Article Text

Abstract
The aim of our survey was to capture the attitudes of Swedes to marginal donors and xenotransplantation. Modern biotechnology makes it possible to replace non-functioning organs, cells, and genes. Nonetheless, people may have reservations and fears about such treatments. With the survey, Attitudes of the General Public to Transplants, we have sought to expose the ambivalence that arises when medical possibilities are juxtaposed with ideas of risk. The design of the questionnaire originates from the interdisciplinary cooperation between ethnologists, medical scientists, and geneticists. By combining qualitative and quantitative methods, it is possible to illustrate the complexity that characterises people’s view of modern biomedicine. People’s reflections are based on a personal and situation bound morality, which does not necessarily coincide with what they generally consider as ethically justifiable.
- marginal donors
- xenotransplantation
- culture
- ethics
- risk
- interdisciplinary research
Statistics from Altmetric.com
The desire to replace defective body parts with functioning parts has deep roots in the history of medicine. Long before the development of modern surgery, attempts were made to transplant both from human to human and from animal to human. An early example of the latter—“xenotransplantation”—is provided by the surgeon at the end of the seventeenth century who operated on a Russian noble with a skull injury, giving him a piece of a bone from the skull of a dog.1
Modern biotechnology makes it possible to replace not just non-functioning exterior body parts with healthy ones, but also non-functioning organs and cells. As a result of progress in both surgery and immunology, transplants of human biological material are an established form of therapy today. Nonetheless, people may have reservations and fears about such treatments. At a general level, the advantages of biomedicine are often contrasted with ideas about its threatening consequences. These ideas include the worry that medical research is improperly creating new criteria by which to define what is natural and unnatural. This is particularly clear in discussions about the concept of brain death. To be able to perform a heart and lung transplant—for example, the donor must be pronounced brain dead. Yet it is not always simple to define a body whose heart is still beating as dead, even though the criterion of brain death has been applied for quite some time now.2,3
Scholars at the Department of European Ethnology at Lund University in Sweden are pursuing extensive interdisciplinary research, focusing on the interaction between medical technology, societal formation, and cultural identity.4–6 The starting point for the interdisciplinary cooperation is the insight that the issues raised by modern biomedicine require a broad spectrum of knowledge, with experiences from both “soft” and “hard” sciences. Collaboration between ethnologists, medical scientists, and geneticists has led to new questions and fruitful methodological approaches. A number of problem areas have been identified and tackled. One of these concerns the complicated feelings aroused by transplantation technology. Within this framework we have sought to expose the ambivalence that arises when medical possibilities are juxtaposed with ideas of risk. The research group’s discussions of these topics have resulted in the survey Attitudes of the General Public to Transplants.7
THE SURVEY: ATTITUDES OF THE GENERAL PUBLIC TO TRANSPLANTS
In 2001 the research group initiated a study focusing on members of the general public in Sweden. Through a Swedish institute for public opinion surveys called SIFO Research & Consulting AB, 1000 randomly selected individuals aged 15 and upwards were interviewed by telephone. Seven questions were put within the framework of a nationwide so called telephone omnibus, a telephone survey that SIFO Research & Consulting AB runs Monday to Thursday every week, and through which the interviewees are confronted with an aggregate of questions relating to a large number of subjects and to the different clients of the institute.7,8
The main aim was to capture the attitudes of ordinary people to transplants of organs, cells, and genes from human to human and from animal to human. The focus was on transplantation as a treatment method, but the study also sought to capture opinions about the research itself. Yet another aim was to investigate the situation in Sweden as a follow up to some questions in the EU barometer published in 1998, Biotechnology in the Public Sphere: A European Sourcebook. That survey was conducted in 1996, reflecting what the general public in Europe thought about a number of phenomena in biotechnology.9
The questions put to the informants in our survey were formulated on the basis of the research group’s experiences of combining humanistic and scientific/medical hypotheses. They were based both on the ethnologists’ in depth interviews, which provided knowledge about individuals’ outlooks, and on the medical and genetic scientists’ everyday experiences of the biomedical field. In contrast to earlier studies by the research group, Attitudes of the General Public to Transplants has been carried out using primarily quantitative methods. This attitude survey comes from a need to supply the insights of the in depth interviews done earlier with wide empirical material. Our starting point is that statistical data primarily mediate principal viewpoints, while a culture analytical method gives an understanding both of principles and of specific viewpoints connected to the life situation of individual persons.
Our study centred on transplants, with the focus on both moral approval and the acceptance of risk. By “moral” acceptance we allude to that process where people relate to ethical principles, that is, their personal view of the prevailing norms. Acceptance of “risk” refers to both medical and existential risks. The seven questions proceed from a relatively familiar topic—organ transplants—to methods in biotechnology which, because of their experimental nature—xenotransplants and gene therapy—are less well known and problematic. The last question tries to capture the attitude of the general public to the growing commercial trend in Swedish (and European) research.
Each question, with the exception of number 7, was supplemented with one or two sentences of an explanatory character. For the question on marginal donors—for example, the informants were told that the method was a consequence of the current shortage of organs and that organs from older donors may be expected to have a shorter functional life than organs from younger people.
The answers to the questions were first processed by SIFO Research & Consulting AB, on the basis of (1) a certain number of response alternatives, which can be identified in the text below, and (2) the variables gender, age, occupation, trade union membership, place of residence, and political affiliation.7
In this first presentation of Attitudes of the General Public to Transplants we provide a general analysis of the survey. We have chosen to emphasise the questions about allo- and xenotransplants, while the other questions are considered more briefly. Furthermore, we have decided not to give account of the tabular report of the survey. Those percentages that are given below represent, however, statistically significant deviations within the total. The margin of error for a percentage of 50% has been estimated at ±3.1%.
Use of and information about organs from marginal donors (questions 1–2)
A number of studies have examined people’s general attitudes to transplants.10–12 Question 1 in our survey sought to examine one particular problem with transplants. In today’s transplantation work there is a serious shortage of human transplants. One way to counteract this situation is to use marginal donors, in other words, to transplant less viable organs from older persons.
It turned out that three out of four respondents thought the use of organs from older donors was morally acceptable. Men were generally more positive than women: 80% of the men, compared with 70% of the women, considered it morally acceptable to use organs that could be expected to be less viable. The weakest support for marginal donors came from women aged 65 and over; only 53% of them thought the use of organs from marginal donors was morally acceptable. Surprisingly, women aged between 30 and 49 were the most positive category of all those investigated as regards gender and age. Their degree of acceptance (85%) is thus higher than that of men in general (80%) and of men aged between 30 and 49 (82%). The following questions were put to start with:
Question 1*
We turn now to transplants of organs and cells to sick people. There is a general shortage of organs today. In order that more patients can receive transplants it has therefore been considered necessary to use organs from older donors, even though these organs may be expected to function for a shorter time than organs from young donors. Do you think that it is morally acceptable to transplant organs with a shorter expected functional life, or do you think that it is morally unacceptable?
Choose one of these alternatives:
-
I think it is morally acceptable to use organs from older donors
-
I do NOT think it is morally acceptable to use organs from older donors
-
Uncertain, don’t know
-
I cannot answer the question.
Question 2 was about the information given to a patient about the expected functional life of an offered organ. It was found that there was great agreement about the importance of knowing this. More than half of the respondents thought it was very important to receive this information, and one in four considered it fairly important. Age was a decisive factor here: the younger the respondents, the more importance they ascribed to the expected functional life of the organ. Men (73%) and women (73%) aged between 15 and 29 were thus those who most valued or found it very important to have information about the viability of the organ, while women (42%) and men (44%) aged 65 and over attached the least importance to it.
Question 2
Organs for transplantation may have different expected viability, depending on the age of the donor and other factors. How important do you think it is that the recipient of the organ should be informed IN ADVANCE that the offered organ has a shorter expected functional life, so that they can give their consent?
Choose one of these alternatives:
-
Very important
-
Quite important
-
It makes no difference
-
Not very important
-
Not at all important
-
Uncertain, don’t know
-
Cannot answer the question.
The class pattern that can be discerned in the responses to questions 1 and 2 indicates that members of blue collar unions (LO) have a more critical attitude to marginal donors than do members of white collar unions (TCO) and professional unions (SACO). The SACO members (67%) were also those who attached the greatest importance to information about marginal donors. As regards the respondents’ political sympathies, it is striking that people who said they would vote for the Green Party (77%) and the Left Party (66%) stressed more than others the importance of information about marginal donors.
Research on xenotransplantation (questions 3–4)
Questions 3 and 4 in the survey were also based on the shortage of human organs. Question 3 provided information about ongoing research in xenotransplantation, that is, the transplantation of genetically modified organs and cells from animals to sick humans. This could perhaps relieve today’s grave shortage of organs or cure serious diseases such as Parkinson’s and diabetes. The subjects were asked whether they found it morally acceptable to carry out research and develop these transplants of organs and cells from animals to humans.
The majority of the respondents found xenotransplants morally acceptable. Compared with the acceptance of marginal donors, however, the degree of acceptance fell from three out of four to two out of three. In the responses to question 3 there was once again a dividing line between the sexes. Among the men, three out of four (74%) were prepared to accept it, against three out of five (58%) women. An interesting difference is that men between 30 and 49 (27%) showed less acceptance than men of other ages. Generally speaking, it can also be observed that people aged between 30 and 49 (29%) were much more negatively disposed to xenotransplants than other age categories.
Question 3
If genetically modified organs and cells from ANIMALS could be used for transplants to sick people it would solve the current shortage of organs or cure serious diseases such as Parkinson’s and diabetes. Do you think that it is morally acceptable to research and develop these transplants of organs and cells from animals to humans, or do you think that it is morally unacceptable?
Choose one of these alternatives:
-
I think it is morally acceptable
-
I do NOT think it is morally acceptable
-
Uncertain, don’t know
-
I cannot answer the question.
Question 4 was put to the 753 people who had given an answer other than “not morally acceptable” to question 3. The question is about the risks that may be associated with xenotransplants. The respondents were told that viruses in the animal’s genes could be transferred to humans via genetically modified animal transplants. These viruses could possibly give rise to new, previously unknown, and perhaps incurable diseases. The subjects were asked whether they considered it morally acceptable, despite this risk, to develop the technology by means of experiments on humans.
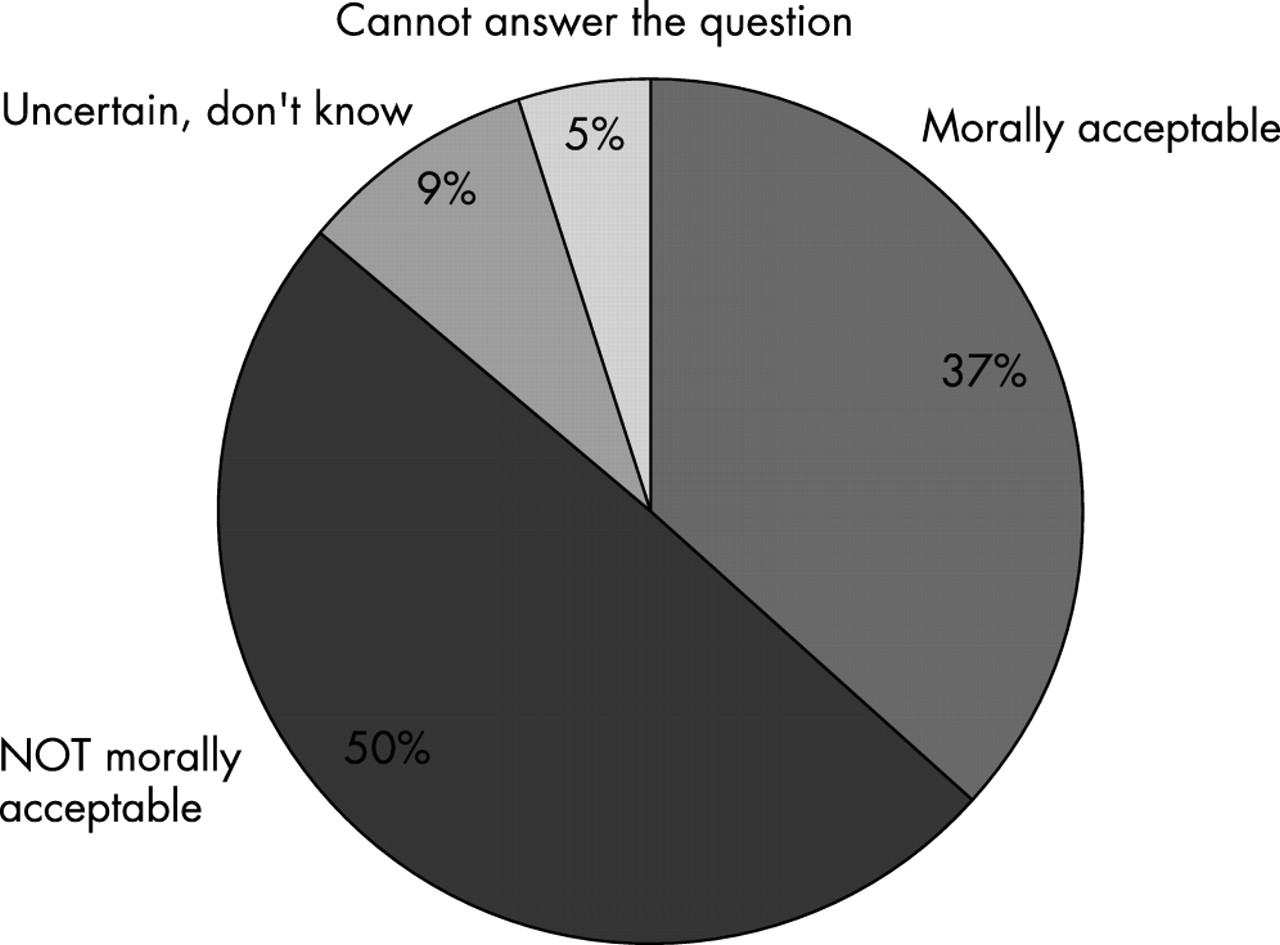
Just over a third were positive here, while half of all those who had not been against xenotransplantation in the previous questions were now opposed. Women (58%) ascribed more importance to the risk than men did (42%). Generally speaking, young people were more inclined to take risks than older people. This pattern is clearest among young men aged between 15 and 29: 57% of them found xenotransplants morally acceptable, despite the risk.
Question 4. If you answered 1, 3, or 4 to the previous question:
It has been shown that there is a risk that a kind of virus found in animals’ genes can be transferred to humans via genetically modified organs and cells from animals. These viruses could POSSIBLY give rise to new, previously unknown, and perhaps incurable diseases. Do you think that it is morally acceptable to develop this technique, despite the risk, by means of experiments on humans, or do you think that it is morally unacceptable?
Choose one of these alternatives:
-
I think it is morally acceptable
-
I do NOT think it is morally acceptable
-
Uncertain, don’t know
-
I cannot answer the question.
As with the answers to questions 1 and 2, it is possible to discern a class pattern when it comes to the attitudes of Swedes to xenotransplantation. It is striking, for example, that it is primarily respondents with links to the countryside and to LO who express a critical attitude to xenotransplantation. Of rural respondents, 31% did not find xenotransplantation morally acceptable. And when xenotransplants were made into a risk issue (question 4), the phenomenon lost support chiefly among LO members (58%) and people who vote Social Democrat (56%). Conservative voters (72%) also distinguish themselves by being those who most frequently said xenotransplantation was morally acceptable. At the same time, members of SACO (10%) were distinctive in the relatively high frequency with which they answered “Uncertain, don’t know” to question 3 about whether xenotransplantation was morally acceptable.
Research on gene therapy (questions 5–6)
Question 5 dealt with a different type of transplantation, gene therapy. The respondents were given a description of the possibility of treating diseases such as cancer by inserting new human genetic material into the patient’s own cells, in the form of healthy genes cultured in the laboratory.
Question 5
Gene therapy is a method that involves treating diseases such as cancer by implanting new HUMAN genes in the patient’s own cells. Healthy human genes, cultured in the laboratory, can thus be TRANSPLANTED to the sick individual’s cells. Do you think that it is morally acceptable to pursue research and development in gene therapy, or do you think that it is morally unacceptable?
Choose one of these alternatives:
-
I think it is morally acceptable
-
I do NOT think it is morally acceptable
-
Uncertain, don’t know
-
I cannot answer the question.
Here, once again, a clear majority of the respondents could accept the method. And again, men accepted these transplants (80%) more than women (63%). Women under 50, however, proved to be almost as positive to gene therapy as men in general. On the whole, subjects under 50 were more liable to accept the method than those aged 50 or over.
In question 6 the 838 people who had given an answer other than “not morally acceptable” to the preceding question were confronted with the information that gene therapy, like xenotransplantation, can have serious side effects. It has been found that there is a risk of medical side effects which can lead to death—for example, through inflammatory reactions. The question was whether it was considered morally acceptable to develop the technique despite this risk.
Question 6. If you answered 1, 3, or 4 to the previous question:
In gene therapy it has been shown that there is a risk of medical side effects, possibly resulting in death—for example, in the event of inflammatory reactions. Do you think that it is morally acceptable to develop this technique, despite the risk?
Choose one of these alternatives:
-
I think it is morally acceptable
-
I do NOT think it is morally acceptable
-
Uncertain, don’t know
-
I cannot answer the question.
Despite potential risks, a majority of subjects still thought it morally acceptable to continue to develop gene therapy as a medical treatment method. As before, the difference between men (67%) and women (52%) is significant. At the same time, women aged between 30 and 49 (64%) accepted this almost as much as men in general.
Like the questions about xenotransplantation, the questions on gene therapy show that the positive attitude to research has taken root among white collar workers and members of TCO and SACO more than among blue collar workers and LO members. Among Social Democratic voters, only 54% would accept the continuation of research in gene therapy despite the risks, which can be compared with 69% of the Conservative sympathisers.
Where should transplantation research take place? (question 7)
Question 7 concerned where transplantation research should be carried out. Should it be done on a commercial basis in biotechnology companies or in a non-commercial setting at universities and hospitals?
Question 7
Do you think that medical research on transplants should be carried on in biotechnology companies—on a commercial basis—or at universities and hospitals—in an academic and mainly non-commercial setting?
Choose one of these options:
-
Preferably in biotechnology companies (on a commercial basis)
-
Preferably at universities and hospitals (in an academic setting)
-
Both
-
Neither
-
It makes no difference
-
Uncertain, don’t know
-
I cannot answer the question.
Here, in contrast to previous responses in the survey, men and women showed relative agreement. A clear majority wanted this type of research to be done in the academic world. The strongest support for the academic world came from people aged between 30 and 49 (84%) and people between 50 and 64 (82%). Less conviction about the advantages of the academic environment was shown by people between 15 and 29 (68%) and people aged 65 and over (68%). The latter categories, however, did not express any great support for biotechnology companies; instead they chose the more diffuse alternatives “Neither”, “It makes no difference”, “Uncertain, don’t know”, and “I cannot answer the question”.
The academic environment at universities and hospitals also received less support among SACO members (69%) and city dwellers (72%). One SACO member in six (17%) and one city dweller in seven (14%) would also give priority to a development that leaves room for both biotechnology companies and universities/hospitals. The response option “Both” also attracted a relatively large number of sympathisers of the Greens (21%) and the Conservatives (17%), while relatively few Left Party sympathisers chose this answer (4%). Left Party voters instead distinguished themselves by being those who were most in favour (91%) of universities and hospitals as a research environment.
DISCUSSION
Transplants from human to human
According to new Swedish legislation on the strengthening of patient influence, patients have a right to information about the benefits and risks of a particular treatment.13 Medical therapies such as transplants must be based on informed consent. The amount and type of information, however, is not wholly unambiguous. Partly because of the diffuse guidelines, transplantation clinics in Sweden follow different practice as regards marginal donors. Some clinics inform the patients of the expected functional life of the organs, while others do not. It is not just in the hospitals, however, that there is disagreement. The Swedish National Board of Health and Welfare also finds it difficult to take a clear stance, having, for instance, criticised clinics where patients have been informed.14 The lack of uniform principles has consequences for patients who need a new organ. It is therefore not surprising that the Swedish patient organisations are perplexed about the rules that ought to apply. The National Patient Organisation has opposed the practice of informing patients about the viability of the organ, while certain local branches have been in favour of this.14
Our survey indicates a similar picture. As in the patient organisations, the general public does not have an unambiguous outlook as regards moral approval and acceptance of risk. Although the majority accept marginal donors, they do not do so unreservedly. Four out of five respondents (83%) think it is important to receive information about the expected functional life of the organ. This suggests that an older person’s organ is not accepted unconditionally. Most people want the opportunity to know what type of organ is to be inserted in the body and also to take a stance as to whether the organ should be transplanted at all.
The fact that not everyone shares the same opinion is particularly evident if one takes the age factor into account. People aged 65 and over are most critical of marginal donors, especially women aged 65 and over. Similarly, the otherwise risk prone young people between 15 and 29 stand out as those most anxious to have advance information about the expected viability of an organ.
To arrive at an understanding of these disagreements and ambivalences it is necessary, as previous studies in the research group have shown, to analyse values in a qualitative and contextual manner.6 When people in long conversational interviews reflect on biomedicine, their answers are more complex than when a questionnaire is used. For example, people who are not directly affected by kidney failure may find it easier to speak in normative terms, about how things ought to be. In contrast, people who have family members or relatives with kidney problems or who undergo dialysis themselves, speak with a kind of personal pragmatism, proceeding from what would be best for themselves. Situation bound attitudes like this explain why the general public can be unsympathetic towards treatments which seriously ill people might advocate, or why younger people more than old people think it is important to have information about the expected life of an organ: young people are—or think they are—in greater need than others of organs with a very long duration. People’s reflections are thus based on a personal and situation bound morality—which does not necessarily coincide with what they in general consider to be ethically justifiable.15 This means also that general ethical principles should be understood contextually. In the same way that people adjust morals and ethics, there are continuous renegotiations at the societal level. An example which clearly illustrates this, which was mentioned in the introduction, is a person’s view of what is a living and what is a dead person. When heart and lung transplants were first performed in the 1960s, the need arose for a dead body with a heart that was still beating. In Sweden the old criterion, heart dead, was replaced in 1988, by a concept of brain related death.
People’s views of transplants are multifaceted, giving no unambiguous answers. One could nonetheless describe the respondents’ ambivalence about biomedical methods as a basic factor in itself. This uncertainty—hopes versus suspicions—should be seen in the light of the problematic situation that modern biomedicine in general creates. Replacing defective organs, cells, and tissues with healthy ones may be one way to gain control over one’s own body. At the same time, the transplantation procedure means that the individual is at the mercy of a structure that is difficult to influence. The question about information concerning marginal donors is one example of the difficulties that can arise when people’s longing for health is confronted with the practice of the health care system.
Xenotransplants
Previous Swedish studies of attitudes of the general public to xenotransplantation have indicated a growing acceptance of this special form of biotechnology. The 1996 EU barometer showed—for example, that there was little support for xenotransplants in Sweden. The 1008 subjects who were interviewed were asked whether they found xenotransplantation morally acceptable. The majority of Swedes (53%) thought xenotransplants were not morally acceptable, and only 12% were wholly in favour.16 Very similar figures were reported by a Swedish questionnaire study of gene technology conducted in 1997 by researchers at the Institute for Futures Studies in collaboration with the institute for public opinion surveys, SIFO Research & Consulting AB. Of the 1336 respondents, more than half (53%) disagreed in whole or part with the statement that it is right to give human genes to pigs so that the pig’s organs can be used for xenotransplantation, and only 8% fully agreed with the statement.17 At around the same time it was shown that the Swedish public’s preferences for organs of different origins (human as well as animal) follow a hierarchy in which animal organs are at the bottom. Only 40% of the Swedish public were willing to receive an animal organ, while as many as 77% were willing to accept an organ from a relative, 69% from a deceased person, and 63% an artificial organ.18,19 A much more positive attitude to xenotransplantation is presented in the 1999 report of the Swedish government’s xenotransplantation committee. A working group within the committee carried out a questionnaire study among 1000 randomly selected individuals. Of the almost 600 questionnaires that were completed and returned, 60% were in favour of the transplantation of animal kidneys. Moreover, 80% were favourably disposed to further research on xenotransplantation.20
Our survey confirms the picture of increased acceptance of xenotransplants. A majority—two out of three—of the respondents thought xenotransplants were morally acceptable. The tendency towards increased acceptance among the Swedish general public was strongest in men. Women were more doubtful about xenotransplantation. From the point of view of age, there is least acceptance among people aged between 30 and 49. This is particularly clear for men between 30 and 49, who are negative to xenotransplantation to a much greater extent than men of other ages. Opposition to xenotransplantation also seems to be more prevalent in the countryside than in the cities, and among socialist rather than non-socialist voters.
The EU barometer found that the question of risk was not of crucial significance for the attitude of the general public to biotechnology and xenotransplantation. Instead the important factors were the potential of the treatment and the moral and existential viewpoints. Another explanation for the decreased worry about risk is suggested by the EU barometer: the disqualification hypothesis. It is argued that there has been a change in the public view of medical expertise, as a result of which people suspect that scientists are unable to predict risks. This awareness—or this loss of faith in expertise—means that the risk argument is no longer credible in the public debate.21
A contradictory picture is painted by the report of the Swedish xenotransplantation committee. This found that the positive attitude to xenotransplants changes drastically when the respondent is confronted with greater uncertainty concerning the results of the treatment and, what is crucial here, risks of infection.22 Understanding the risk factor in general is also given great priority in the Swedish report.23 This lack of agreement between the EU barometer and the Swedish xenotransplantation committee may be surprising, but it can be understood in the light of the fact that animal infection became a burning issue in the public debate in the interval between the two studies. Besides alarms about humans being exposed to virus infections from cows and birds, it was confirmed that the pig’s endogenous retrovirus can infect human cells in vitro.24 All in all, this meant that xenotransplantation was transformed into a risk issue to an extent not known before.
Our survey, paradoxically, confirms both the EU barometer’s and the Swedish xenotransplantation committee’s stance on the concept of risk. On the one hand, one can say that, as in the EU barometer, many of our respondents express a kind of disqualification of the risk argument. Not even when xenotransplantation is associated with risk (question 4) do the respondents reject it as firmly as people did a few years ago. When the question of risk is introduced, as many as 37% of the subjects are still prepared to accept that scientists continue to develop the method. Transplantations and biotechnology have had a long period during which people’s attention has been focused on particular sensational events, such as when Christiaan Barnard performed the first heart transplant in 1967, when Baby Fae was given a baboon heart in 1984, or when Dolly, the cloned sheep, was born in 1997. Further developments of achievements such as these lead to much less discussion. Nevertheless, the probable consequence of this concentration on events—as a confirmation of the greater potential of transplantation technology and the growing therapeutic importance of animals in medicine—has been that the level of acceptance has risen because more people are willing to go further. On an unconscious level, there has been a cultural integration of xenotransplantation.
On the other hand, in agreement with what the Swedish xenotransplantation committee claims, the Swedish public still seem to be sensitive to risk and uncertainty. When the question of xenotransplantation is associated with risk, half of the respondents, who initially had not repudiated xenotransplantation, thought the technology was no longer morally acceptable. It thus seems as if the Swedish public is still strongly affected by the virus scare about xenotransplants that arose towards the end of the 1990s.
It should be stressed that the questions in the different surveys and in our own survey were not identical. In addition, the surveys have partly differed in their thematic orientation. The EU barometer and the Institute for Futures Studies’ survey focused on experimental research and the right of humans to intervene in nature. Our survey also aimed to capture views of frontline research but, like the survey by the Swedish xenotransplantation committee,25 it mainly proceeded from a patient perspective. The focus on diseases and the shortage of organs, for example, probably contributed to the relatively positive attitude among the respondents.
The latter considerations should make us exercise caution when it comes to drawing conclusions about the increased acceptance. Instead of talking about a change of trend in a certain direction, it may be wiser to emphasise the powerful formation process which we are in the midst of. Whether people answer yes or no to questions and statements should not be taken to lead to any apparently self evident conclusions; subtle factors are always involved, such as how questions and statements are formulated and presented, and the response alternatives that are given.3,26 Despite this, the wealth of variation in how and what people answer has less to do with methodological inconsistency or incompetence and more to do with what the actual situation is like at present. There is no real shared standpoint; people’s opinions vary over time and in different contexts. This heterogeneity in the results obtained has also been obvious when authors have compared the many attitude surveys on xenotransplantation conducted in the last 10 years in North America, Australia, and Europe.27,28
Attitudes and quantitative and qualitative studies
Our research group at the Department of European Ethnology in Lund has carried out several studies on the interaction between medical technology, societal formation, and cultural identity. Central aims in these culture analytical studies have been to examine the often ambivalent feelings to which biomedicine gives rise. Primarily qualitative in depth interviews have been done for the purpose of showing people’s views on medical therapies or clinical experiments which maintain or “create” life. One study has been about the transfer of eggs and sperm between people, that is, artificial insemination.5 Other studies have focused on renal transplantation, the transmission of brain cells from aborted fetuses to patients who suffer from Parkinson’s disease, and xenotransplantation as a possible remedy for diabetes. The individuals being interviewed in these studies have all had personal experience of the above mentioned treatments—patients, relatives, medical personnel, and scientists. These in depth interviews have shown that people’s attitudes to biotechnology are complex and that it is worthwhile to analyse them from several perspectives.
In this first presentation of Attitudes of the General Public to Transplants we have chosen to examine the Swedish institute for public surveys, SIFO Research & Consulting AB’s, data in the light of our earlier scientific results. This approach means that, when we—for example, analyse the current data which shows an increased acceptance for xenotransplantation, these results can be confirmed by our in depth interviews. Moreover, it is possible, from a culture analytical perspective, to explain the origin of that acceptance. That is, to demonstrate the integration process whereby the unknown—in the shape of xenotransplantations—is incorporated into people’s consciousness and worldview. By combining different methodological perspectives in this way, it is possible to shed light on both the complexity and the ambivalence that characterise people’s view of modern biomedicine.
Interviews with 1000 randomly selected individuals aged 15 and upwards
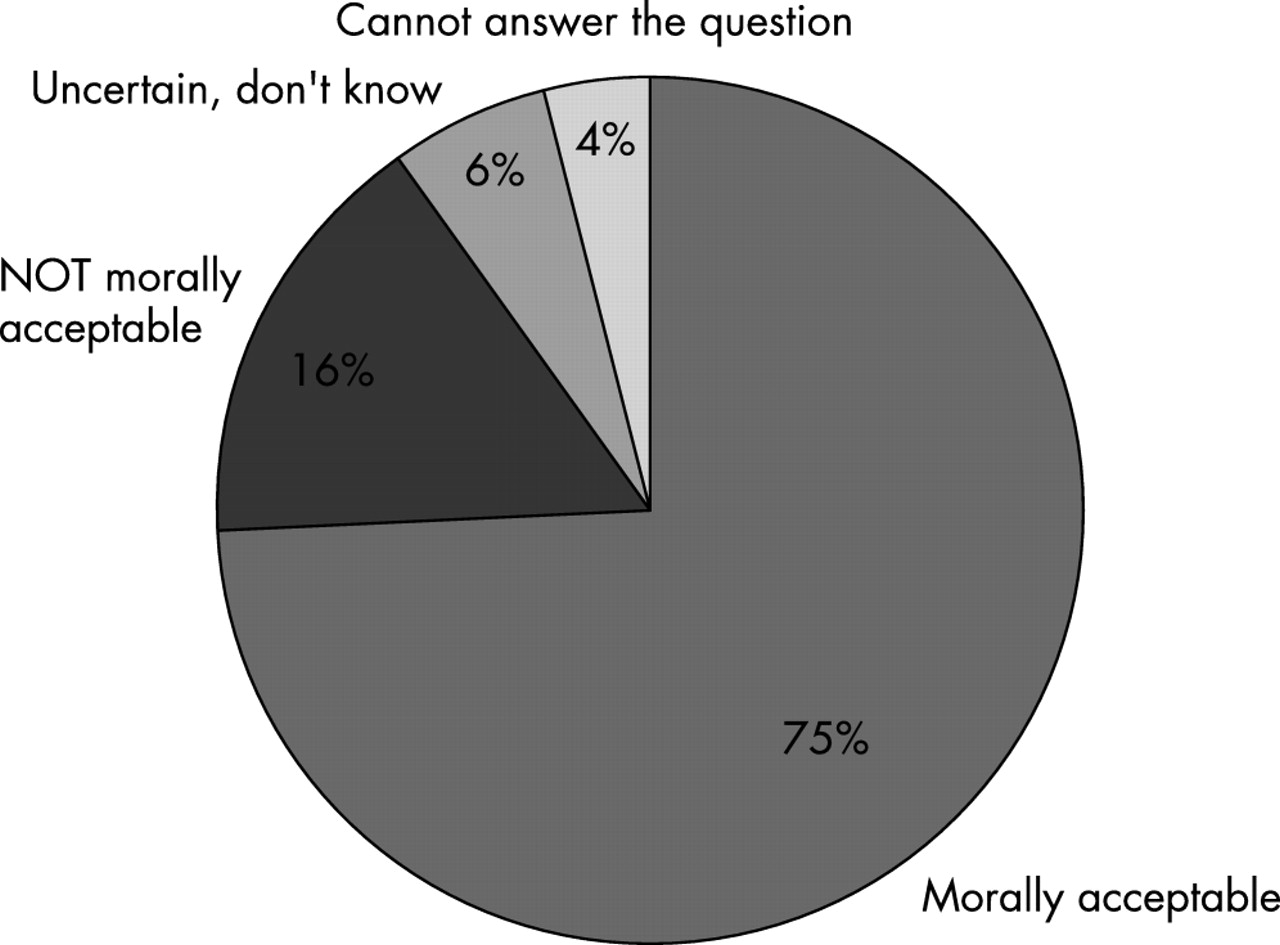
Do you think that it is morally acceptable to transplant organs with a shorter expected functional life? (Question 1) Distribution of responses to question 1: total group (n = 1000).

How important do you think it is that the recipient of the organ should be informed that the organ has a shorter expected functional life? (Queston 2) Distribution of responses to question 2: total group (n = 1000).
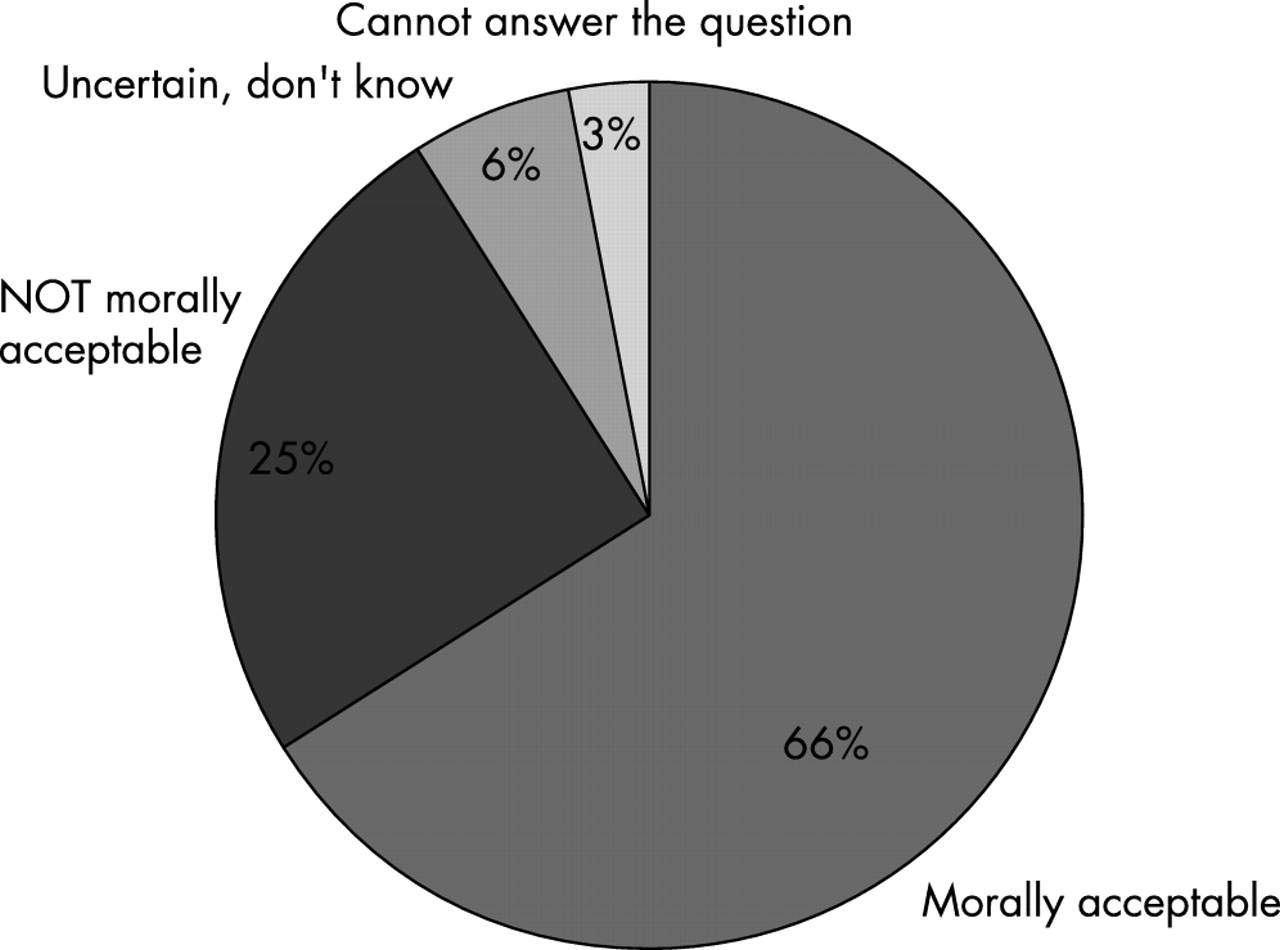
Do you think that it is morally acceptable to research and develop transplants of organs and cells from animals to humans? (Question 3) Distribution of responses to question 3: total group (n =1000).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Do you think that it is morally acceptable to develop this technique, despite the risk, by means of experiments on humans? (Question 4) Distribution of responses to question 4: total group (n = 753).
Acknowledgments
The authors thank Associate Professor Nils H Persson and Phil Dr Marie Omnell-Persson at the Department of Nephrology and Transplantation, Malmö University Hospital, and Associate Professor Lynn Åkesson at the Department of European Ethnology, Lund University, for their comments. Thanks also to Associate Professor Annika Tibell and Professor Emeritus Carl-Gustav Groth at the Department of Transplantation Surgery at Huddinge University Hospital/Karolinska Institute, and to Gunilla Sparell at SIFO Research & Consulting AB who was project leader for the survey “Attitudes of the General Public to Transplants”. Support was provided by the Bank of Sweden Tercentenary Foundation, the Juvenile Diabetes Foundation/the Knut, and Alice Wallenberg Foundation, the Lennart Jacobsson Foundation, Centre for European Studies at Lund University and the Council for Research in the Humanities and Social Sciences.
Footnotes
-
↵* Questions 1–7 are taken from the survey.
Other content recommended for you
- Starting clinical trials of xenotransplantation—reflections on the ethics of the early phase
- The donor lung: conservation of a precious resource
- Objective assessment of criteria for selection of donor lungs suitable for transplantation
- Genetic disenhancement and xenotransplantation: diminishing pigs’ capacity to experience suffering through genetic engineering
- Does it matter that organ donors are not dead? Ethical and policy implications
- Xenotransplantation: a bioethical evaluation
- Sham neurosurgery in patients with Parkinson's disease: is it morally acceptable?
- PreImplantation Trial of Histopathology In renal Allografts (PITHIA): a stepped-wedge cluster randomised controlled trial protocol
- “One man’s trash is another man’s treasure”: exploring economic and moral subtexts of the “organ shortage” problem in public views on organ donation
- Viability testing and transplantation of marginal livers (VITTAL) using normothermic machine perfusion: study protocol for an open-label, non-randomised, prospective, single-arm trial