Adrenal insufficiency after treatment with fluticasone
BMJ 2002; 325 doi: https://doi.org/10.1136/bmj.325.7368.836/a (Published 12 October 2002) Cite this as: BMJ 2002;325:836
Second line controller treatment might have been tried
- Brian J Lipworth, professor of allergy and respiratory medicine (topdoc{at}brianlipworth.com)
- Ninewells Hospital, Dundee DD19SY
- Department of Paediatrics, Regional Hospital of Bolzano, Italy
- Paediatric Department, University of Verona, I-37134 Verona, Italy
- Al Mishari Hospital, PO Box 300145, Riyadh 11372, Saudi Arabia
- Booth Hall Children's Hospital, Manchester M9 7AA
- BMJ
EDITOR—The lesson of the week from Drake et al highlighted iatrogenic adrenal suppression due to high doses of fluticasone in children.1 The real lesson here is not to use drugs off label without having any other alternative or being aware of the potential adverse effects.
It is unclear from the report whether the prescribers told the parents of these children of the potential for developing adverse effects at five to seven times the maximum recommended dose in children (>200 ¼g/day of fluticasone). Presumably the prescribers were aware of the decline in the therapeutic ratio above 200 ¼g/day but had weighed the potential benefits against the risks in each specific case, even though no data indicate any efficacy gain above this dose in children. It is not stated in the report whether any attempt had been made to step down to a lower dose, or whether second line non-steroidal controller treatment had been tried before increasing to such high doses.
It would also be relevant to know about the children's lung function before admission as the lung bioavailability of fluticasone is directly correlated to predicted forced expiratory volume in one second, such that systemic absorption would be reduced in more severe asthma.
This report should not detract from using appropriate low doses of inhaled corticosteroids, including fluticasone, in asthmatic children as they have a high therapeutic ratio at conventional labelled doses.2–1 Their use above such doses may result in patients falling off the precipice of the systemic dose-response curve.
Footnotes
-
Competing interests BJL has received financial support for clinical trials, attending postgraduate meetings, staff training and equipment from companies who make inhaled steroids, including GlaxoSmithkline, AstraZeneca, 3M Healthcare, Aventis, Schering Plough. The mother and spouse of the author have shares in GlaxoSmithKline, which makes fluticasone
Data on fluticasone are reassuring but what about doctors' prescribing?
- Lydia Pescollderungg, doctor,
- Angelo Pietrobelli, doctor (attilio.boner{at}univr.it),
- Attilio L Boner, professor
- Ninewells Hospital, Dundee DD19SY
- Department of Paediatrics, Regional Hospital of Bolzano, Italy
- Paediatric Department, University of Verona, I-37134 Verona, Italy
- Al Mishari Hospital, PO Box 300145, Riyadh 11372, Saudi Arabia
- Booth Hall Children's Hospital, Manchester M9 7AA
- BMJ
EDITOR—Drake et al reported on four asthmatic children with symptomatic hypoglycaemia caused by high dose and long term treatment with inhaled fluticasone propionate and concomitant infectious disease.1 Children received 500-1500 ¼g fluticasone daily for 16 months to five years. Despite this high dosage, linear growth was linear even if below that predicted from parental height. Inhaled corticosteroids are well known to cause only temporary slowing of growth in children. Properly used in the recommended doses according to the severity of the disease, inhaled corticosteroids do not prevent the attainment of normal adult height.2 According to this report, the four children in the cases described by Drake et al will also probably reach their expected adult height—if they survive their doctors' prescribing.
The case reports do not provide any information on the severity of asthma in these subjects. Overtreatment with fluticasone was likely since after the hypoglycaemic episodes all children tolerated a dose reduction and, in case 1, fluticasone withdrawal without any reported deterioration in the asthma. Overdosing on inhaled corticosteroids in children (up to a dose of 4800 ¼g/day beclomethasone equivalent) has been documented in the BMJ, even if it was previously reported that most of the therapeutic benefit of inhaled fluticasone is achieved with a total daily dose of 100-250 ¼g. 3 4
Overtreatment is likely to be associated with normal airway capacity and with consequent greater systemic absorption of the drug throughout the lung. The consequence of this is a greater likelihood of side effects.5
Footnotes
-
Competing interests ALB has received research funds from GlaxoSmithKline for a member of staff and for consulting.
Dose-response curve should have been highlighted
- Abdullah Sh Mohamed, consultant physician (chest) (inawalaleye_4{at}hotmail.com)
- Ninewells Hospital, Dundee DD19SY
- Department of Paediatrics, Regional Hospital of Bolzano, Italy
- Paediatric Department, University of Verona, I-37134 Verona, Italy
- Al Mishari Hospital, PO Box 300145, Riyadh 11372, Saudi Arabia
- Booth Hall Children's Hospital, Manchester M9 7AA
- BMJ
EDITOR—The article by Drake and accompanying commentary miss the point.1 The main problem is the enormous doses of fluticasone for chronic asthma over long periods in these children. The authors concentrated on the hypoglycaemia, but growth stunting was noted too.
Drake et al would have served their readers better if they had highlighted the dose-response curve of inhaled fluticasone. In adults and adolescents 80% of the therapeutic benefit of 1000 ¼g/day dose is achieved at a dose of 70-170 ¼g/day, well within the maximum licensed dose for children (200 ¼g/day).2 Moreover, the maximum therapeutic benefit in these groups was achieved at 500 ¼g/day after plateauing at 100-200 ¼g/day. The dose-response in relation to systemic effects remains linear.3
Whether prescribed by a respiratory specialist or a general practitioner, these massive doses of inhaled corticosteroids for chronic asthma, in children and adults, should be relegated to the past.4
Footnotes
-
Competing interests ASM has been reimbursed once by GlaxoSmithKline for attending a symposium.
Lowest possible dose of inhaled glucocorticoids should be given
- Leena Patel, senior lecturer in child health (lp{at}man.ac.uk),
- Peter E Clayton, professor of paediatric endocrinology
- Ninewells Hospital, Dundee DD19SY
- Department of Paediatrics, Regional Hospital of Bolzano, Italy
- Paediatric Department, University of Verona, I-37134 Verona, Italy
- Al Mishari Hospital, PO Box 300145, Riyadh 11372, Saudi Arabia
- Booth Hall Children's Hospital, Manchester M9 7AA
- BMJ
EDITOR—Drake et al did not mention whether their patients had weight loss and fatigue, but it is notable that they did not have cushingoid features despite having significant suppression of the hypothalamopituitary-adrenal axis from exogenous inhaled glucocorticoid.1 We have also observed that features of adrenal insufficiency—including impaired growth, poor weight gain, fatigue, and hypoglycaemia—predominated over the peripheral effects of excess exogenous glucocorticoids in eight children with asthma.2 Three of these had received inhaled glucocorticoids other than fluticasone, and only one had had doses higher than 600 ¼g/day.
Several explanations have been put forward for this phenomenon of symptomatic adrenal insufficiency. 2 3 One explanation is abrupt withdrawal or reduction in the dose of exogenous glucocorticoid associated with non-compliance, especially during intercurrent stress, in patients with inadequate adrenocortical reserve. 2 3 We believe that most patients receiving treatment with chronic inhaled glucocorticoids who default occasionally on their drug treatment are less likely to have profound suppression of the hypothalamopituitary-adrenal axis, akin to patients receiving prednisolone on alternate days. Our patients were reportedly compliant with their inhaled treatment, and this may have resulted in persistent adverse effects on the axis.
In his commentary Hindmarsh suggests a lack of endogenous or exogenous glucocorticoid at certain times of the day.1 This might occur with beclomethasone dipropionate,3 but it is unlikely to occur with fluticasone, owing to its longer elimination half life and greater steady state accumulation with repeated dosing. We also believe that the insidious weight and growth failure documented in our patients implies that cortisol deficiency was present for more than a few hours per day. Presentation with hypoglycaemia (in two of our patients) was an acute episode on the background of a chronic problem.
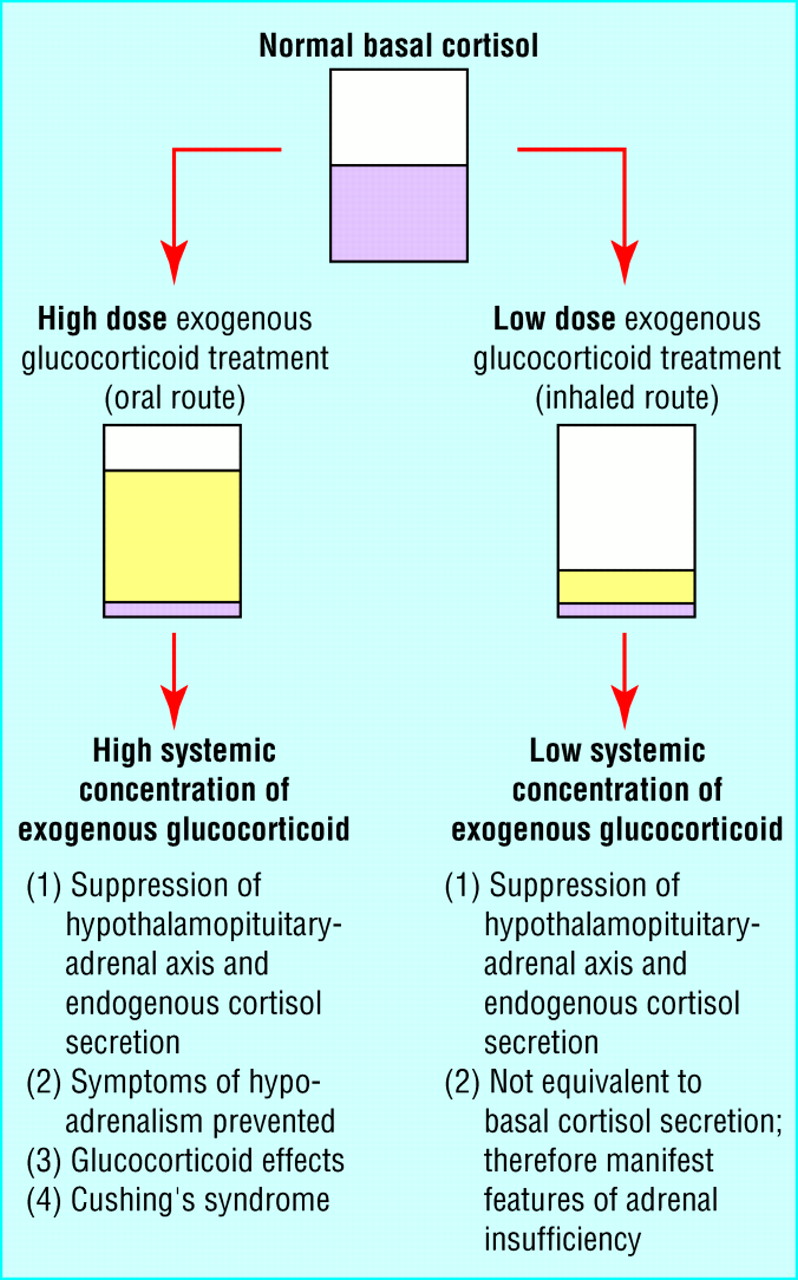
We think that this phenomenon of symptomatic adrenal insufficiency during treatment with inhaled glucocorticoids is likely to be influenced by individual sensitivity to glucocorticoids and differential tissue and possibly drug sensitivity, with greater effects on the hypothalamopituitary-adrenal axis than other tissues (figure).

Differences between Cushing's syndrome and paradoxical adrenal insufficiency with inhaled glucocorticoids
{kind=link}
However unusual and rare this complication might be in the context of the many children treated with inhaled glucocorticoids who do not experience any adverse systemic effects, adrenal insufficiency is potentially life threatening, and general practitioners and paediatricians need to be aware of it. 2 4 Presentation may be acute with hypoglycaemia or insidious with poor weight gain, poor growth in height, and fatigue. We emphasise the importance of using the lowest effective dose of inhaled glucocorticoid, stepping down when asthma is controlled, and regularly monitoring growth and assessing function of the hypothalamopituitary-adrenal axis in children with growth failure.2
Footnotes
-
Competing interests LP has been reimbursed by AstraZeneca and GlaxoSmithKline for attending conferences.
Summary of rapid responses
- Birte Twisselmann, technical editor
- Ninewells Hospital, Dundee DD19SY
- Department of Paediatrics, Regional Hospital of Bolzano, Italy
- Paediatric Department, University of Verona, I-37134 Verona, Italy
- Al Mishari Hospital, PO Box 300145, Riyadh 11372, Saudi Arabia
- Booth Hall Children's Hospital, Manchester M9 7AA
- BMJ
EDITOR—The lesson of the week by Drake et al prompted 10 electronic responses, eight of which came from respondents with links to pharmaceutical companies—six to GlaxoSmithKline, manufacturers of fluticasone, one to AstraZeneca, manufacturers of budesonide, and one to both.1 Consequently, much of the correspondence is devoted to explaining the respective advantages or disadvantages of one drug over the other.
Mike Devoy and Yvonne Greenstreet, as well as Peter Daley-Yates—all employees of GlaxoSmithKline—argue that fluticasone has less of an effect on the hypothalamopituitary-adrenal axis than budesonide at clinically equivalent doses. This is because differences in systemic exposure are related to bioavailability and not lipophilicity, tissue distribution, or half life of a drug. Devoy and Greenstreet further point out that it affects children's growth less than budesonide. Cathy Jackson, a shareholder in GlaxoSmithKline, remarks that the inhaler device should have been specified as this determines the suppression of the hypothalamopituitary-adrenal axis.
Lars-Géran Carlsson, Bengt Lindberg, and Jarl Ingelf, who work for AstraZeneca in Sweden, counter that water soluble steroids such as budesonide are more rapidly eliminated. Thus fluticasone's suppression of the hypothalamopituitary-adrenal axis was three times that of budesonide in a dose-response study in children.
Nearly all respondents thought that the high dosage may have caused the adrenal crisis. Ranjan Suri and Sheila Mackenzie from the Royal London Hospital even ask for the evidence that children had asthma that merited treatment with inhaled corticosteroids because patients with mild asthma do not need such treatment and are more likely to be sensitive to side effects.
Most respondents argued that the lowest possible dose should be used. Lipworth (letter above), Devoy and Greenstreet, and Minna Kaila, a paediatric allergist from the University of Tampere, Sweden, point out that, instead of high doses of steroids, long acting — agonists or leukotriene receptor agonists should have been given as second line treatment.
References
- 1.↵