Article Text

Abstract
Objective: To assess the knowledge of four groups of individuals regarding who is legally authorised to consent to health care or research involving older patients.
Design: A provincewide postal survey.
Setting: Province of Quebec, Canada.
Participants: Three hundred older adults, 434 informal caregivers of cognitively impaired individuals, 98 researchers in aging and 136 members of research ethics boards (REBs).
Measurements: Knowledge was assessed through a pretested postal questionnaire comprising five vignettes that describe hypothetical situations involving an older adult who requires medical care or is solicited for research. The respondent had to identify the person who is legally authorised to provide consent.
Results: Nearly 80% of all respondents provided the correct answer when the hypothetical scenario depicted a person who was competent to consent or incompetent but legally represented. Knowledge was worse (from 2% among older adults to 44% among REB members) for the scenario describing a research situation that involved an incompetent adult without a legal guardian.
Conclusion: The observed lack of knowledge raises doubts about the ability of current legislation to truly protect the rights of older adults with diminished decision making capacity. It points to the need for educational programmes aimed at increasing public awareness of the legislation put in place for those requiring special protection.
- substituted consent
- legislation
- knowledge
- older adult
- informal caregiver
- researcher
Statistics from Altmetric.com
Respect for human dignity is a fundamental value in our society. It embodies widely adopted principles of contemporary ethics: the principles of autonomy, beneficence, non-maleficence, and distributive justice.1–5 As a moral imperative, respect for human dignity requires that healthcare practitioners and researchers secure free and informed consent from their patients or prospective research subjects before proceeding. Although aging must never be equated with incompetence, many older adults gradually lose their decision making capacity because of progressive cognitive deficits.6–8 Although proposed definitions vary slightly, decisional capacity usually implies the ability to take in, process, assimilate, and employ information regarding the risks, benefits, and alternatives to the proposed treatment or research procedures in order to reach a rational decision.9,10 Persons no longer capable of exercising informed choice are vulnerable to exploitation and deserve special legal protection.2,11–15
Legislation designed to protect and promote the rights and welfare of incompetent adults seeks to balance the preservation of autonomy, the provision of needed medical care, and a societal commitment to advance knowledge potentially beneficial to research subjects or, more likely, future patients.10,13,16–18 Such legislation varies between jurisdictions. In the province of Quebec, Canada, where this study was conducted, the rules that govern consent for a cognitively impaired individual are defined in the civil code enacted on January 1, 1994.19 According to article 15, when a person of full age is incapable of consenting to care required by his health condition, “consent is given by his mandatory, tutor or curator”. These are persons who are formally appointed by a court to represent the interests of an incapable adult. If the person is not so represented, “consent is given by his spouse, [ . . .], a close relative or a person who shows a special interest in the person of full age”. Article 12 further specifies that a person who gives his consent to health care for another individual “shall ensure that [ . . .] the risks incurred are not disproportionate to the anticipated benefit.”
Consent to research is governed by articles 20 and 21. “A person of full age who is capable of giving his consent may submit to an experiment provided that the risk incurred is not disproportionate to the benefit that can reasonably be anticipated”.19 A person who lacks the capacity to consent may also submit to an experiment, but only under strict conditions:19 1) the experiment must not involve serious risk to his health; 2) it must have the potential to produce results capable of conferring benefit to other persons in the same age category or having the same disease or handicap; 3) it must be approved and monitored by a research ethics board (REB) designated by the minister of health and social services; 4) the prospective subject’s dissent must be respected; and 5) consent to the experiment must be provided by the legal guardian of the cognitively impaired person. Hence, in contrast to health care required by the person, a family member is not authorised to make a substituted decision for research on behalf of a close relative, unless the former was formally appointed by a court to act as the prospective subject’s legal representative.
These legal provisions can only achieve their objective of protecting vulnerable populations if concerned individuals are aware of their existence and understand their implications. Such individuals include older adults who may later lose their decision making ability, informal caregivers of cognitively impaired individuals to whom practitioners and researchers often turn for a substituted consent, researchers in aging, and members of REBs. We know of no study that has examined the knowledge such people have of the rules governing consent to treatment and research. Yet there is reason to believe that their knowledge may be less than perfect. Firstly, patients and informal caregivers often confuse treatment and research, especially when the principal investigator also acts as the prospective subject’s health professional.1,12,13 Secondly, few older adults have completed advanced directives;20–23 doing so offers the opportunity to gain knowledge about current regulations that govern third party consent. Lastly, although researchers and REB members should be familiar with the laws that specify who can authorise enrolment of an incompetent individual in a research protocol, training in these matters is scarce.1,15,24
We surveyed the four groups of individuals listed above with the primary objective of assessing their knowledge of the Quebec legislation that currently governs the process of consent to treatment and research. As a secondary objective, we examined whether respondents’ knowledge varied with their sociodemographic characteristics and prior involvement in research.
METHODS
The study protocol was approved by the REB of the Sherbrooke University Geriatric Institute. Knowledge was assessed through a postal questionnaire mailed to a representative sample of each target population.

Flow chart showing the number of mailed and returned questionnaires, by study group.

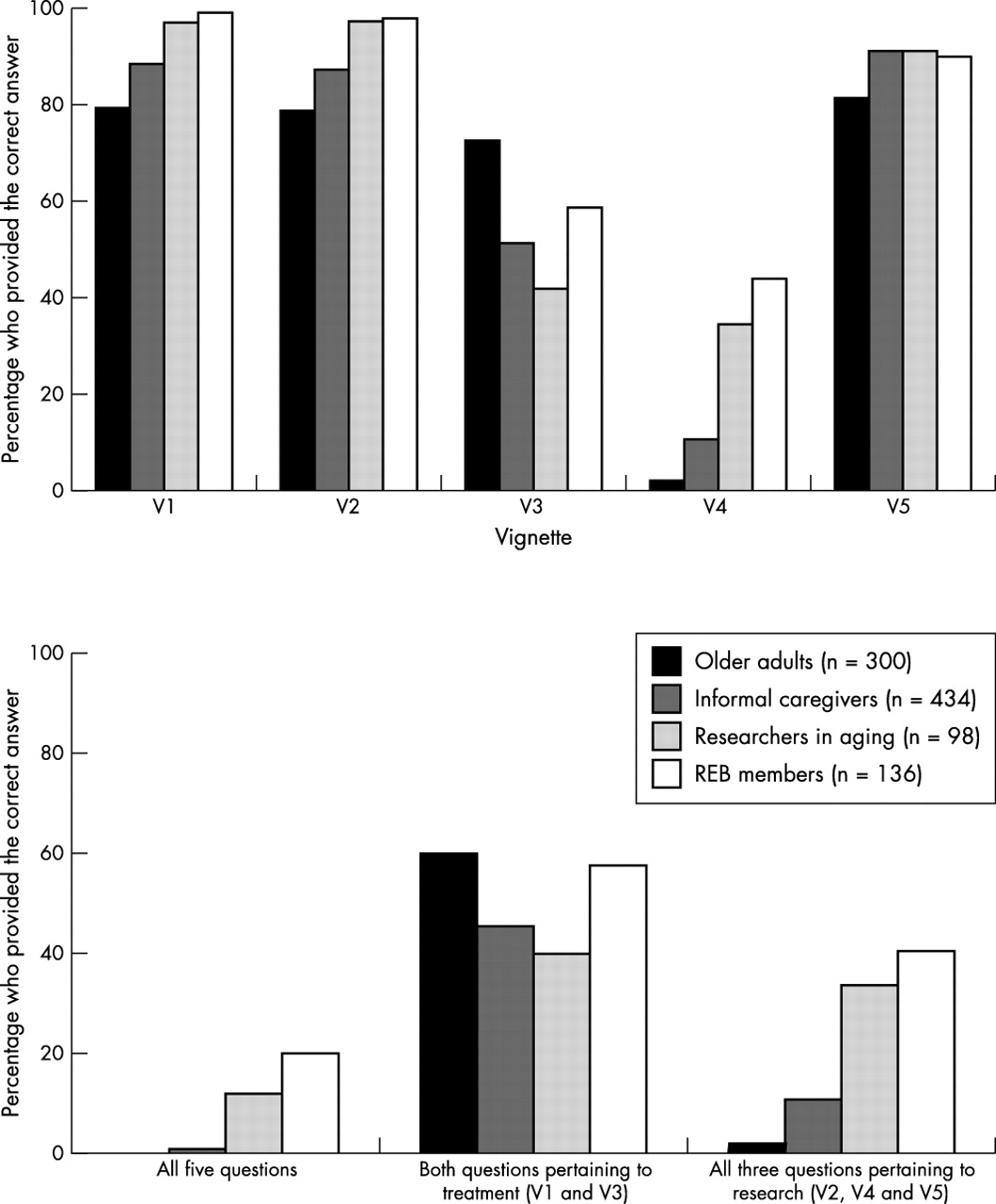
Knowledge about the person legally authorised to provide consent to treatment and research. V1, a person able to consent to treatment; V2 a person able to consent to research; V3, a person unable to consent to treatment who does not have a legal guardian; V4, a person unable to consent to research who does not have a legal guardian; and V5, a person unable to consent to research who has a legal guardian

{kind=link}
{kind=link}
{kind=link}
Sample selection
A random list containing the names, sex, and addresses of 700 adults was extracted from the provincial administrative database containing all beneficiaries of the Quebec universal health insurance plan. The sample was restricted to French speaking, community dwelling adults aged 65 and over who were presumed free of diseases affecting their ability to provide valid answers to a questionnaire. This latter criterion was operationalised by excluding any beneficiary with a diagnosis of mental illness (ICD-9, section V, codes 290 to 298, 300 to 305, 309 to 312), retardation (codes 317 to 319), or central nervous system diseases (section VI, codes 331 to 333).25
Regional Alzheimer societies and memory clinics were used to access 700 informal caregivers of persons with dementia. Each participating centre was instructed to randomly select a predetermined number of caregivers in proportion to the size of their membership or clientele. Researchers in aging were identified from the latest version of the provincial directory of public researchers. Because the number of active researchers in aging is relatively small (160 were identified), sampling was considered unnecessary and every researcher was invited to participate in the survey.
Lastly, we identified the 44 REBs designated by the minister of health and social services. These are all based in a research centre affiliated to a university or a hospital. We then excluded seven committees that exclusively reviewed research protocols involving children or teenagers. Again, because of the relatively small size of this population, we invited all 399 members of the 37 remaining committees to participate in the study.
Questionnaire
A preliminary version of the postal questionnaire was designed by the research team and examined by a committee composed of 12 experts representing the fields of bioethics, medicine, law, and research. Their comments were used to generate a revised version that was reviewed by a linguist and pretested on 4–13 subjects from each target population. Minor revisions led to the final version of the questionnaire. It comprises two main sections. Section one assesses the respondent’s knowledge of the Quebec legislation governing consent to treatment and research. This is achieved through five vignettes (see Appendix) describing hypothetical situations involving a person who requires care or whose participation in research is solicited. Following each vignette, the respondent is asked to identify the person who is legally authorised to provide consent. Section 2 collects sociodemographic information on the respondent and his/her prior experience in research or as a member of an ethics committee.
Survey
The postal survey was conducted from November 2000 to May 2001. With the objective of maximising response rates, we followed Dillman’s Design Method whenever possible.26,27 Dillman’s method consists of a set of practical suggestions that cover the design of an attractive questionnaire, the ideal number of repeated mailings and the content of each mailing. Potential respondents received a first copy of the questionnaire with a personal covering letter that explained how they were chosen, stated the objective of the survey, and underscored the importance of their participation. The first mailing also contained a self addressed stamped envelope, a letter of support from an agency credible in the eyes of the respondent, and a postcard to be returned separately from the questionnaire. The postcard, which bore the respondent’s name, served two purposes: first to identify ineligible individuals and second to identify eligible individuals who had returned the questionnaire anonymously. Space was provided on the postcard to indicate that the potential respondent did not satisfy our eligibility criteria. Two weeks later, a reminder postcard was mailed to all non-respondents. Finally, two months after the first mailing, individuals who had not returned their questionnaire received a replacement copy and a new personalised letter.
Mailings to the older adults and researchers were coordinated by the research team. In order to preserve the anonymity of their members and clients, Alzheimer societies and memory clinics preferred to manage the mailings themselves. They were provided with the required number of prepared envelopes and reminder postcards that they then distributed, by mail or in person, to the informal caregivers they had randomly chosen. The ethics committee chairs expressed the same desire. In this latter case, we forwarded the required number of questionnaires to their secretarial office, which was responsible for distributing them to their members. A reminder letter for distribution to all committee members was sent to the secretarial offices two weeks and one month later.
Analyses and sample size justification
After reporting the participation rate specific to each target population, we summarised the characteristics of the four groups of respondents using means and standard deviations or percentages. Using bar charts, we then display the percentage of correct answers for each vignette. Lastly, we present the results of multivariate (α = 0.05) logistic regression analyses for ordinal data aimed at identifying covariates linked to the respondent’s knowledge. In essence, these analyses compare the characteristics of the respondents who provided right answers to the queries with those who failed some of the questions. We started by examining one characteristic at a time, then examined simultaneously all respondents’ characteristics that were linked to the number of right answers. Multivariate analyses were restricted to the predictors that satisfied the proportional odds assumption.
Assuming a 60% response rate, we established at 700 the number of questionnaires to send to older adults and caregivers. We thus expected to analyse the responses of approximately 400 individuals from each of these two groups. A sample of that size would allow us to draw a precise picture of the respondents’ knowledge of the legislation governing consent to treatment and research. As mentioned earlier, all researchers in aging who could be identified and all members of eligible ethics committees were invited to take part in the study.
RESULTS
Figure 1 provides an overview of the final sample. Because we did not entirely control the mailing of the questionnaires to the caregivers, only 632 questionnaires were distributed, instead of the target number of 700. Potential subjects were classified as ineligible for various reasons that differed somewhat across the four groups. Ineligible older adults were either deceased, no longer living at the address we obtained, illiterate, or too ill or cognitively impaired to complete the questionnaire. Ineligible caregivers were individuals who had ceased to care for a relative suffering from dementia or health professionals who attended support groups offered by Alzheimer societies. Researchers excluded from the survey had moved outside the province, were deceased, or conducted research that did not place them in direct contact with human subjects. The six ineligible REB members were researchers in aging who had already completed the questionnaire. Following exclusion of ineligible individuals, response rates varied from 35% among ethics committee members to 75% among caregivers of persons lacking decision making abilities.
In the group of older adults, those who returned the questionnaire were younger (p = 0.005) and comprise a higher proportion of women (p = 0.003) than among non-respondents. Because little information was available on non-respondents from the other three target groups, we could not identify aspects on which they differed from those who returned the questionnaire. Characteristics of the four groups of respondents are summarised in tables 1 and 2.
Characteristics of older adults and informal caregivers
Characteristics of researchers and research ethics board (REB) members
Figure 2 shows the percentage of respondents who provided the correct answers for each vignette. Overall, high rates of appropriate answers are observed when the vignette depicts a person who is clearly competent to consent (V1 and V2) or is incompetent but legally represented (V5). Rates are much lower when the hypothetical situation involves an incompetent person who does not have a legal guardian (V3 and V4). In general, researchers and REB members knew more about the legislation that regulates the process of consent than informal caregivers who, in turn, were more knowledgeable than older adults (all ps < 0.001). Surprisingly, the inverse was observed in the case of consent to treatment required by the health condition of an incompetent person (V3). Perhaps older adults have been exposed to a similar situation more frequently in the past than members of the other three study groups.
As shown in the lower part of figure 2, very few respondents correctly answered all five questions. Roughly half provided the right answer to the two vignettes describing a treatment situation. Fewer correctly answered all three questions depicting a research situation, especially among older adults and informal caregivers.
Respondents’ characteristics independently associated with greater knowledge are reported in table 3. Within each group, few variables were found to influence the respondent’s ability to provide the correct answer, whether the scenario pertained to treatment or research. In part, this is due to the homogeneity of the responses: for many scenarios, the answers were heavily weighted in one direction or the other (see figure 2).
Respondents’ characteristics linked to better knowledge
DISCUSSION
The main objective of this study was to determine whether concerned individuals from Quebec know who is legally authorised to provide informed consent to treatment or research on behalf of a person with diminished decision making capacity. The study reveals a lack of knowledge across the four study groups in situations where a cognitively impaired person in need of care or solicited for research is not legally represented (V3 and V4). Because knowledge may vary from one country to another, our study should be replicated in other jurisdictions, using the same questionnaire to facilitate international comparisons. Future studies could also survey other groups of concerned individuals, in particular, clinicians, who are responsible for treatment and often contribute to the recruitment of research subjects. Recent studies conducted in Australia and Great Britain showed that doctors in these countries were unaware of important aspects of the law related to substituted consent.28–31
Returning to the current study, it is informative to focus attention on the respondents who failed to provide the correct answer to the third and fourth scenarios. Results show that a majority of older adults (53.2%) believed that legal consent to the care required by a cognitively impaired person could be given by the treating physician. One in five informal caregivers (20.9%) shared this view. Surprisingly, 34% of researchers and 58% of REB members wrongly thought that no one could consent to the care proposed by the clinician for an incapacitated person. The vast majority of respondents who gave the wrong answer to the fourth scenario thought that a caring family member was legally authorised to provide a substituted consent for research on behalf of a cognitively impaired relative (older adults: 85.1%; informal caregivers: 77.5%; researchers: 61.3%; REB members: 74.1%). The current legislation in Quebec prohibits enrolling mentally incapacitated individuals in research protocols if they are not legally represented. Clearly, most people are unaware of that.
These additional data suggest an alternative interpretation of our results. It is possible that we did not really measure knowledge but rather what people thought made sense. Most respondents believed that a competent person was legally authorised to accept or refuse the care proposed by a health practitioner (V1) and to decide whether he/she would participate in a research study (V2). Any other answer made little sense. Likewise, most people thought consent to research involving an incompetent person who is legally represented should be provided by the legal guardian (V5). In these three cases, their guesses coincided with the law. Unaware, however, of who is legally authorised to consent to treatment or research on behalf of an incompetent person (V3 and V4) and unwilling to tick “I don’t know”, they provided what they thought was the most sensible answer. This time, though, the law does not match their views.
Whatever the appropriate interpretation, our study raises concerns about the ability of current legislation to truly protect the most vulnerable members of society. As mentioned above, the majority of older adults, informal caregivers, and researchers thought that a caring family member could consent to research in the name of an incapacitated adult. This finding suggests that researchers likely proceed with an unauthorised proxy consent. While some may argue that a consent by a caring family member is acceptable on ethical grounds, it none the less leads to derogation of current regulations and disrespect for the legal process put in place to protect vulnerable individuals.11 Our findings also raise disturbing questions about the ability of REBs to effectively accomplish their mission of promoting and protecting the dignity, interests, and integrity of human subjects. We acknowledge that ethical approval of research protocols is based on consensual decisions among REB members. Perhaps one knowledgeable member per committee, a jurist for example, would be enough to guarantee the protection of vulnerable individuals. None the less, individual members of REBs must have a minimum amount of knowledge to make a significant contribution to the committee’s deliberations.
The concerns raised above are justified in so far as the respondents are representative of their respective populations. In general, solicited respondents who fail to return a mailed questionnaire have been shown to differ from those who respond.27 Because of a lack of information on non-respondents, which is typical of anonymous postal surveys, we were limited in our ability to detect significant differences between respondents and non-respondents. We did observe that older adult respondents were younger and included more women than non-respondents. These differences are unlikely to have biased the results as neither age nor sex was associated with knowledge, at least among adult respondents aged 65 and over (see table 3).
In comparison to other postal surveys, response rates were quite good for two of the populations surveyed—caregivers and researchers—a little low among older adults, and disappointing for the fourth group comprising REB members.27,32,33 Three reasons may explain the low response rate of the last group. First, ethics committees are known to be overburdened by the quantity and complexity of protocols they have to review.13,15,24 Second, with this group of respondents, we were unable to fully apply Dillman’s method that has been proven to maximise response rates. In particular, ethics committee members did not receive a personalised covering letter, a letter of support, and a replacement copy of the questionnaire. Last, but not least, REB members may have felt threatened by our survey, which could—and did—reveal their individual lack of knowledge regarding who is legally authorised to consent to research on incompetent individuals. If this had a significant effect on the decision to participate in the survey, then our results are overestimates and REB members’ knowledge is likely to be less than that shown in figure 2.
In conclusion, our findings underline the need to raise public awareness of the legislation that currently governs consent to treatment and research in Quebec. This statement raised another issue: who should have this responsibility? Alzheimer societies and memory clinics could assume this role with those they serve, once they have gained sufficient knowledge themselves. How can older adults be reached? Perhaps through their family physician if future surveys show that they have good knowledge of the rules governing proxy consent. Paradoxically, local ethics committees have been cited as ideal bodies to educate researchers about the ethical and legal conduct of research.13 Our results show that their members need to be better trained before they can assume an educational role in regard to researchers. It remains to be seen whether a similar need exists in other countries.
Acknowledgments
The authors thank the 12 experts who helped design the questionnaire, as well as the staff of the Alzheimer societies, memory clinics, and ethics committees for distributing the questionnaires. We also extend our deepest appreciation to the 968 individuals who took the time to answer our questionnaire. And we thank the Alzheimer Society of Canada for funding the project.
REFERENCES
Other content recommended for you
- Post-trial access to study medication: a Brazilian e-survey with major stakeholders in clinical research
- Education of ethics committee members: experiences from Croatia
- Development of a patient-centred medication management model for polymedicated home-dwelling older adults after hospital discharge: results of a mixed methods study
- Access to medical records for research purposes: varying perceptions across research ethics boards
- Attitudes of research ethics board chairs towards disclosure of research results to participants: results of a national survey
- Impact of the COVID-19 pandemic on people in need of care or support: protocol for a SARS-CoV-2 registry
- ‘The ethics approval took 20 months on a trial which was meant to help terminally ill cancer patients. In the end we had to send the funding back’: a survey of views on human research ethics reviews
- Informal caregiver support needs and burden: a survey in Lithuania
- Exploration of home care nurse’s experiences in deprescribing of medications: a qualitative descriptive study
- Optimising patient active role with a user-centred eHealth platform (CONCERTO+) in chronic diseases management: a study protocol for a pilot cluster randomised controlled trial