Article Text

Abstract
Background Studies have shown that medical students and residents believe that their ethics preparation has been inadequate for handling ethical conflicts. The objective of this study was to determine the self-perceived comfort level of medical students and residents in confronting clinical ethics issues.
Methods Clinical medical students and residents at the University of Maryland School of Medicine completed a web-based survey between September 2009 and February 2010. The survey consisted of a demographic section, questions regarding the respondents’ sense of comfort in handling a variety of clinical ethics issues, and a set of knowledge-type questions in ethics.
Results Survey respondents included 129 medical students (response rate of 40.7%) and 207 residents (response rate of 52.7%). There were only a few clinical ethics issues with which more than 70% of the respondents felt comfortable in addressing. Only a slight majority (60.8%) felt prepared, in general, to handle clinical situations involving ethics issues, and only 44.1% and 53.2% agreed that medical school and residency training, respectively, helped prepare them to handle such issues. Prior ethics training was not associated with these responses, but there was an association between the level of training (medical students vs residents) and the comfort level with many of the clinical ethics issues.
Conclusions Medical educators should include ethics educational methods within the context of real-time exposure to medical ethics dilemmas experienced by physicians-in-training.
- Clinical Ethics
- Education
- Education for Health Care Professionals
Statistics from Altmetric.com
Introduction
Medical ethics has assumed greater importance in the doctor–patient relationship during the past three decades. Consequently, there has been an increased emphasis on physicians assuming acceptable professional attitudes and obtaining the necessary skills to confront the difficult moral dilemmas that occur in patient care.1–3 No consensus, however, exists regarding content, pedagogical methods and timing of ethics education in the training years.4 ,5 Many formal medical ethics curricula teach abstract ethical principles6 and critical thinking skills needed to analyse particular ethical dilemmas,7–10 but these methods might not prepare students to handle the moral conflicts they confront on the wards or clinics. Indeed, in a study performed by Roberts and colleagues,11 medical students and residents at one academic institution perceived a need for more education directed at a range of practical ethical and professional dilemmas present during training. Similarly, other studies have shown that medical students and residents feel that their ethics education has been inadequate in preparing them to handle ethical dilemmas encountered at an end-of-life situation, and in the field of paediatrics.12–14
Other than one brief study that assessed the comfort level of paediatric residents regarding seven clinical ethics issues,13 there has not been another study assessing the comfort level of individuals across a range of training levels (eg, medical students and residents) when dealing with a broad range of practical clinical ethics issues. Accordingly, the objective of this study was to evaluate the self-perceived comfort level of medical students and residents with confronting various clinical ethics issues in their training, and the association, if any, of prior ethics education, or their level of training relating to their sense of comfort.
Methods
Study design
We performed a cross-sectional survey study between September 2009 and February 2010.
Study tool development
We developed a survey tool based on our study objectives and the previous literature.4 ,5 ,12–14 The survey consisted of several domains. The first section incorporated demographic data (gender, medical school year and residency year, and extent of prior ethics education). The second section asked participants to rate their general level of preparedness when facing ethical dilemmas, their assessment of their prior ethics education, and their need for further ethics education. The third section asked participants their self-perceived comfort levels when handling specific clinical ethical issues. Respondents were asked to rate their comfort levels on a five-part Likert Scale: 1=very uncomfortable, 2=somewhat uncomfortable, 3=uncertain, 4=somewhat comfortable, and 5=very comfortable. The last section consisted of 20 knowledge-type questions assessing common clinical scenarios involving ethical issues. We had the survey pilot-tested by members of the hospital ethics committee at the University of Maryland Medical Center (UMMC).
Study population
We recruited medical students from the 3rd and 4th year classes of the University of Maryland School of Maryland (UMSOM), and the postgraduate year (PGY), 1–6, residents at UMMC from the departments of medicine, surgery and paediatrics. Preclinical medical ethics education at the UMSOM consisted of multiple lectures scattered in between science-course blocks approximately once every 2–3 months, and small groups discussing specific ethics topics incorporated within relevant systems-based subjects. No formal ethics course existed at the UMSOM. Ethics education in the department of medicine consisted of morning report sessions once every other month, and monthly ward ethics rounds.
Survey distribution
The survey tool was distributed via a web-based survey platform: (http://www.surveymonkey.com). Potential study participants were sent an email explaining the study, along with an electronic link to the survey tool. Participants were offered an incentive consisting of a US$5.00 coffee coupon.
Statistics
We entered data into SPSS V.13.0 (Statistical Package for Social Sciences). For purposes of analysis, we collapsed the categories of ‘strongly agree’ and ‘agree’, as well as the categories of ‘strongly disagree and disagree’. We used χ2 analysis to determine the association of independent variables (gender, year of training and prior ethics training) with the dependent responses, and a logistic regression analysis to determine independent predictors of the dependent responses. The level of significance was set at p value <0.01 due to the multiple comparisons that were performed.
Ethical aspects
The institutional review board at the University of Maryland School of Medicine approved this study.
Results
We obtained 238 surveys from a sample size of 524 (overall response rate of 45.4%); 129 surveys from 317 medical students (3rd and 4th years; response rate of 40.7%); and 109 surveys from 207 residents (medicine (136), paediatric (39), and surgery (32); response rate of 52.7%). All medical students attended the UMSOM; 24 of the 109 residents were graduates of the UMSOM.
Table 1 shows the demographics data of the respondents. Regarding prior ethics training, 13.4% stated they received a formal course in ethics during their medical school training, and approximately 30% reported having had ethics instruction at least once a month in years 1 and 2, while approximately 20% and 15% reported such ethics teaching in years 3 and 4, respectively.
Characteristics of respondents (n=238)
Figure 1 shows participants’ responses regarding their general self-assessment of their preparedness to handle ethical dilemmas, and their perspectives on ethics training in medical school and residency. A slight majority (60.8%) agreed that they felt prepared to handle ethical dilemmas. Less than a majority (44%) agreed that medical school training was helpful in preparing them to handle ethics dilemmas, and 63.8% thought there should be more ethics education in medical school. A slight majority of the residents (53.2%) thought that residency training was helpful in preparing them to deal with ethical dilemmas, and a slightly higher percentage of residents (62.7%) felt a need for more ethics training in their residency training programme.
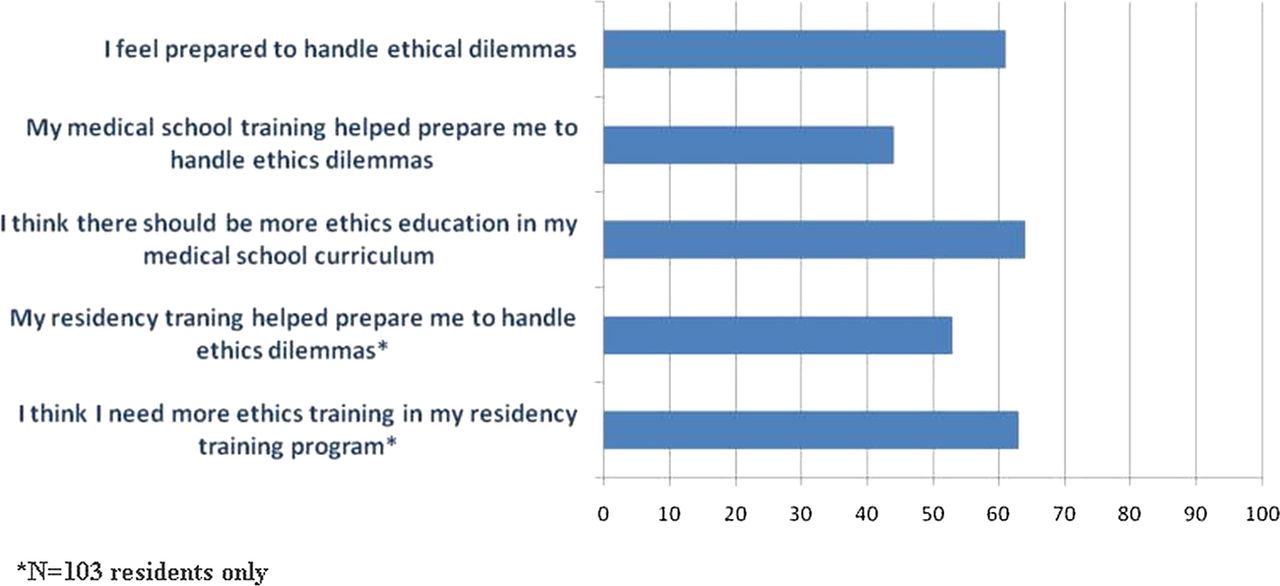
Percentage of respondents who agreed with general perspectives about their previous ethics training (n=238). This figure is only reproduced in colour in the online version.
Respondents who had a formal ethics course in medical school, and those who had ethics training at least once a month in any medical school year were significantly more likely to agree that their ethics training in medical school helped prepare them for handling ethics dilemmas compared with those with such training; (58.9% vs 36.9%, and 75.0% vs 42.3%, respectively; both p<0.01). Logistic regression analysis revealed that having ethics training at least once a month during any medical school year was a strong predictor of agreeing that medical school training helped prepare them for handling ethics dilemmas; (p<0.001; OR 5.2; 95% CI 1.99 to 13.38).
Figure 2 shows the percentage of the participants who agreed they felt comfortable in handling issues related to professional conduct and ethics issues related to professional conduct, communication issues, justice, end of life and autonomy. Participants felt most comfortable with the following issues: talking with patients who were refusing recommended treatment (74.9%); discussing advance directives (74.5%); discussing do not resuscitate orders (74.0%); breaking bad news (73.5%); understanding disparities in healthcare among different ethnic/racial groups (76.7%); recommending hospice for patients nearing death (74.4%); knowing how to obtain valid informed consent (87.8%); and dealing with patients who want to sign out ‘against medical advice’ (74.2%). Participants felt least comfortable with the following issues: dealing with an attending acting unethically (22.4%), reporting impaired colleagues (33.0%); dealing with a colleague abusing prescription drugs (33.2%); reporting colleagues who falsified information (37.8%); reporting medical errors (44.8%); resolving disagreements between family members (41.3%); and ‘knowing when to withhold information from patients based on cultural values’ (28.7%).
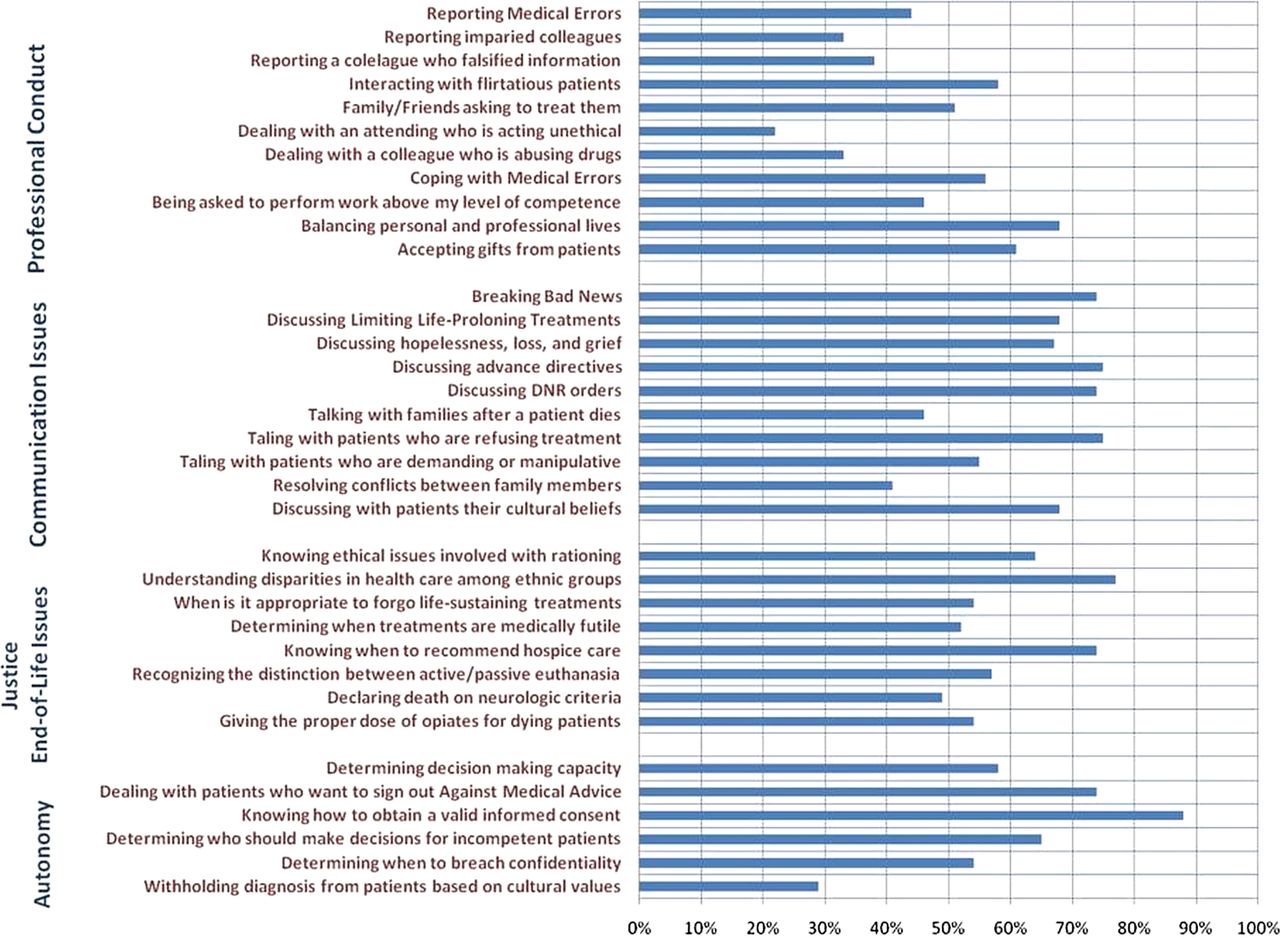
Percentage of respondents who were comfortable dealing with indicated clinical ethics issue (n=238).
Participants who had a formal ethics course in medical school, compared with those without such training, were significantly more likely to feel comfortable ‘discussing limiting life-prolonging treatments’ (78.6% vs 66.7%, p<0.01) and ‘knowing when to withhold information from patients based on cultural values’ (50.0% vs 25.6%, p<0.01). Having ethics training at least once a month during any medical school year was not associated with being more comfortable with any of these issues.
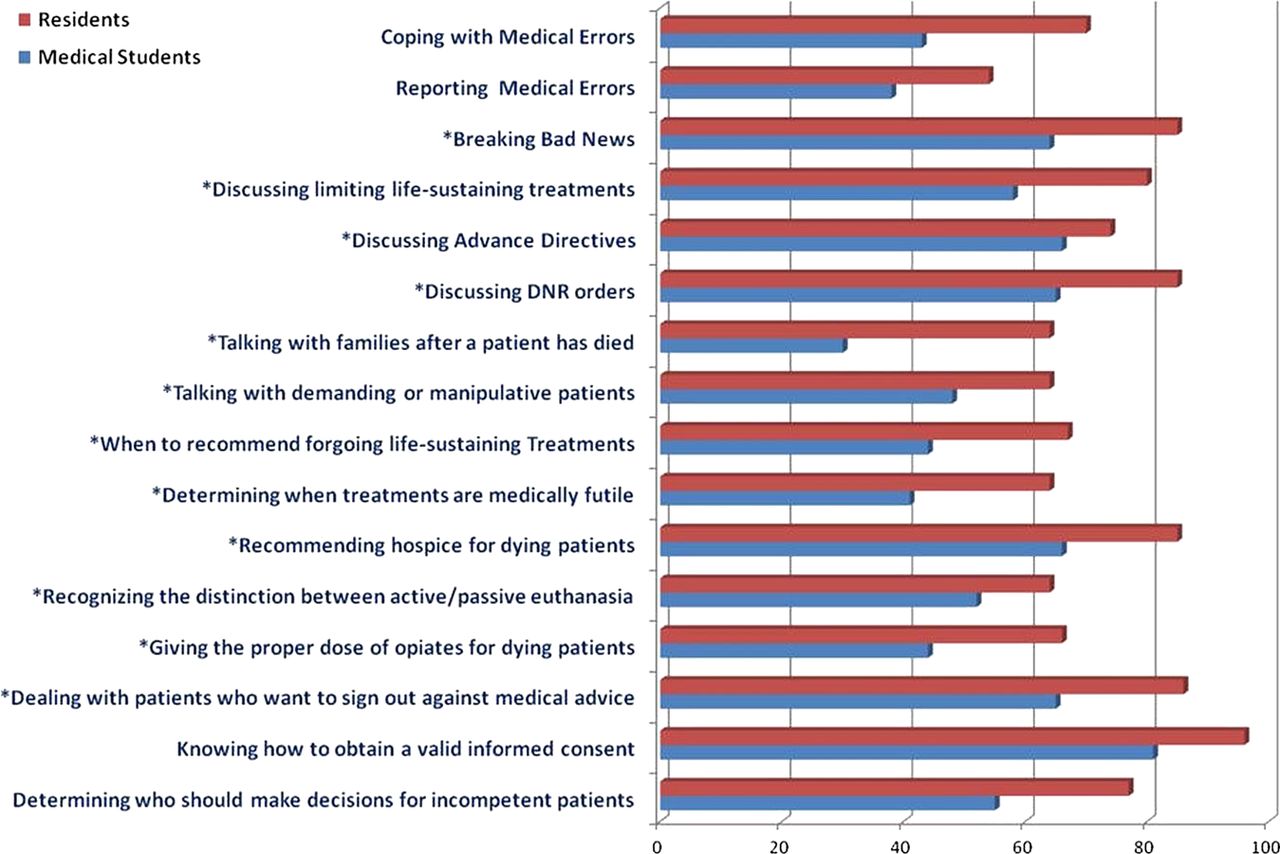
Figure 3 shows the clinical ethics issues in which residents were significantly more likely to feel comfortable in handling situations, compared with medical students. A χ2 analysis performed between the following arbitrarily defined groups (medical student year 3, medical student years 4, PGY 1, PGY 2 and PGY >3) and the dependent response variables, revealed that comfort levels with several of the clinical ethics issues progressed increasingly between these groups (p<0.01).

{kind=link}
{kind=link}
{kind=link}
Clinical ethics issues in which residents were more comfortable than medical students (p<0.01); n=238. *Ethics issues in which comfort levels progressed increasingly among the training groups (medical students and residents); p<0.01.
Regarding responses to the 20 knowledge-type questions assessing common scenarios containing ethical dilemmas in clinical practice, the mean scores (percentage correct) for the individual questions ranged from 25.6% to 90.0%; the aggregate mean correct score for all the questions was 68.6%. Residents had a higher aggregate mean correct score compared with the medical students; 72.4% vs 65.4% (p<0.01). Having had any type of prior ethics training was not associated with having a higher mean correct score on any of these knowledge-type questions.
Discussion
This cross-sectional study demonstrated that when asked regarding their comfort level in handling a broad range of clinical issues, there were only a few issues with which more than 70% of the respondents expressed feeling comfortable. Furthermore, only a slight majority of residents and clinical medical students felt prepared for handling ethics dilemmas that occurred in their clinical training experience. Our study also showed that only 44.1% and 53.2% of the respondents agreed that medical school and residency training, respectively, helped prepare them to handle such everyday clinical ethics issues. Consistent with these results was the observation that more than 60% of the respondents expressed a need for more ethics training in both the medical school curriculum and the residency training programme. Our study showed, in general, that any type of prior ethics education was not associated with respondents feeling comfortable with most of the clinical ethics issues. For a few of the clinical ethics issues, respondents who reported having a formal ethics course in medical school expressed more comfort compared with those without any such prior training.
Our study also demonstrated that residents tended to feel more comfortable than clinical medical students on many of the clinical ethics issues. Several reasons might account for residents expressing greater comfort levels compared with medical students. First, residents, compared with medical students, might have had a greater knowledge base in ethical issues. Alternatively, residents have more opportunities than medical students to participate in small-group case-based discussions, whereby residents discuss real clinical ethics encounters with their current patients.15 Finally, the difference between residents and medical students might be explained by existence of the ‘informal’ curriculum that refers to the everyday learning experiences outside formal teaching exposures.16 ,17 However, commentators have written more on the effect of the ‘informal’ curriculum on enhancing trainees’ professional development (eg, attitudes and behaviours) rather than an effect on handling clinical ethics issues.18 The optimal medical ethics training may very well depend on direct clinical exposure of trainees to ethics dilemmas, the so-called ‘experiential’ curriculum, whereby, experience gained by actually confronting these clinical ethics issues while on the wards can impart a sense of comfort with everyday ward ethics issues. What is needed then, is a curriculum that situates these clinical ethics experiences to trainees in a more systematic fashion and within a structured format, thus allowing them to more explicitly build ethical reasoning skills. Several commentators have suggested that effective preparation in ethics and professionalism will need to respond to the real-life ethical dilemmas experienced in the real world of medicine.6 ,19
Limitations in our study included a reliance on self-report of the participants; a sample size limited to a single academic teaching hospital that limits generalisability; and a moderate response rate of 45.4% that might have introduced some sampling bias. The strengths of this study included its cross-sectional design, thereby giving results across different training levels, and the comprehensiveness of the survey in examining a broad range of clinical ethical issues that trainees confront in their everyday clinical encounters.
Our data does begin to suggest that ethics training, consisting of formal instruction within the context of real-world exposure to ethical dilemmas, might improve trainees’ comfort levels when dealing with clinical ethics issues.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online table
Footnotes
-
Contributors All the authors listed contributed the following to the manuscript: conception and design, or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; final approval of the version to be published. There is no one else who has provided these contributions to the manuscript.
-
Competing interests None.
-
Ethics approval University of Maryland School of Medicine.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Other content recommended for you
- A trial of a reproductive ethics and law curriculum for obstetrics and gynaecology residents
- Ethical dilemmas encountered by small animal veterinarians: characterisation, responses, consequences and beliefs regarding euthanasia
- Croatian physicians’ and nurses’ experience with ethical issues in clinical practice
- Ethics knowledge of recent paediatric residency graduates: the role of residency ethics curricula
- What do medical students experience as moral problems during their obstetric and gynaecology clerkship?
- Is medical students' moral orientation changeable after preclinical medical education?
- Teaching medical ethics to undergraduate students in post-apartheid South Africa, 2003–2006
- Feasibility of an ethics and professionalism curriculum for faculty in obstetrics and gynecology: a pilot study
- Ethics support in clinical practice
- Teaching ethics in Europe