Article Text

Statistics from Altmetric.com

Liverpool fans desperately trying to escape the crush in the terraces.
“Dr Venables from Sheffield on the phone for you, he says you are old friends”. My secretary Jane transferred the call to me, and so it began. Graham asked if I could take a young man from Keighley, who had been injured at the Hillsborough football stadium in Sheffield on 15 April 1989. The Football Association Cup semi-final that afternoon, between Liverpool and Nottingham Forrest, had been abandoned soon after kick off, when hundreds of Liverpool fans were crushed in fenced pens at one end of the ground. The disaster had been seen unfolding live on TV. Airedale General is Keighley’s hospital, and at that time I was responsible for the physical rehabilitation service. The young man’s name was Anthony Bland, he was 18 years old, and he had suffered severe anoxic brain damage when his chest was crushed. Graham said that after a few days ventilation he had been able to breathe unaided, and once extubated, appeared to be in a vegetative state.
Tony Bland was transferred to us in May. He was unresponsive, with open eyes and all the features of the vegetative state.1 His parents, older sister, and other family members came to hear what was planned. After outlining what we would do to try to prevent complications and encourage recovery, I explained that because he had suffered severe brain damage it did not look hopeful, but we would do our best. Graham had already begun breaking the bad news. The police liaison officer assigned to the family came to see me, and asked to be kept informed of Tony’s progress. Soon afterwards, the local and national press heard that a “Hillsborough victim” was at Airedale and asked for information.
Despite the rehabilitation team’s best efforts, which included getting Tony into our therapy pool with the help of his father, careful nursing, and regular attention from a rota of family members, there was no improvement. He remained unresponsive. There was no eye contact and no sign of communication. After three months his family could see that there had been absolutely no change, and said so. The CT scan showed cortical atrophy (fig 1) and his EEG was flat. I told the family again about the vegetative state, and that recovery was less and less likely as time passed without improvement. Realising that nothing more could be done, they questioned why we should go on.
The American Academy of Neurology (ANN) had just published a guideline on the management of the vegetative state.2 There had also been a President’s Commission Report in 1983 and a Canadian Law Reform Report in 1984. All recommended allowing treatment withdrawal, including nutrition and fluids.3 I showed the AAN report to Mr and Mrs Bland and discussed treatment withdrawal with them and the team. It seemed to all of us that no purpose would be served by continuing treatment, including artificial nutrition and hydration (in the USA ethics texts call it “medical nutrition and hydration” whereas in the UK and Australia “artificial” is more common). Tony was not conscious, and was extremely unlikely to recover consciousness, so could never have any semblance of normal human life. We talked about stopping treatment. Tony’s family and everyone in the care team were agreed. We set a date to withdraw all life prolonging treatment, including artificial nutrition and hydration, while continuing comfort care and support
HILLSBOROUGH AND THE MEDIA
While the Bland tragedy was quietly unfolding in Airedale, Lord Justice Taylor was holding a Home Office Inquiry into the Hillsborough disaster.4 Many newspapers had printed allegations, later shown to be lies, about the behaviour of the Liverpool football fans outside and inside the ground. The Sun newspaper, with its banner headline “THE TRUTH”, was the most offensive. Five years later, the Nottingham Forest manager Brian Clough and Margaret Thatcher’s Press Secretary, Bernard Ingham, reiterated the allegations.5 It was widely assumed that the Liverpool fans were to blame for the tragedy, while the survivors and the families of the dead held the police responsible for allowing people to walk, unstewarded and unpoliced, down a tunnel with a 1 in 6 gradient into the back of already overcrowded pens. The pressure on those at the front was like a slow turning vice–96 men, women, and children died. The facts concerning what happened that day were distorted and persistently misrepresented in the media.6 Lord Taylor’s conclusion that “the real cause of the Hillsborough disaster was overcrowding” and “the main reason for the disaster was the failure of police control” was ignored (see paragraphs 311 and 278).6 The frustration, anger, and distress endured by the survivors and the bereaved families are beyond my imagination. Their loss and suffering was exacerbated by a partial process of investigation, lack of disclosure of evidence, the conduct and outcome of the inquests, and the misrepresentations in the media (for a full account of the circumstances of the disaster, the aftermath and the legal processes, see –Scraton5). To this day the Sun newspaper is hardly bought on Merseyside.
THE CORONER’S LETTER
With all this furore going on and a police investigation into the disaster underway, I decided to inform the Sheffield Coroner, Dr Popper, of our plan to withdraw all treatment, including artificial nutrition and hydration. It is difficult now to convey my shock on receiving his intimidating reply. Having stated that he had no jurisdiction over any living person, he advised that I would risk a murder charge should I withdraw treatment. He made it clear that he “… could not countenance, condone, approve or give consent to any action or inaction which could be, or could be construed as being, designed or intended to shorten or terminate the life of this young man. This particularly applies to the withholding of the necessities of life, such as food and drink”. He requested a reply by return indicating that I had understood his opinion, and that I would not withdraw treatment. He advised me to contact my medical defence society and the Regional Health Authority (RHA) solicitor. He sent copies of his letter to the Chief Constable of the West Midlands Police, the Force investigating the disaster, the Yorkshire RHA solicitor, and my defence society. On the following day I was visited at the hospital by a detective from Keighley Criminal Investigation Department (CID). He informed me that if I withdrew treatment and Tony died, I would be charged with murder. He was reluctant to do this as he had heard I was a “decent fellow”.
How naïve I was, how little I knew about the law. I assumed that if treatment had been withdrawn in similar circumstances in America and Canada, and if all those closely concerned were convinced, after careful thought and discussion, that it was morally right, then we could and should go ahead. Mr and Mrs Bland were in total agreement with the team. They were angry and even more disheartened by the threat of prosecution. Certain that their son would not have wanted to be kept alive in a vegetative state and beyond recovery, they saw no purpose in continuing the treatment.
Thousands of words have since been written about the case, eight judges gave opinions, moral philosophers and law experts discussed the judgments, religious leaders pronounced. Yet neither the family nor I understand why it was all so complicated. It seemed simple then and it seems simple now. (For the judgments see Airedale NHS Trust v Bland 1993 1 All ER 821 HL, which also provides references to the appeal Court and Family Division hearings. For a selection of writing on the case see: Institute of Medical Ethics working party8; Finnis9; Kelly10; House of Lords11; Singer12; Harris13; Royal College of Physicians14; McLean15; Jennett16.)
LEGAL ADVICE
We were advised by the Medical Protection Society and the Regional Health Authority solicitor to apply to the High Court for an order declaring that treatment withdrawal would not be unlawful. One lawyer said to go ahead and withdraw, because no jury would convict, but for me the idea of months suspended from work, press attention, a trial for murder, and a General Medical Council hearing was not an attractive option. The Blands could not understand why the courts should be involved, and were unwilling to agree to the Airedale Trust making an application to withdraw treatment. Their sadness at the appalling circumstances that had taken their son, and their anger at the handling of the aftermath of the Hillsborough disaster, was so profound that they just could not contemplate any further involvement with authority or the media. Tony’s care and treatment continued. Gradually his limbs became more contracted, but at no time was there any sign of awareness or communication. His mother and sister began to find it difficult to visit. His father had nightmares about his son, and the care team became disheartened.
His mother and sister began to find it difficult to visit. His father had nightmares about his son, and the care team became disheartened
The Hillsborough disaster continued to make news, but at Airedale we kept quiet and got on with our work. From time to time journalists enquired about Tony’s progress and Mr Bland and I gave comments. In January 1991 the Institute of Medical ethics published a report concluding that it was morally justified to withdraw artificial nutrition and hydration from patients in the persistent vegetative state (PVS).8 Soon after, Granada TV broadcast a discussion programme on end of life issues. Mr Bland, Professor Bryan Jennett, and I took part, as did Nicholas Winterton MP (Member of Parliament) who contacted the Minister of Health, Virginia Bottomley, who passed the matter to the Home office. At the same time, Keighley’s MP, Gary Waller, asked for legal clarification, and subsequently attempted to introduce a Private Members’ Bill that would have allowed treatment withdrawal. In December 1991 the Right Hon John Patten MP wrote from the Home Office that the Government had no plans to change the law; that withdrawing treatment, even to relieve suffering, would constitute murder or manslaughter. He stated that the law existed to protect the weak, the disabled, and the elderly. Parliament could not decide that a person’s life was not worth living. He noted that the matter had been reviewed by the 1980 Criminal Law Revision Committee which had rejected proposals to “relax” the law in this area.
In September 1991 BBC Radio 4 included an interview with Mr Bland and me in a File on Four programme about euthanasia. We took part in a TV discussion programme on the day of the April 1992 general election. In June 1992 John Waite made a Face the Facts programme for Radio 4 about PVS. The programme examined the problem thoroughly, and compared our situation with a PVS case in Scotland where treatment had been withdrawn following the Procurator Fiscal’s advice that such a decision would not be inappropriate (Scotland has a different legal system from England). That case had been highlighted by Professor Jennett and Clare Dyer in a BMJ article contrasting the American and British legal positions.17 It was even suggested that we move Tony to Scotland and withdraw treatment there. Mr Bland, while unwilling to support an Airedale Trust application to withdraw life prolonging treatment, was quite willing to comment and, in his own way, campaign for what the family felt should be allowed to happen to his son. I agreed and joined Mr Bland in interviews on radio, television, and for the newspapers. Tony’s condition did not change. There was no sign of an end to this dreadful situation.
After Face the Facts I was contacted by Ann Sommerville, Secretary of the British Medical Association (BMA) Medical Ethics Committee. The Committee was preparing a statement on PVS and had contacted the Crown Prosecution service (CPS) to ask about our case. The CPS took the view that treatment withdrawal was the same as “euthanasia” and, therefore, murder. However, the Official Solicitor offered to provide guidance on seeking a declaratory statement. He advised that Airedale’s lawyers should seek a declaration in the Family Division of the High Court that withdrawal of medical treatment was lawful and in the patient’s best interests. This would be handled in the same way as previous medical cases, such as those involving sterilisation of incapacitated adults and treatment withdrawal in severely ill newborns. By going to the Family Division press coverage could be minimised or avoided. The outcome would not be certain; the court might decide that withdrawal was unlawful. It was clear that the Official Solicitor wanted the legal problem of treatment withdrawal in PVS decided.
I explained all this to Mr and Mrs Bland. While they were considering what to do, Tony developed a urinary tract fistula and septicaemia. Neither my surgical colleague nor I wished to operate, and the ensuing crisis helped me to persuade the Blands to let Airedale Trust make the application to withdraw life prolonging treatment. From that moment things moved very fast and media pressure became intense. First, the RHA solicitor put me in touch with a barrister who discussed the case in general and the surgery in particular. On his advice we went ahead with the operation and treated the infection. He met Mr and Mrs Bland with me, and discussed what to do next. I informed Ann Sommerville that we were going ahead and the Official Solicitor’s counsel contacted our lawyer and the RHA solicitor, forwarding a large bundle of documents about treatment withdrawal cases in other jurisdictions. Our barrister visited Tony and was visibly shocked by the experience.
Word got out that we were going ahead with an application to the Family Division to withdraw treatment. On the evening the story broke the hospital switchboard was jammed. All press calls were rerouted to the RHA press office to allow the hospital to continue to work. While our barrister prepared a skeleton argument, the Official Solicitor–acting for Tony Bland–asked four independent experts to examine him and report on his medical condition. Two were “for” our side and two “for” the Official Solicitor, who was opposing treatment withdrawal. Professors Bryan Jennet and Peter Behan, Dr Niall Cartlidge, and Dr Keith Andrews visited Airedale and wrote reports, agreeing that Tony was in a vegetative state and that there was no prospect of recovery. In advance of publication in the New England Journal of Medicine, Bryan Jennet obtained the report of the PVS Task Force, with good long term follow up data showing that there were no late recoveries of awareness.18 This was submitted in evidence along with the BMA Ethics Committee report. We were given a date for a hearing at the High Court in London. Mr Bland and I were to give evidence, and the experts would be cross examined.
The Blands and I received sacks of mail. For the Bland family it was almost all sympathetic and supportive
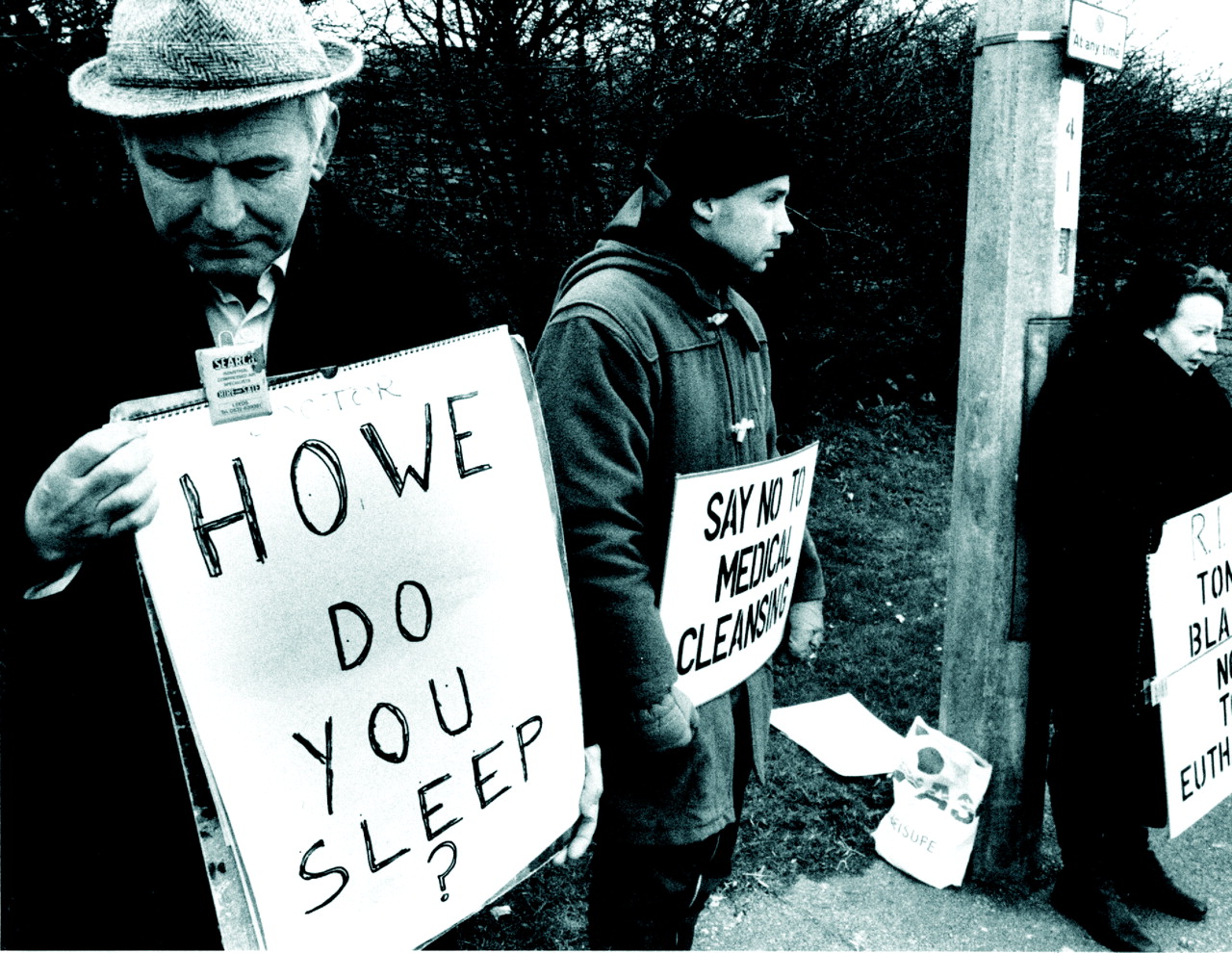
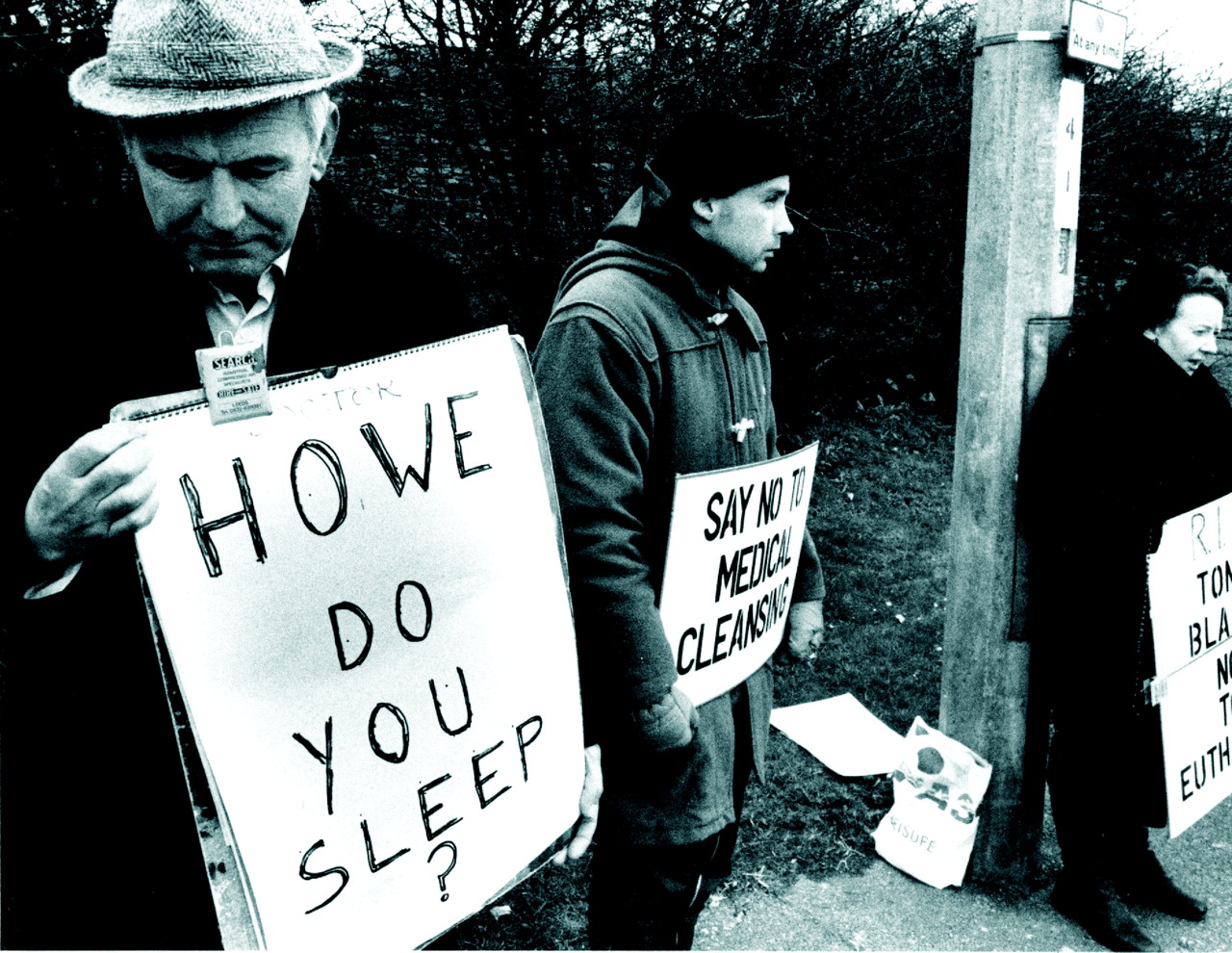
PROTESTS
The hospital was picketed by pro-life campaigners. One banner read “Howe do you sleep?” (fig 2). Another proclaimed “Say no to medical cleansing”. Local people told the protesters in plain language to leave their hospital staff alone and go away. From then, and through the three court hearings, the Blands and I received sacks of mail. For the Bland family it was almost all sympathetic and supportive. The most moving letters were from people who had experienced the horror of a relative in the vegetative state, and who wished they had been able to see it end more quickly. An occasional letter criticised treatment withdrawal. Letters ran more than 10:1 in favour of withdrawal. The nurses also received letters of support, as well as flowers. A number of people were worried about how we could be so sure there would be no recovery and no suffering. With my secretary’s help I replied to all, explaining what PVS was, and how we could be sure there could be no recovery. Some wrote back to say their worries had been relieved by the information. There were a few bizarre letters suggesting curative treatments, such as plasma infusion recommended with increasing hysteria after each court hearing by a retired pathologist.
I expected abuse and was not disappointed. One disturbing letter came with “BY FIRST CLASS RECORDED DELIVEY” typed on the envelope and in the letter, and addressed personally to me at Airedale Hospital, 47–51 Crumlin Rd, Keighley (Crumlin Road is a well known street in Belfast, but no such name exists in Keighley). It was from a “Professor T Hansen et al”. From an address in London the professor wrote that His Excellency, the Medical Vocation Commissioner (MVC) for the District of British Isles had asked him to inform me that I was involved in a conspiracy to murder Tony Bland. The letter continued: “nothing and nobody on earth will be able to save you, the chairman of the Airedale NHS Trust, the Chief Medical Officer Calman and Virginia Bottomley from the harshest prison terms imaginable for practising concentration camp medicine”. I was exhorted “to not be a bloody fool and do not go ahead with taking Tony Bland’s life, A MURDER MOST FOUL”. The letter stated that my name was on “THE WATCH LIST” and that copies had been sent to the Pope and Boutros-Ghali, the Secretary General of the United Nations. My sympathy was with Virginia Bottomley, the Health Minister, for she clearly said the matter was not for the Health Department, but for the criminal law. As a dire warning Hansen pointed out that after Mr Christopher Patten crossed swords with the MVC, he had lost his seat in parliament, found himself unemployable in London, left for the job in China, and was now fighting a cardiac death. Mr Patten and the rest of us are still alive and well.

Tony Bland (courtesy of the Bland family).
Jack Scarisbrick, chairman of the charity Life Cares, offered to remove Tony from hospital and care for him for the rest of his natural life. Some writers called me a murderer and said I was not fit to be a doctor. Father Morrow, a priest who had been one of the protestors at the hospital gates, announced that he would obtain an arrest warrant for me, on a charge of murder, should Tony die. The loveliest letters were from former and present colleagues, some far away, and one of the nicest was from the ward sister where I first worked after qualification at the City Hospital, Belfast.
DEALING WITH THE MEDIA
The RHA press officer protected us from the media by handling all calls, and organising and limiting interviews and statements. The Blands agreed to publish their story in one newspaper and this protected them from unwelcome attention by the rest. People stopped me in shops and on the street offering support and sending good wishes to the family and the nurses. Clinics gradually lengthened as the patients offered support and criticised the protesters, discussed ethics and law, and asked to make plans for their end of life care. The level of compassion shown was very touching and very helpful. All the reporters who interviewed us were considerate and concerned about the family and staff. Some critical articles were published, including one by Melanie Phillips in the Guardian, which likened the decision to withdraw treatment to Nazi “euthanasia”. The editor printed my reply, but under the unhelpful and indeed misleading heading of “Patients left to die every day”. The marked contrast between the reasonable way we were treated by the media and the onslaught on the Liverpool fans puzzles me still.
There were irritating aspects to some interviews, which often went over the same worries expressed in the letters: certainty of outcome, lack of awareness, and mode of death. Many reporters and commentators repeatedly asked about “euthanasia”, the assumption being that allowing treatment withdrawal in PVS would open the floodgates to wholesale murder of helpless people. With few exceptions, it proved impossible to get them to understand that treatment limiting decisions were made in intensive care, cancer care, and so on every day, in every hospital. Few were willing to seek clarity about voluntary medically assisted suicide, involuntary killing, or allowing to die. Nor, despite strenuous efforts, would they report what John Harris called “The Government’s euthanasia programme”19; not one reporter, interviewer, or programme maker took up the suggestion that they would be better investigating the undisputed fact that thousands of people die prematurely because of government decisions, than trying to link PVS to mercy killing, or whatever else they interpreted as euthanasia. The examples I gave were the lack of dialysis facilities in the UK and the death toll from failing to ban smoking in public places. I told them that many people with renal failure, who could live a much better life on dialysis than someone in PVS, were never dialysed. Further, the victims of these decisions certainly do not give informed consent, and by no stretch of the imagination are the voters fully consulted on these issues at elections. As Harris pointed out, this is a much larger problem than voluntary assisted suicide or PVS. My efforts were politely ignored.
THE COURT HEARINGS
Just before the first court hearing in November 1992 we were told that since our barrister was not a QC (Queen’s counsel), while Mr Munby, appearing for the official solicitor was, a QC would be appointed to appear for the Airedale NHS Trust. The day before the hearing we met the new man at his chambers in London. He was fully briefed on all the issues. The President of the Family Division, Sir Stephen Brown, heard the case, and decided that it would not be unlawful to withdraw treatment. The Official Solicitor appealed and a date was promptly given for that hearing. The Court of Appeal disallowed it, but granted leave to appeal to the House of Lords and the case went ahead quickly.
The Family Division hearing had been my first experience of a high court in action, and I took annual leave and went to the Lords to watch the final hearing in December, which was fascinating. At appeal only the lawyers and judges are involved, no witnesses are called. As everyone was leaving court during a break in proceedings one of the lawyers asked if I found the discussions interesting. I admitted fascination and bafflement at some of the arguments. He said that he wished their Noble Lordships would stop going on about parliament reforming the law on PVS, because MPs were not capable of deciding something as important and complicated as this. His words rang true when Mrs Winterton MP tried unsuccessfully to overturn the Lords’ decision with a Private Members’ Bill that would have made it illegal to remove artificial nutrition and hydration from any patient under any circumstances. During that debate, there were thoughtful contributions from MPs who were medical doctors, but many speeches displayed a profound lack of understanding.
TONY’S LAST DAYS
Once the final decision was announced, we asked for, and received, a news blackout. The press left us alone on the understanding that after Tony died we would hold a press conference. Not so the protestors. First, they leafleted cars in the hospital car park, then some of them burst onto the ward shouting that the staff were murderers. The ward sister bundled them out very quickly and the police were called. From then on we had a security guard at the ward door, and Mr and Mrs Bland stayed in the hospital to avoid any doorstepping of their home.
His death was peaceful and his parents were with him when his breathing stopped
In March 1993 all life prolonging treatment was stopped. Tony sank into an eyes closed coma, then signs of renal failure appeared and he died of bronchopneumonia nine days after withdrawal, with his parents by his side. Good nursing care ensured that he looked peaceful to the end, the mode of his death appeared no different to other deaths in hospital. In the application, we had stated that the feeding tube would be left in place in case drugs were needed, but none were. About four days after we had stopped using the tube one of the nurses asked why we did not just remove it. This seemed like a nice idea, especially since it was clear that it was not needed. We took out the feeding tube and the urinary catheter, and removed every piece of medical equipment from the room. When Mr and Mrs Bland came back to sit with their son, they looked around the room in amazement and then Mr Bland said, “That is the first time he has looked like our Tony since the day he left for sheffield”. For the first time in my working life I realised how intrusive medical kit can be. His death was peaceful and his parents were with him when his breathing stopped. Mr and Mrs Bland believe that their son died at Hillsborough in 1989.
The following morning a press conference went ahead at the hospital. An inquest was held in Bradford, and the protestors were outside jostling with reporters as we came and went. The pathology report showed that there had been almost total destruction of the whole of the cerebral and cerebellar cortex (fig 3). But father Morrow continued his protest and went to Bingley Magistrates Court and tried to get an arrest warrant for me. The magistrate refused. He tried to be heard at the inquest and the coroner refused to allow this.
AFTERMATH
For the hospital and staff, that was the end of the attention and the protests. Mr and Mrs Bland were contacted via the hospital by people with relatives in PVS, and they met or phoned as many as they could. Requests to give talks and lectures and take part in debates kept me busy for a while. Those that I accepted were interesting and sometimes hard work, especially one at Edinburgh Medical school with a leading “pro-life” protester, Peggy Norris. We debated the whole business of treatment withdrawal. She lost, as her “look at the Nazis” slippery slope argument was more offensive than convincing. The BBC’s Casualty team asked me to review the scripts for a story line involving a PVS patient. I made suggestions, was thanked, and thought no more about it. Months later one of the researchers called. She had watched the first scene with the vegetative patient, and did not think the actor looked like PVS as I had described it. She asked me to review the tapes, and her concerns were justified—the portrayal was hopelessly unrealistic. I was invited to attend the next two filming sessions in Bristol to advise the actor and director. The completed episodes showed what PVS looked like, and clearly illustrated the emotional, legal, and ethical problems. The attention to detail and accuracy in the production was very impressive.
The Official Solicitor’s Office asked me to report on, and then supervise the care of three vegetative patients whose relatives had applied to court for permission to withdraw treatment. The doctors involved were either unwilling to withdraw or uncertain what to do. Two of these people were well managed in nursing homes and the other died at home in the care of his parents and the district nurses.
LOOKING BACK
After more than 10 years, I look back on this whole extraordinary episode with amazement and satisfaction. The law relating to withdrawal of life prolonging treatment in PVS was clarified and guidance given for future cases, including a requirement for rehabilitation before making an application. It was affirmed that artificial nutrition and hydration are medical treatments. The Judges argued that in common law the doctrine of the sanctity of human life gave way to personal autonomy. They also concluded that existing in a vegetative state was of no benefit to Tony and implied that this was not a life worth living.
I realised the importance of letters of support, and the intrusiveness of medical equipment. Tony’s death was peaceful, and no different to other deaths in hospital. Many commentators, including senior members of the royal College of Nursing, had predicted a hideous death from “starvation”. His family were, at long last, able to mourn his death. Mr Bland asked me to read at the funeral, which was attended by hundreds of local people and some of the lawyers involved, from our team and the official solicitor’s office. The Airedale staff who cared for Tony were sad, but we were all sure it had been the right decision. The dire predictions by senior nurses, and some clergy, that the staff and the family would feel severe distress and guilt at the decision and at the manner of Tony’s “final” death (as they imagined it) did not come to pass. Did they not realise that we had looked after and still look after dying patients, and that treatment limiting decisions must be, and are made every day? At the time we all felt, and still feel, that it is an affront to human dignity to keep a body with no person in it, alive for years. Many colleagues told me that the publicity made them think more about morals in their daily work; some decided to study ethics as a result. Patients too said the case made them think, and many wanted to plan their own end of life care. It became easier for me to open such discussions and get patient wishes recorded in the medical notes. I met some famous philosophers and lawyers, and for a short time was a little bit famous myself.
THE PEOPLE INVOLVED
It would not have been possible to cope without the support, help, and protection of my secretary Jane Stafford, and the RHA press officer Bob Schofield. Colleagues at Airedale were very helpful and the whole hospital rallied round the nursing staff and rehabilitation team. But the person who deserves the most praise and admiration is Mr Bland, whose plain good sense and determination never wavered, he was never angry or difficult with our staff, and he dismissed the protestors with the comment that they clearly did not understand what they were shouting about.
AUTHOR’S NOTE
This article has been read and approved by the parents of Tony Bland who are happy for it to be published.

Tony Bland’s CT brain scan showing cortical atrophy.
Protesters outside Airdale General Hospital (reproduced with permission from the Craven Herald).

{kind=link}
{kind=link}
{kind=link}
Coronal sheet of fixed brain confirming severe cortical atrophy (kindly provided by Dr L Bridges).
Acknowledgments
I would like to thank Professor Phil Scraton, Queen’s University, Belfast, for his help in preparing the article.
Other content recommended for you
- Causes and consequences of delays in treatment-withdrawal from PVS patients: a case study of Cumbria NHS Clinical Commissioning Group v Miss S and Ors [2016] EWCOP 32
- A matter of life and death: controversy at the interface between clinical and legal decision-making in prolonged disorders of consciousness
- Judge over-rules family's wish that patient should be allowed to die
- Ethical issues in nutrition support: a view from the coalface
- Current controversies and irresolvable disagreement: the case of Vincent Lambert and the role of ‘dissensus’
- Court applications for withdrawal of artificial nutrition and hydration from patients in a permanent vegetative state: family experiences
- Mother asks court to let her brain damaged daughter die
- A matter of life and death
- Permanent loss of awareness is crucial to diagnosis of PVS
- Withdrawing clinically assisted nutrition and hydration (CANH) in patients with prolonged disorders of consciousness: is there still a role for the courts?