as a driving licence, passport, or income tax return would have to make a decision which would then be definitive, regardless of relatives’ wishes. The inherent risk with this practice is a reduction in available numbers, given previous evidence of the public being three times more likely to donate a relative’s organs rather than their own.46 A more recent proposal to encourage opting in has been the solidarity model,47 whereby those individuals who had previously agreed to donate would, in the event of requiring transplantation themselves, have priority over those who had refused. Whilst not without new ethical problems, this scheme would appear effective as an incentive, but it must be accepted that even with these proposals donor provision is not going to dramatically increase in the near future.
Certain countries have resourced programmes to address all the above procurement strategies with some success,48 but the realisation that this does not appear immediately reproducible in different settings has forced practitioners in the transplantation field to consider alternative sources of donor organs.
THE PROBLEMS ASSOCIATED WITH CLASSICAL CADAVERIC RETRIEVAL
Most organs do not tolerate the deterioration in cardiorespiratory performance that precedes all but sudden death, or the warm ischaemia that follows classical cardiorespiratory death. These factors were integral to the redefinition of death49 to include brain death and later BSD, whereby viable organs could thence be retrieved from the heart beating organ donor before any systemic deterioration. Retrieval from the non-heart beating organ donor (NHBOD) was virtually eliminated from Western practice from that moment in time.
ARGUMENTS IN SUPPORT OF NHBOD
Although reconsideration of this practice has been triggered by the donor shortage, the process could have certain ethically defensible drivers. Thus families, or indeed the patient, denied the opportunity to donate conventionally because the patient never fulfilled criteria for BSD, could access the “comfort” of benefit to others. The delay in waiting for progression to BSD to legitimise donation not only consumes expensive resources, but is demoralising for both family and staff, and is associated furthermore with secondary organ dysfunction50 and emerging evidence of graft dysfunction due to immunological activation of the donor organ.51 The maintenance of patients beyond the initial phase of severe brain injury simply to determine if they will progress to BSD may furthermore actually prevent that progression and beget long term family and societal problems by expansion of the permanent vegetative state (PVS) population. Procurement of organs after early withdrawal of care would avoid this later situation with its attendant ethical problems at the end of life.52 The practice of retrieval from the NHBOD, however, is not obviously weighted towards “good” and ethical validity.
ANALYSIS OF THE RECRUITMENT PROCESS FOR NHBOD AND KEY ETHICAL CONCERNS
The two main sources are the relatively “controlled” withdrawal of care in the critically ill (Maastricht category 3) and the “uncontrolled” scenario of either “dead on arrival” (category 1) or unsuccessful resuscitation (category 2).53 Each group brings its own ethical issues but certain concerns are common to all, not least the “conflict of interest” debate.
The inherent problem within this donor pool, of organs being particularly vulnerable to warm ischaemia, generates disquiet, not only regarding hazard to the potential recipient, but as to the approaches taken to reduce that warm ischaemia time (see table 2). This disquiet revolves around the definition of death and the process potentially being the immediate cause of death within the category 3 group. Conducting invasive procedures without consent or alternatively failing to act in the patient’s best interests (if the patient cannot be considered unequivocally dead) are key ethical concerns in categories 1 and 2. A further area of unease, particularly in category 3, is that whereas BSD is a definitive endpoint for the pathological process, withdrawal of care for the purposes of organ retrieval in the non-BSD patient is based on a medical value judgment, is clearly within medical control, and can be considered vulnerable therefore to a conflict of interests.
Strategies to improve the viability of organs from the non-heart beating donor
POTENTIAL HAZARD OF NHBOD TO THE RECIPIENT
Hazard to the recipient is demonstrated by the not unexpected finding that kidneys from NHBOD did not function as well as those from the beating heart donor.54 This raises questions as to the validity of the recipient’s consent if they are not provided with information in this regard, particularly when category 2 organs are implanted, primary non-function being in excess of 50% in certain series.55 Techniques are available to predict the viability of donor organs56 which provide some measure of safeguard, rendering it less than satisfactory when critical thresholds are ignored.55 Although improvements are continually being made to perfusion solutions and techniques such that outcome figures have improved57 and organs previously considered non-salvageable58 are functional after transplantation, the primary problem is the warm ischaemic time and it is the approaches to the reduction of this in all categories of patients that raise serious questions.
LEGITIMACY OF DEFINITIONS OF DEATH
A fundamental concern revolves around definitions of death and this needs to be placed in the context of debate over the last 40 years.
The recognition that medical advances could sustain cardiac activity whilst progression of intracranial pathology resulted in whole brain death, 59 generated a need to evaluate concepts of death. It can be argued that the redefinition of death49 to include this product of medical intervention was simply utilitarian, facilitating optimal organ procurement that could not be legitimately conducted on anything other than a cadaver. Aside from this vexed issue, however, the finality of brain death and the futility of ongoing supportive care is understood and accepted by a majority of the civilised world. The redefinition furthermore clearly established the need for death before organ retrieval.
A greater difficulty with definition has been created by cortical death after brain injury whereby spontaneous respiratory effort is retained in conjunction with cardiac activity, and long term survival is possible with nutritional support and general care. Whilst at the extreme end of the spectrum of PVS the patient will display a complete lack of sentience equivalent to the brain dead patient, leading to calls for a further redefinition of death60 and indeed utilisation for organ donation,25 the very fact that a spectrum of neurological deficit exists, negates the use of a term, death, which must be absolute to avoid discrediting the original expansion. Indeed, despite the immense dilemmas created by end of life decision making in this cohort of patients, no professional body61 or legislation62,52 has ever considered them other than alive.
Medical advances have also created problems in applying death as an absolute generic term in the context of traditional death. A clinical state compatible with classical death, characterised by unresponsiveness and absence of cardiac output and respiratory effort may within a short period of time reverse spontaneously (auto resuscitation) if due to a disturbance of cardiac rhythm, and may be reversed by interventional resuscitation over a slightly longer time frame with no neurological deficit. That clinical state cannot therefore be directly equated with classical death, regardless of the likelihood or inevitability over time of classical death without intervention. The patient could more accurately be described as dying rather than dead.
Resuscitation beyond a three to five minute watershed after classical death can also restore cardiac output and respiratory effort. Although, in the absence of protective factors, the patient will invariably demonstrate an extreme neurological deficit, they will, however, be defined as alive.
These factors are acknowledged within virtually all American states under the Uniform Determination of Death Act61 whereby death is defined by cardiovascular criteria only once it is irreversible. Although the main driver for the legislation appeared to be the protection of physicians using brain orientated criteria,63 the cardiovascular criteria appear unequivocal and it is against this template that the approach as regards NHBOD can be judged.
The Maastricht workshop64 considered that 10 minutes without perfusion of the brain was necessary before any intervention geared towards organ retrieval, and the Institute of Medicine recommended a five minute observation period.65 The Pittsburgh protocol66 sanctions surgical retrieval of organs at two minutes after asystole, which appears incompatible with the above statutory cardiovascular definition of death, whereby the loss of functions used to determine death should be irreversible.67 Furthermore, the possibility of sentience at retrieval,68 although remote, appears intuitively higher than for a case of established brain stem death and it must be accepted that medical practitioners have raised questions as to the latter possibility.69,27 Evidence to suggest that neurological functions considered irreversibly lost may be restored70 is likely to fuel such speculation, leading to public uncertainty and the possibility as previously described, of derailing the transplant programme in general (Panorama, Transplants: are donors really dead?, BBC2, 13 Oct 1980). Furthermore, the expansion of this procurement practice, with many units not having any or any approved policy65 would also serve to generate disquiet.
Practitioners at Pittsburgh have sought to answer criticism that irreversible loss of brain function would not have occurred at two minutes, with the arguments that irreversible lack of cardiorespiratory function is sufficient to certify death and that since the patient or family have refused resuscitation, the clinical state is clearly irreversible.71 It would be easy to dismiss this as professional sophistry were it not for the fact that outside the setting of organ donation, death is routinely, legitimately, and legally certified within the timescale of two minutes, in scenarios when death is expected, including after withdrawal of supportive care. Indeed, it would be considered unreasonable if families had to wait at least 10 minutes after asystole, apnoea, and unresponsiveness before the patient could be considered dead. It would appear somewhat illogical therefore if different criteria for cardiovascular death were applied dependent on whether organ retrieval was countenanced.
Although different definitions of irreversible and the different time scales described above are hardly conducive to public confidence, it is arguably more important to conduct the retrieval in a defensible manner than to manipulate definitions of death. Unfortunately, given that the Pittsburgh shorter period is solely for the benefit of the future recipient, it is inevitable that this will engender professional and public misgivings. If the patient is not considered definitively and irreversibly dead at two minutes, it can be argued that the process of organ procurement at that time becomes the cause of death, and that it is this which makes the condition irreversible.
APPRAISAL OF OTHER STRATEGIES USED TO DECREASE WARM ISCHAEMIA TIME
Other aspects of the process, namely that the timing, speed, and nature of the death generate comparisons with euthanasia, may reinforce the above concerns. Category 3 patients have to progress swiftly from withdrawal of care to asystole if organ function is not to be compromised. The most viable organs will come from a patient with significant brain injury but no serious damage to other systems, and by virtue of this, death in these circumstances is usually not rapid. Certain centres conduct trials of withdrawal of care to determine the likelihood of rapid decompensation72; this raises issues not least of consent. The major concern, however, relates to the pressure to achieve rapid retrieval within the described practice from Pittsburgh whereby the families have sanctioned NHBOD and said their goodbyes, the patient has been transferred to the operating theatre, and the surgeon and scrub team are waiting with the patient prepared with antiseptic. The acceptability in these circumstances of using analgesic agents with the predictable effect of depressing respiratory drive cannot be encompassed within the conventional backstop of double effect.73 The impact of agents given solely to optimally preserve organ function also generates concern in this regard. It can be argued that use of heparin as an anticoagulant is of little systemic consequence, but the capacity to aggravate bleeding carries the accompanying capacity to cause a deterioration in cardiovascular performance. The use of phentolamine, a vasodilator, is certainly open to questioning since the inevitable fall in blood pressure clearly has the potential to expedite death, particularly in the established critically ill.74 Such recommendations that are available75 allow interpretation of the word “harm” and do not advise absolutely against these agents in stating: “medications that do not harm the patient and are required to improve the chances of successful donation are acceptable”.
It would thus appear that elements of care towards the end of life demonstrate at best conflict of interest and at worst could fall within the definition of active euthanasia. To summons the protection of the principle of “double effect” by claiming that since donation benefits the patient and family by complying with their wishes, use of these agents is permissible,76 is an extreme example of professional sophistry.
Conflict of interest is also reflected in the converse practice of resuscitating those patients for whom life sustaining treatment is inappropriate or has been refused, when the procurement team is not ready or the family have not reached a decision.77 Although this would fall within the category of assault if consent had not been obtained, it could be argued that if the patient had expressed a wish to become a donor, this practice could reasonably be accommodated as a means of achieving that goal.
The practice of cannulation of the patient prior to withdrawal of care for the purposes of preservative perfusion is also open to varied interpretation and it is of note that this practice is not prohibited by the recommendations above.75 It could be argued that interventions of this nature would require an escalation of analgesic and sedative or anaesthetic agents with the potential for destabilisation of the cardiovascular system, thereby precipitating, or priming for, a more rapid death. This process too could not comfortably be contained within the principle of “double effect”.
Although the American approach comes with the redeeming feature of openness through publication, there are many areas of ethical disquiet, not least because of the diversity of process. It is difficult to determine whether other countries such as Holland and Japan adopt a uniform defensible template in their practice of controlled NHBOD and information from the UK is also extremely limited as to the extent and nature of practice.78
KEY PROBLEMS WITH PROCUREMENT STRATEGIES FROM CATEGORY 2 PATIENTS
The process of “uncontrolled” organ procurement as practised in Leicester, UK79 is, however, published. Patients admitted to the A&E (accident and emergency) unit with a history of cardiopulmonary arrest either outside or within the department were targeted. The entry criteria for inclusion in the procurement process were, in the absence of disease, an age below 65 years, and a period of circulatory arrest without basic life support of less than 30 minutes. It is not specified by which criteria resuscitation manoeuvres were discontinued, but death was certified by cardiovascular criteria. Once certified, the patient was moved to the A&E operating theatre where ventilation and cardiac massage were carried out either manually or mechanically (Thumper CPR System—Michigan Instruments). In the absence of the family to approach for consent a surgical cut down of the femoral vessels in the groin was conducted prior to insertion of a perfusion catheter into the aorta and the instillation of cold preservative solution. This process would be continued until the family could be contacted and asked for consent.
This category of procurement raises similar questions regarding a valid definition of death as outlined above in relation to category 3 patients. It is uncertain whether the law would consider the patient alive or dead but certain parallels can be drawn from the process of “elective ventilation”. It was stated in defence of that practice by the authors that the intervention of ventilation was initiated at the moment of death, with the actual diagnosis of death at some later stage by formal brain stem death testing.80 This flexible interpretation of death using different criteria was not considered sufficiently absolute and robust to contain the practice within the law and this viewpoint could equally be adopted with regard to procurement practice for the category 2 patient.
Concerns are generated not only regarding the validity of the diagnosis, but by the practice of cardiac massage and ventilation with 100% oxygen after the diagnosis of death, prior to the establishment of renal perfusion. Depending on the period of asystole, it is not inconceivable that re-establishment of cerebral perfusion may be associated with some restoration of brain function. Dilated unreactive pupils in the context of cardiac arrest may be attributable to the use of agents such as adrenaline and atropine, and even in the absence of these drugs, do not unequivocally predict a poor neurological outcome. This in turn raises questions as to a definition of death and the timing of such. If the patient is potentially alive, even though death is inevitable, the continuation of CPR (cardiopulmonary resuscitation), the surgical placement of aortic catheters and the administration of organ preservatives is clearly not in the patient’s best interests and constitutes an assault in a similar vein to “elective ventilation”. There is a paucity of statute covering this area but the common law position in England for the incompetent patient is that a doctor may only initiate and maintain treatment that is considered by professional opinion to be in a patient’s “best interests” and by invoking the doctrine of “necessity”.81,82 Given that within England no person or body has the authority to offer consent on behalf of an incompetent adult for any aspect of care, the stated consent of the family, coroner, and ethical committee described in the above publication would not carry legal validity.
If the patient could legitimately be considered dead, these interventions would acquire a different connotation. The Human Tissue Act 1961 allows for persons lawfully in possession of a body to remove parts for therapeutic purposes either with the expressed wishes of the deceased and/or in the absence of objection of relatives. The process of procurement described above does not comply with these directives. The interventions as a prelude to organ retrieval are seemingly outwith the definition of “removal” and in most cases the process is initiated without authorisation by patient or family. It is unclear whether interference with a corpse without legitimate authority would be considered a crime at common law, there being no property in a body. The courts do recognise, however, that whoever is responsible for disposal of the body does have a possession right83 and interference with this right could clearly create liability. Although this process cannot be viewed in the same vein as indecent interference, which the law will not allow,84 it could also be construed as mutilation, which although purposeful, may be actionable. The possibility also exists of the deceased’s relatives raising a claim for psychiatric injury, particularly if the interventions have been witnessed, a factor key to litigation success in previous cases.85 Even without these considerations it can be argued that although the general public may accept that a corpse cannot be harmed, respect for the dignity of the human body is likely to be widespread.86 This process could easily be interpreted as a lack of respect for the human body, the patient, and indeed any concerns that the family may hold, thereby engendering mistrust and antipathy towards the process of organ donation. Furthermore, the interventions prior to organ retrieval would appear to be based on “presumed consent” and it is possible to invoke the “slippery slope” argument that once this practice has become established and thereby accepted, progression to retrieval on this basis is not such a major clinical, ethical, or legal hurdle. Mistrust is a likely consequence of public awareness of this process.
CONCLUSIONS
It has been estimated that the number of donor organs could rise by 25% through the expanded use of NHBOD87 making it inevitable, in an era of universal shortage, that there will be pressure to procure from this cohort of patients. All transplant procurement strategies come with an ethical dimension but this particular process raises multiple concerns, not least of which is ambiguity as to the timing and definition of death. Given the disquiet with the concept of brain death88 it is difficult to see how the differences in interpretation described above can contribute to public and professional confidence. The need for rapid progression to cardiovascular death in category 3 patients to reduce the warm ischaemia time results in a range of practices which come uncomfortably close to accepted definitions of euthanasia without necessarily providing the ethical “good” of a death without suffering. Administration of large doses of analgesic/sedative/anaesthetic agents once the withdrawal/dying process was initiated would achieve this latter goal and could be accommodated within the law if titrated against neurological monitoring modalities.89 It is difficult to predict, however, the professional and public response to this, one interpretation being that public confidence would increase with the knowledge that even with rapid procurement, practitioners could guarantee freedom from awareness and any suffering, and indeed, bring an inevitable death to a swifter conclusion. The alternative interpretation of practitioners becoming engaged in a process close to euthanasia may actually engender even more distrust.
Procurement from category 2 patients raises in addition to the above the issues of non consensual treatment and the possibility of return of cognitive function. Since animal models have demonstrated recovery of neurological function after 11 minutes of circulatory arrest90 this possibility cannot be discounted, also warranting discussion on the desirability and acceptability of administration of large dose anaesthetic agents and/or neurological monitoring.91 Recent evidence that cerebral protective strategies improve outcome after cardiac arrest92 has the further potential to raise questions of conflict of interests whereby resuscitative attempts may not be pursued so rigorously, rendering it mandatory for public confidence that criteria for irreversibility be more specifically defined. Given difficulties in identifying futility within the intensive care setting, the spectre of conflict of interests will also linger for the category 3 patients.
Non-heart beating organ donation/donors can be considered an ethical “good” in meeting an individual’s wishes during life, providing some comfort to the family, improving the quality of life of the recipient and for certain organs, reducing the costs of replacement therapy and thereby benefiting society.
If, however, society, and indeed the medical profession, is to wholeheartedly subscribe to this process and achieve this ethical “good”, the above inconsistencies, ambiguities, and irregularities need to be eliminated, clarified, or endorsed in an explicit, transparent format.
In such a system, “consent” for all components of cadaveric donation would, to everyone’s benefit, reflect the informed will of the public rather than legalise or sanction the tactics of the transplant service.
REFERENCES
Linked Articles
Other content recommended for you
- Death, dying and donation: organ transplantation and the diagnosis of death
- Individual choice in the definition of death
- Dignifying death and the morality of elective ventilation
- Elective ventilation and the politics of death
- Elective non-therapeutic intensive care and the four principles of medical ethics
- Brain donation for schizophrenia research: gift, consent, and meaning
- Proceeding with clinical trials of animal to human organ transplantation: a way out of the dilemma
- Emergency medicine, organ donation and the Human Tissue Act
- Depictions of ‘brain death’ in the media: medical and ethical implications
- Ethical considerations in the application of preconditioning to solid organ transplantation